
Abstract
Background
Chemical, biological, radiological, and nuclear (CBRN) emergencies pose major global health threats, especially in geopolitically sensitive and disaster-prone regions. Nurses, as key frontline responders, must possess sufficient knowledge, a positive attitude, and operational readiness to effectively manage such high-risk events. Simulation-based education—particularly tabletop exercises (TTEs)—is increasingly recognized as an effective method to enhance disaster preparedness in healthcare settings.
Objective
This study evaluated the effectiveness of a CBRN-focused TTE in improving nurses’ knowledge, attitude, and preparedness in a hospital environment.
Methods
A quasi-experimental one-group pretest-posttest design was employed involving 60 hospital nurses in Iran. Participants completed validated tools measuring CBRN-related knowledge (26 items), attitude (11 Likert-scale items), and preparedness (modified 45-item Emergency Preparedness Information Questionnaire). A structured tabletop scenario was conducted, followed by re-assessment 1 week later. Paired t-tests and Pearson correlation analyses were performed.
Results
post-intervention analysis revealed statistically significant improvements across all domains: knowledge (mean difference = + 8.13, 18.5% improvement, P < .001), attitude (+2.35, 10.0% improvement, P = .039), and preparedness (+30.04, 32.4% improvement, P < .001).
Conclusion
TTEs effectively improve nursing competencies related to CBRN response. Findings indicate that preparedness showed the greatest relative improvement, supporting the integration of TTEs into regular professional development programs to build readiness capacities.
Introduction
Chemical, biological, radiological, and nuclear (CBRN) incidents—whether arising from natural disasters, industrial accidents, or deliberate threats—pose a significant challenge to global health systems, particularly in geopolitically sensitive and disaster-prone regions like the Middle East and Iran. Nurses, as the largest clinical workforce and frontline responders, require comprehensive readiness across knowledge, attitudes, and operational capacities to effectively manage these incidents.
Despite intensified global efforts and institutional focus on disaster resilience, systematic reviews still highlight pronounced gaps in hospital preparedness for CBRN events. For instance, a 2024 cross-sectional survey in German tertiary hospitals reported that fewer than one-third of hospitals regularly conducted CBRN drills, properly equipped decontamination facilities, or adequately trained staff in personal protective equipment (PPE) protocols. 1 A recent systematic review corroborates these findings, demonstrating widespread deficiencies in scenario-based CBRN training and low overall operational readiness across diverse healthcare systems. 2
Simulation-based training—including tabletop exercises (TTEs)—is increasingly recognized as an effective and scalable strategy to enhance disaster preparedness. A scoping review of TTEs across health professions revealed that TTEs significantly enhance knowledge, critical thinking, inter-professional coordination, and disaster role clarity compared to traditional lectures alone. 3 An additional systematic analysis of simulation exercises, particularly tabletop formats, emphasized their cost-effectiveness, ease of implementation, and ability to identify organizational vulnerabilities in both low- and high-resource settings. 4
Among healthcare professionals, nurses derive distinct benefits from simulation-based modalities. Quasi-experimental studies in Iran and Indonesia demonstrated that combining TTEs with lecture-based workshops significantly improves nurses’ knowledge, attitudes, critical decision-making skills, and overall preparedness—often to a greater extent than lectures alone. 3 Furthermore, research in emergency medicine training has shown that simulation groups retained scenario-based competencies longer than those receiving lecture-based instruction when tested 2 weeks after the intervention (P = .036). 5 In Saudi Arabia, TTEs were shown to be nearly as effective as full-scale drills for paramedic students, with slightly higher perceived learning and greater cost-efficiency. 6
Specifically regarding to CBRN preparedness in the MENA region, a 2024 consensus-based Delphi study highlighted the urgent need to operationalize disaster readiness strategies in fragile health systems, including structured simulation training to integrate hospital staff responses. 7
Despite this growing empirical support, few studies have examined the direct impact of CBRN-specific tabletop simulations on nurses’ knowledge, attitude, and preparedness—particularly in Iranian healthcare settings. Most existing research either remains generalized under broader disaster contexts or lacks rigorous pre- and post-test designs.
This study aimed to evaluate the effectiveness of a structured TTE in improving hospital nurses’ knowledge, attitudes, and preparedness regarding CBRN incidents. The objective was to determine whether simulation-based, scenario-driven training could lead to measurable improvements in these domains, thereby supporting the integration of TTEs into routine disaster preparedness programs within healthcare settings.
Despite growing interest in simulation-based disaster education, most existing studies have focused on general disaster scenarios or combined interventions without isolating the specific effects of TTEs. Evidence on CBRN-focused TTEs remains particularly scarce, especially in low- and middle-resource settings where such incidents pose heightened risks due to fragile health systems and limited access to large-scale training facilities. Furthermore, few studies have explicitly examined the relationship between cognitive outcomes (knowledge and attitudes) and self-perceived preparedness in this context, leaving uncertainty about the mechanisms through which TTEs influence readiness for CBRN emergencies.
To address these gaps, the present study investigates the effectiveness of a structured, CBRN-specific TTE among hospital nurses in Iran. This is one of the first empirical attempts in the Middle East to systematically evaluate pre- and post-changes in knowledge, attitudes, and preparedness using validated tools. By focusing on a high-risk region and isolating the effect of TTEs, the study contributes new evidence to both global disaster education literature and practical strategies for strengthening frontline nursing capacity against CBRN threats.
