
Abstract
Background
Peer-assisted learning (PAL) has been increasingly adopted in undergraduate medical education as a strategy to enhance the acquisition of clinical skills. Its potential to promote collaborative learning, cost-effectiveness, and professional development makes it an attractive pedagogical approach. However, the evidence surrounding its implementation and outcomes in clinical skills teaching remains scattered.
Methods
We conducted a scoping review following the PRISMA-ScR guidelines to map the extent, range, and nature of the literature on PAL in undergraduate clinical skills education. Relevant studies were identified through searches of PubMed, Scopus, Web of Science, and ERIC from inception to 17 September 2024. Articles were included if they examined PAL interventions involving undergraduate medical students in clinical skills training. Data were extracted on study characteristics, implementation strategies, outcomes, and reported challenges.
Results
A total of 95 studies met the inclusion criteria. PAL was applied across a range of clinical skills including history taking, physical examination, procedural skills, and communication training. Reported benefits included improved student confidence, enhanced skill acquisition, and positive perceptions of peer tutors and learners. Challenges included variability in tutor training, assessment methods, and sustainability of programs. Evidence gaps were noted in long-term outcomes and standardization of evaluation tools.
Conclusions
PAL is a valuable educational approach for teaching clinical skills in undergraduate medical education, with benefits for both tutors and learners. Further research is needed to establish standardized frameworks, assess long-term impact, and guide integration into formal curricula.
Keywords
Introduction
Peer-assisted learning (PAL) has been defined as “people from similar social groupings who are not professional teachers helping each other to learn and learning themselves by teaching”. 1 It is derived from Vygotsky's social constructivist theory of learning which emphasizes that the knowledge synthesized in the mind of the learner interplays with the external community in which the learning process is happening. 2 Stemming from this theory, the theory of “cognitive congruence” hypothesized that the more the tutors and learners share a common knowledge base, the better the learning outcomes will be. 3 Schmidt and Moust expanded the theory by stating that sharing a social role with the learners helps the tutor in the knowledge transfer process, they called this concept “social congruence”. 4
Since the 1990s, PAL has been incorporated into different teaching activities and disciplines with mostly positive outcomes. 5 It has demonstrated a number of benefits to student-learners, student-teachers and educational institutions. 6 Reported benefits for student-learners include increased satisfaction, reduction in anxiety in clinical encounters, more opportunities for learning, more chances for participation in clinical activities, and better development of cognitive and psychomotor skills. 7 Likewise, student-teachers benefit from PAL. Researchers have identified three reasons why medical students should learn and practice teaching skills. 8 First, they are the future doctors and faculty members who will teach the new generation. Second, they will be better educators to their patients, which improve doctor–patient relationship and lead to better patient outcomes. Third, they will be able to learn better by understanding the concepts of learning and teaching. To support the last point, evidence has shown that student–teachers gain a lot of pedagogical and professional benefits from being involved in PAL activities. 9 Such benefits include deeper understanding of the topic being taught, 10 better academic performance, 11 increased confidence, 7 enhanced self-learning skills, 12 and development of leadership qualities. 13 Teaching institutions stand to benefit from PAL as well. Evidence suggests that PAL can help address the worldwide educator shortage and reduce the teaching load on faculty. 9 Although important, it is essential not to consider these logistical concerns in isolation from the student-related outcomes of such intervention. 6
PAL has been analysed in the context of cognitive, psychomotor and affective learning outcomes. 7 The authors approached this topic from the perspective of educators engaged in undergraduate clinical skills training. One of the author's teaching experience centres on supporting junior students in developing history-taking and physical examination skills, while another author focuses on introducing surgical skills to more senior learners. Through their involvement in these activities, the authors have observed a growing interest in the potential role of PAL within clinical skills education and recognized the need for clearer evidence on how PAL has been structured, delivered, and evaluated across institutions. Thus, the specific focus of this review will be the utilization of PAL in teaching clinical skills, in which psychomotor development is the main measurable outcome. 5 Evidence indicates that PAL is particularly effective when applied to the teaching of practical skills. 14 The definition of a clinical skill that will be applied in this review is “any action, performed by a healthcare worker involved in direct patient care, which impacts on clinical outcome in a measurable way”. 15 Most published reviews on this topic focused on the outcomes and benefits of PAL.16–18 However, no identified review discussed the details of PAL-approaches, including their characteristics and the context in which they were applied.
To address this gap in the characterization of PAL-approaches within undergraduate clinical skills education, this scoping review was conducted guided by the methodological framework of Arksey and O’Malley 19 and reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. 20 In their paper, Arksey and O’Malley have identified four reasons to carry out a scoping review, namely to investigate the extent of research activity in a specific field, to summarize research findings, to analyse the possibility of running a systematic review, and to pinpoint gaps in literature. 19 This review aims to scope the literature for different PAL-approaches in the teaching of clinical skills in undergraduate medical education (UME). The main objectives will be matched to the first two reasons mentioned earlier, specifically to identify the different approaches in which PAL was applied in these studies, and to summarize the characteristics of these PAL-approaches and of the students participating in them.
Methods
This review was conducted as part of a postgraduate Master's programme at the University of Warwick. Academic approval for the study proposal was granted on 16 September 2024. There is no published protocol for this scoping review. As the study involved no interaction with human participants and relied solely on the analysis of previously published literature, it fell under the category of literature-based research. According to the University of Warwick's Research Integrity and Ethics Policy, literature-based studies that do not involve human participants, identifiable personal data, or biological samples do not require formal ethical approval 21 ; therefore, no ethical review was sought for this scoping review.
This review followed the PRISMA-ScR guidelines at every stage to ensure the quality of the reported findings.
20
Moreover, a full PRISMA-ScR checklist, including section numbers, is attached (Appendix 2).
22
It was conducted using the framework developed by Arksey and O’Malley, which has five essential steps (the “optional” sixth step will not be covered due to time constraints).
19
These are:
Step 1 (Identifying the Research Question): the research question was constructed using the Population-Concept-Context (PCC) framework.
23
The question is “how can PAL (concept) be incorporated in the teaching of clinical skills (context) for undergraduate medical students (population)?”. Step 2 (Identifying relevant studies): the search strategy was developed iteratively by the authors in consultation with an academic librarian experienced in systematic and scoping review methodology. An initial exploratory search of Medline was conducted to identify keywords and index terms commonly used to describe PAL. As no relevant Medical Subject Headings (MeSH) for PAL were identified, the final search strategy relied on a combination of free-text terms and Boolean operators. Table 1 shows the complete Boolean search string used. The same search strategy was adapted in three other databases: Web of Science, Scopus, Education Resources Information Centre (ERIC). All databases were searched from inception to 17 September 2024. The only limit applied was the availability of the full text in English. No filters were applied for study design, publication type, or publication year. All results were extracted to the synthesis review management software Rayyan for duplicate removal and blinded screening.
24
Step 3 (Study Selection): First, Rayyan software was used to detect the duplicate articles. All screening was conducted using Rayyan's blinded review and conflict-detection features. Prior to formal screening, both reviewers completed a calibration exercise by jointly reviewing a sample of articles to refine the definitions of the eligibility criteria and ensure consistent application during abstract and full-text screening. Although Rayyan facilitates blinded dual screening, it does not provide a built-in function for calculating Cohen's κ,
25
and the pre-resolution decision matrix required for such a calculation was not preserved during conflict resolution. Nonetheless, the review process incorporated two independent reviewers, systematic conflict identification, and resolution by consensus, thereby ensuring a rigorous and reproducible approach to study selection. Table 2 details the Inclusion and exclusion criteria. Only studies published as full-text articles in English were included. This decision was made to ensure adequate methodological detail and feasibility of analysis. Non-English full texts, abstracts without accessible full manuscripts, conference proceedings, theses, and other gray literature were excluded. This decision was made to ensure adequate methodological detail for data extraction and comparability across studies. For the purpose of this review, undergraduate medical students, including those undertaking clinical rotations or designated as “clinical clerks,” were considered eligible. In contrast, studies relying solely on postgraduate trainees or faculty as instructors were excluded from the review. Studies employing blended teaching models (ie students co-teaching with interns, residents, faculty or other experts) were included. Step 4 (Charting the data): a “data charting form” was used to extract the relevant details from the selected articles.
22
Extracted information was divided into three categories: literature, population, and PAL-approach characteristics, including the type of skills being taught. Outcome measures were not extracted or synthesized, as the objective of this scoping review was to map PAL-approach characteristics rather than evaluate intervention effectiveness. MS Excel, version 16.93 (Microsoft Corporation) was used to organize and chart the data.
26
Step 5 (Collating, summarising, and reporting results): the extracted data was collated and analysed under each of the three categories. A quantitative summary of important data points is presented in a table format, along with a narrative analysis. Significant findings are discussed further in the “Discussion” section.
Search Strategy.

Inclusion and Exclusion Criteria.

Results
The process of article search and selection, along with article counts, is detailed in the PRISMA-ScR flowchart (Figure 1). 20

Preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) flowchart.
Appendix 1 details all included studies, and the data extracted from them. Table 3 summarizes the publication characteristics of the 95 included studies.
Characteristics of Included Studies.

Literature Characteristics (Publication Trends)
The characteristics of the included literature, including publication year, geographic distribution, study design, and sample sizes, are summarized below. Publication dates for the included studies ranged from 2002 to August 2024. Only one study was published in each of the years 2002, 2005, and 2006 (3/95, 3.2%). After 2006, the number of publications increased steadily, reaching a peak of 11 studies in 2020 (11/95, 11.6%). A subsequent decline was observed in the following years, with 8 studies in 2021 (8/95, 8.4%), 9 in 2022 (9/95, 9.5%), and 9 in 2023 (9/95, 9.5%).
The three countries contributing the largest number of publications were Germany (23/95, 24.2%), the United States (19/95, 20%), and the United Kingdom (18/95, 18.9%). The remaining 24 countries each contributed four or fewer studies. Figure 2 summarizes the geographic distribution of studies by World Health Organization (WHO) region. 122 The European region accounted for the largest proportion of publications (55/95, 57.9%), driven predominantly by contributions from Germany and the United Kingdom, followed by the Region of the Americas (21/95, 22.1%). The Western Pacific, Eastern Mediterranean, South-East Asia, and African regions contributed 9 (9/95, 9.5%), 6 (6/95, 6.3%), 3 (3/95, 3.2%), and 1 (1/95, 1.1%) study, respectively. These figures reflect the country in which the PAL intervention was conducted rather than the location of the publishing journal.

Geographic distribution of studies by World Health Organization (WHO) region.
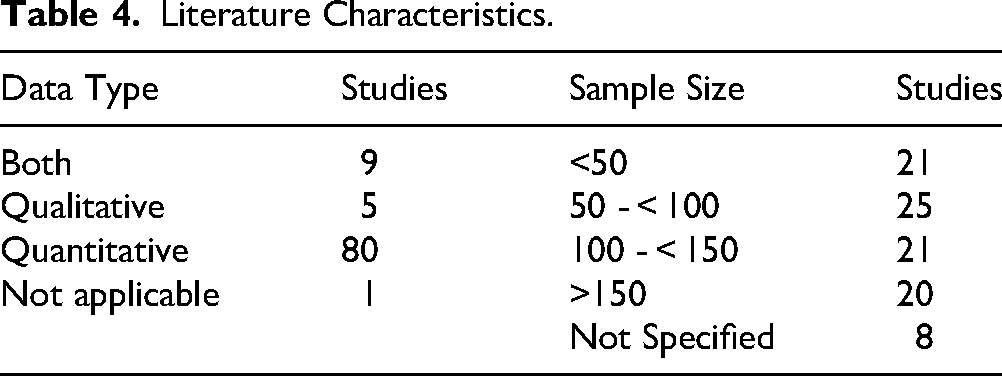
Table 4 provides an overview of the data types reported and the range of sample sizes used across the included studies. Most studies collected quantitative data (80/95, 84.2%), while only five studies (5/95, 5.3%) used a qualitative design. Nine studies employed mixed-methods approaches (9/95, 9.5%), and one study did not report collecting either qualitative or quantitative data (1/95, 1.1%). Sample sizes varied widely, with the largest cohort including 1534 participants across a five-year period. 87 The smallest sample size in a quantitative study was 14 participants.62,82 Among studies collecting quantitative data, the median sample size was 91. Of the five qualitative-only studies, three reported their sample sizes: 16, 22, and 168.29,52,91 In eight studies, sample size was not specified (8/95, 8.4%). Together, these patterns demonstrate a progressively increasing research interest in PAL for clinical skills training, with notable geographic and methodological clustering across the literature.
Literature Characteristics.
Population Characteristics
The demographic and academic characteristics of the participating students, as well as the structure of peer- and near-peer tutor involvement, are detailed in this subsection. Near-peer assisted learning, in which senior students teach more junior learners, 123 was the most common approach and was used in 56 of the included studies (56/95, 58.9%). Approaches in which tutors and learners were at the same academic level were reported in 15 studies (15/95, 15.8%), while 10 studies (10/95, 10.5%) used both models concurrently. Reciprocal PAL, where students alternate between tutor and learner roles, 9 was used in two studies (2/95, 2.1%).
Across the studies that reported tutor and learner levels, student-tutors were drawn from the three senior years of medical school (years 4-6) in 89 studies, while student-learners came from the three junior years (years 1-3) in 27 studies. These counts are not mutually exclusive, as several studies included students from more than one academic level. Figure 3 illustrates the distribution of participating students by undergraduate year, acknowledging that individual studies may contribute data to multiple levels. The specific difference in seniority between tutors and learners could be calculated in 18 studies (18/95, 18.9%). Among these 18 studies, the tutor–learner gap was one year in 10 studies (10/18, 55.6%), two years in five studies (5/18, 27.8%), three years in two studies (2/18, 11.1%), and four years in one study (1/18, 5.6%). In the remaining studies, the difference could not be determined because authors either did not specify learner levels or reported broad ranges.

Distribution of participating students by undergraduate class (learners vs tutors).
The number of student-tutors involved in the PAL intervention was not specified in 28 studies. A comparable number of studies also did not report how tutors were selected for participation. Among the studies that did specify the number of student-tutors (67/95, 70.5%), 25 studies (25/67, 37.3%) involved five tutors or fewer, while 15 studies (15/67, 22.4%) reported more than 15 tutors. The largest number of peer-tutors in a single study was 78, 102 whereas the smallest was one tutor,62,94 With respect to tutor recruitment, 30 studies (30/95, 31.6%) selected or invited tutors to participate, whereas 35 studies (35/95, 36.8%) relied on volunteer participation. Two PAL programs were delivered as part of elective modules; one within a Medical Education elective and the other within a musculoskeletal system PAL module.32,51 Table 5 summarizes the distribution of tutor types, the number of student-tutors involved, and the methods by which tutors were selected across the included studies. Overall, the included studies reveal considerable variation in learner levels, tutor seniority, and tutor recruitment methods, underscoring the heterogeneity of PAL implementation across institutions.
Population Characteristics (Student-Tutors).

PAL-Approach Characteristics
Variation in the design and delivery of PAL interventions is described below, including tutor training, program structure, comparison groups, group sizes, and assessment methods. In 38 studies, the analysed PAL intervention represented a subset of a larger, ongoing PAL program (38/95, 40%), whereas more than half of the studies (54/95, 56.8%) evaluated the full program. This information was unclear in three studies (3/95, 3.2%). Regarding tutor preparation, 31 studies (31/95, 32.6%) trained student-tutors exclusively in the clinical skills to be taught, while 13 studies (13/95, 13.7%) provided only pedagogical training. The majority of studies trained tutors in both domains (34/95, 35.8%). Only one study reported that no training was provided (1/95, 1.1%), 80 and 16 studies (16/95, 16.8%) did not specify the training approach.
Among the studies that used a controlled trial design (51/95, 53.7%), 36 trials (36/51, 70.6%) compared PAL to an expert-led teaching arm. The remaining controlled studies compared PAL to no additional intervention (8/51, 15.7%) or to alternative educational methods such as team-based learning (TBL) or virtual reality instruction.86,89 Only five studies (5/95, 5.3%) compared different PAL-approach characteristics, including intervention duration,97,115 delivery modality (online vs in-person PAL),116,119 and learner level (pre-clinical vs clinical students). 98
Only a small subset of the included studies incorporated online, hybrid, or tele-enabled formats within their PAL interventions. Four studies explicitly reported technology-mediated delivery methods: one used tele-ultrasound as the primary instructional modality, 124 one implemented an online performance-scoring system within a near-peer basic life support program, 114 one described a physical examination course combining in-person and remote components, 112 and the fourth compared online and in-person near-peer surgical teaching during the COVID-19 pandemic. 119 These technology-supported approaches were exceptions within the broader dataset, in which the majority of PAL interventions were conducted entirely face to face.
Outcome evaluation methods varied across studies: 31 studies used surveys alone (31/95, 32.6%), 19 used student assessments alone (19/95, 20.0%), and 39 used a combination of both (39/95, 41.1%). Six studies (6/95, 6.3%) did not use either method. Of these six, five collected qualitative data through focus groups,52,91 semi-structured interviews,76,110 or both. 29 One study described the program without collecting empirical data. 71
The number of sessions used to teach these skills also varied. Twenty-seven studies included only one session (27/95, 28.4%), while 19 studies reported “multiple” sessions without specifying the exact number (19/95, 20%). Among the 74 single-skill-group studies (see below), 26 (26/74, 35.1%) used a single session and 33 (33/74, 44.6%) used between two and nine sessions. None of the studies addressing three or four skill groups delivered them within a single session. The largest number of sessions reported in a single study was 21 one-hour sessions over four months, covering a single skill group. 111 The number of sessions was not specified in four studies (4/95, 4.2%).
Among the studies that reported student group size (69/95, 72.6%), most interventions (54/69, 78.3%) involved groups of no more than ten students. In contrast, two studies, both describing the same PAL program, reported group sizes as large as 50 students.102,110 Table 6 summarizes key PAL-approach characteristics, including tutor training methods, comparator groups used in controlled studies, and the distribution of skill-group numbers and session structures across the included programs. These findings highlight substantial diversity in the design, duration, comparator groups, and assessment strategies of PAL interventions, reflecting the absence of a standardized approach in current practice.
PAL-Approach Characteristics.

* The total here is 96. One study compared PAL to both expert-led teaching and team-based learning (TBL) 86
Skills Taught
The types of skills taught across the included studies varied considerably but were collated into nine categories, hereafter referred to as “skill groups”. An overview of these skill groups, along with their relative frequencies, is presented in Table 7. The most prevalent skill group was physical examination, represented in 37 of 92 programs that specified the skill taught (37/92, 40.2%). The remaining eight groups, in descending order of frequency, were surgical skills (19/92, 20.7%), ultrasound skills (17/92, 18.5%), procedural skills (16/92, 17.4%), history-taking skills (14/92, 15.2%), cardiopulmonary resuscitation skills (12/92, 13.0%), interpretation skills (6/92, 6.5%), communication skills (5/92, 5.4%), and spinal manipulative therapy (1/92, 1.1%).
Skill Groups, Number of Studies and Examples of Included Skills.

Most studies incorporated only a single skill group, with 74 of 95 studies (74/95, 77.9%) focusing on one domain. Eleven studies addressed two skill groups (11/95, 11.6%), five addressed three groups (5/95, 5.3%), and four studies addressed four groups (4/95, 4.2%). One study referred broadly to “clinical skills” without specifying the exact skill taught. 56 The distribution of skill groups indicates that PAL is most frequently applied to physical examination and procedural domains, while more specialized or interpretive skills are represented less consistently.
Missing Information
Across the included studies, several key variables were incompletely reported. The number of student-tutors involved in the PAL intervention was not specified in 28 studies (28/95, 29.5%), while tutor recruitment or selection procedures were also unreported in 28 studies (28/95, 29.5%). Tutor training methods were not described in 16 studies (16/95, 16.8%). Sample size was not reported in eight studies (8/95, 8.4%), and the number of skill groups taught was unspecified in one study (1/95, 1.1%). The academic level of tutors or learners could not be determined in a substantial proportion of studies because authors either did not specify these details or reported broad ranges. With respect to intervention characteristics, the number of teaching sessions was not reported in four studies (4/95, 4.2%), and group size was not specified in 26 studies (26/95, 27.4%). These patterns of missing information underscore the variability in reporting PAL-program characteristics and highlight the need for more standardized and comprehensive reporting frameworks.
Discussion
Literature Characteristics
The limited number of qualitative studies suggests that many researchers in this area may be more comfortable collecting and analysing quantitative, ‘objective’ data than engaging with qualitative methods. 125 It may also reflect the lack of experience of most medical education researchers in the qualitative research methodology. 126 Nonetheless, this methodology is essential in providing us with deeper understanding of how, and why, different teaching approaches, including PAL, affect learners. 127 For example, the five studies included in this review that followed a qualitative methodology have provided more insight into the challenges facing the adoption of an online PAL-program, 91 the experience of students with PAL,52,76 the processes at work within a PAL program, 29 and the impact of PAL on student-tutors. 110
Population Characteristics
The findings of this review demonstrate that the near-peer approach is the most commonly used method among researchers. It has been suggest that PAL works best when the student-tutors have an experience advantage over their colleagues. 123 The experience difference between learners and tutors is called the “educational distance” or “cognitive distance”, and there is still no consensus among researchers on the distance that yields the best educational outcomes. 128
Tutor recruitment is an essential aspect of any PAL program. 9 In most of the included studies, tutor participation was voluntary. This was true whether the tutors were selected by the faculty, answered a volunteering call, or volunteered in their own right. Ethical considerations may have played a role, but one always has to be aware of the risk of “self-selection” bias when generalizing the outcomes of these interventions. 5 Some programs were initiated, organized, and carried out by students themselves, with appropriate faculty supervision.30,55,72
PAL-Approach Characteristics
This scoping review did not report on the outcomes of PAL interventions, nor did it perform any formal appraisal. Nonetheless, the synthesized findings suggest that several methodological issues should be considered when interpreting the existing effectiveness literature. Firstly, the context and specifics of the PAL-approaches varied greatly among the included articles. Previous literature-synthesis projects done in this topic have reported a similar observation.5,18 Such heterogenicity has previously prevented researchers from systematically pooling the results of different studies to do a metanalysis. 7 Secondly, the results of the studies analyzing a fraction of a larger program may not reflect the outcomes of the whole PAL-intervention. Program evaluation theories state that the “educational context” in which an educational intervention is applied has a direct impact on the evaluation results. 129 This indicates that selecting a different part of the program may have led to different reported outcomes. A third reason is the fact that some authors used subjective self-assessment questionnaires without the utilization of an objective assessment method. Subjective methods of evaluation do not always correlate with the results of objective assessment, 5 and may lead to misleading conclusions regarding the efficacy of the intervention.
Providing student-tutors with formal pedagogical training is essential to ensure effective peer-assisted instruction. 130 In most medical education institutions, students receive no formal training in educational theory and methods, and may feel overwhelmed once they adopt the tutor role. 123 In the studies that provided aforesaid training, the selected topics varied. Examples included theoretical topics, such as adult learning principles, 108 small-group theory, 31 and theories of skill-teaching. 50 Nonetheless, most authors chose to provide a more practical training, examples included teaching strategies, 92 small-group work, 29 giving constructive feedback,59,67,102 planning an educational intervention, 46 and learner assessment. 114 Some interventions were part of a medical education elective, in which students spent several weeks learning about, and practicing, medical education.44,51,64
In theory, PAL-interventions are more suited to the teaching of clinical skills than factual skills. 9 Acquiring and improving such skills require a small-group setting, where learners get the chance to discuss, watch and practice the skills in a controlled setting. 18 Bulte et al concluded that evidence supporting PAL in small-group settings is stronger than that available for other teaching formats. 123 The findings of this review show that most researchers opted for the small group setting in their interventions. However, the exact numerical cut-off point that separates a small-group from a large-group has long been debated among medical education scholars, 131 with some even suggesting that small group-setting is rather a set of principles and skills that lead to a more useful communication between tutors and learners. 132 In the studies that followed an educational trial methodology, the majority compared PAL to expert-led teaching or to no-intervention at all. Only one study compared the effectiveness of PAL to another similar small group setting intervention (ie TBL). More well-designed trials are needed to compare PAL to other such interventions like problem-based learning (PBL) and simulation-based learning.
Only a small number of studies used online or hybrid formats for PAL. These included tele-ultrasound teaching, an online performance-scoring system, and programs that delivered some sessions remotely. Because these studies were few and varied in their design, no firm observations can be made about how online PAL compares with in-person delivery. Most PAL programs in the literature continue to be delivered face to face, which likely reflects the practical, hands-on nature of clinical skills teaching. Further work is needed to better understand when online or hybrid PAL approaches are feasible and how they might complement traditional in-person sessions.
Limitations and Recommendations
This review did not report outcomes because its scope was limited to mapping PAL approaches and their contextual characteristics rather than evaluating intervention effectiveness. Given the marked heterogeneity and inconsistent reporting of outcomes across the included studies, neither a descriptive synthesis nor a critical appraisal would have been methodologically appropriate. Accordingly, the review focuses solely on the structure and implementation features of PAL interventions. Additionally, with the large number of studies fulfilling the inclusion criteria, the choice was made not to analyse some important data points, including the aims and objectives of the included studies. Other data points may also have benefited from deeper analysis, including PAL-tutors selection and training process, the role of the PAL intervention within the larger curriculum, and the descriptions of the sessions. Furthermore, the search methodology did not include any unpublished studies or gray literature. These decisions were made in response to time and manpower constraints. Hopefully, this paper will instigate more literature synthesis projects in this important field of medical education.
The findings of this review outline how PAL is currently being used to support clinical skills teaching and highlight the wide variation in how programs are designed and implemented. These observations may help curriculum planners identify which elements of PAL are most relevant to their own settings, such as tutor level, the type of skills taught, and the structure of training or sessions. The mapping also shows areas where reporting is inconsistent, which limits comparison across institutions. Other researchers reviewing the literature on PAL have come to the same conclusion. 5 Together, these points indicate that PAL continues to be a flexible and commonly used approach in clinical skills education, but one that would benefit from more standardized reporting and purposeful integration into medical curricula.
Ross and Cameron proposed a 24-item framework to guide the planning and implementation of PAL interventions, 9 and a reporting checklist adapted from this framework is provided in Appendix 3 to support clearer and more consistent descriptions of PAL activities. In addition, a taxonomy summarizing the core components of PAL interventions has been developed based on the findings of this scoping review. Together, these tools can improve reporting transparency and facilitate more robust data synthesis and analysis in future reviews.
Conclusion
This scoping review mapped how PAL has been used to support clinical skills teaching in undergraduate medical education. The findings show considerable variation in how programs are designed, particularly in tutor level, tutor preparation, group size, and the number of sessions delivered. Most programs used small-group formats with tutor-to-learner ratios commonly ranging between 1:5 and 1:10, and tutor preparation usually consisted of brief orientations covering both the skills to be taught and basic teaching principles. Assessment methods varied across studies, with written surveys and practical skills assessments used most frequently.
Reporting practices differed widely, making comparison across studies difficult. Clearer documentation of key components would support more consistent reporting and allow educators to better understand how PAL is implemented. A unified reporting framework would be beneficial, and a draft checklist has been included in Appendix 3 to guide future descriptions of PAL activities. In addition, more qualitative research is needed to explore how tutors and learners experience PAL and to identify the contextual factors that influence its applicability in different settings. Overall, PAL remains a flexible approach for teaching clinical skills, and its integration into curricula can be strengthened through clearer reporting and deliberate planning of core program elements. By clarifying how PAL has been structured and reported, this review provides a basis for educators to design more coherent PAL programmes and for researchers to undertake future comparative and outcome-focused studies.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261422892 - Supplemental material for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review
Supplemental material, sj-docx-1-mde-10.1177_23821205261422892 for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review by Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed and Lynette Van Der Merwe in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261422892 - Supplemental material for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review
Supplemental material, sj-docx-2-mde-10.1177_23821205261422892 for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review by Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed and Lynette Van Der Merwe in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205261422892 - Supplemental material for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review
Supplemental material, sj-docx-3-mde-10.1177_23821205261422892 for The Use of Peer-Assisted Learning in Teaching Clinical Skills in Undergraduate Medical Education: A Scoping Review by Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed and Lynette Van Der Merwe in Journal of Medical Education and Curricular Development
Footnotes
Ethics Approval
Academic approval for the study proposal was granted on 16 September 2024. No human participants were directly involved.
Author Contributions
Conceptualization: Suhaib Mohamed Moamen
Methodology: Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed
Data Curation: Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed
Writing – Original Draft: Suhaib Mohamed Moamen
Writing – Review & Editing: Suhaib Mohamed Moamen, Abdulla Ismaeel Mohamed, Lynette Van Der Merwe
Supervision: Lynette Van Der Merwe
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Funding
No funding was obtained for this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.