Materials and Methods
Study Design and Setting
The influence of a CBRN-focused TTE on nurses’ knowledge, attitudes, and perceived readiness was evaluated using a quasi-experimental single-group pretest-posttest approach. Chosen for its strategic function as a likely receiving center for mass-casualty events, the research was conducted from March to May 2024 at a central hospital in Gerash, Iran. Though a randomized controlled study (RCT) would offer the most compelling causal proof, institutional regulations guaranteeing equal access made execution of an RCT unfeasible for all eligible personnel training. Accordingly, this design presented a moral and realistic way of assessing the TTE in a practical clinical context. We employed standardized assessment instruments, scheduled the follow-up assessment 1 week following the intervention, to minimize possible dangers to internal validity like testing effects and aging, and guaranteed uniform facilitation throughout all training programs.
Participants and Sampling
A total of 60 nurses were recruited using stratified random sampling to ensure proportional representation from clinical units involved in emergency response. Five major departments—Emergency, Intensive Care Unit, Internal Medicine, Surgery, and Pediatrics—were defined as sampling strata. Lists of eligible nurses were prepared for each unit, and participants were randomly selected using a computer-generated sequence, with the number drawn proportionate to the nursing workforce in each ward. This strategy ensured that the sample reflected the operational distribution of nurses across critical hospital units.
Eligibility criteria included: (1) a minimum of 6 months of clinical experience, (2) a bachelor's degree or higher in nursing or a related field, and (3) no prior participation in formal CBRN emergency response training. Nurses who declined participation or were unavailable during the intervention period were excluded.
An a priori sample size calculation was performed using G*Power software (version 3.1) for a paired t-test. Assuming a medium-to-large effect size (Cohen's d = 0.65), an alpha level of 0.05, and a desired statistical power of 0.80, the required sample size was estimated to be 20 participants. To enhance statistical reliability and support subgroup comparisons, we intentionally recruited a larger cohort. Ultimately, 60 nurses were enrolled across the study period. A post-hoc power analysis based on the observed large effect size for the primary preparedness outcome (Cohen's d = 0.89) demonstrated that the achieved power exceeded 0.99, substantially above the conventional threshold of 0.80. All participants completed both pre- and post-assessments, resulting in a 0% attrition rate.
Instruments and Data Collection
Three structured and psychometrically validated instruments were used to assess nurses’ knowledge, attitudes, and perceived preparedness for CBRN emergencies in a pre-test/post-test format. Data were collected in supervised, paper-based sessions—1 day before and 1 week after the TTE.
Chemical, Biological, Radiological, and Nuclear Knowledge Questionnaire
The CBRN knowledge tool, originally developed by TB Erickson et al,
8
consists of 26 multiple-choice items evaluating recognition of chemical agents, biological hazards, radiation effects, and appropriate protective responses. Each correct response is scored as 1 point, while incorrect or “I don’t know” answers receive 0 points. Total scores (0-26) were converted to percentages and categorized as follows:
− Poor knowledge: 0-33.3% − Moderate knowledge: 33.4-66.6% − Good knowledge: 66.7%-100%
Chemical, Biological, Radiological, and Nuclear Attitude Scale
Attitudes toward CBRN preparedness were assessed using an 11-item Likert-scale questionnaire measuring perceptions, willingness, and psychological readiness. Items are rated from 0 (strongly disagree) to 4 (strongly agree), with reverse scoring applied to 3 negatively worded statements. Total scores (0-44) were converted to percentages and interpreted as follows:
− Negative attitude: 0-33.3% − Neutral attitude: 33.4-66.6% − Positive attitude: 66.7%-100%
Emergency Preparedness Information Questionnaire (Modified)
The Emergency Preparedness Information Questionnaire (EPIQ), originally developed by Georgino et al,
9
was adapted to emphasize CBRN-specific competencies. The modification process involved reframing the original items within the tool's ten domains to directly reflect the context of a CBRN mass-casualty event. For instance, items related to “decontamination” specifically addressed chemical and radiological decontamination procedures, items on “infection control” were tailored to biological agent isolation precautions, and items concerning “PPE use” emphasized the selection and use of appropriate respirators and protective suits for CBRN threats. The modified version includes 45 items across 10 domains, including triage ethics, psychosocial support, epidemiology, infection control and isolation, emergency communication, decontamination, care for vulnerable populations, resource access, PPE use, and incident command. Items are scored on a 5-point Likert-scale (1 = very unfamiliar to 5 = very familiar). Total scores (45-225) were converted to percentages and categorized as follows:
− Low preparedness: < 33.3% − Moderate preparedness: 33.4-66.6% − High preparedness: > 66.7%
Validity and Reliability
Content validity was established through expert review by 7 specialists (4 emergency physicians and 3 disaster nursing faculty members). Items were rated for relevance and clarity on a 4-point scale. The scale-level content validity index (S-CVI/Ave) was 0.91, and item-level CVIs (I-CVI) ranged from 0.82 to 1.00, indicating strong content validity.
Internal consistency reliability was examined using Cronbach's alpha on pre-test data (Table 1). All instruments demonstrated high reliability:
Reliability and Validity of the Study Instruments.
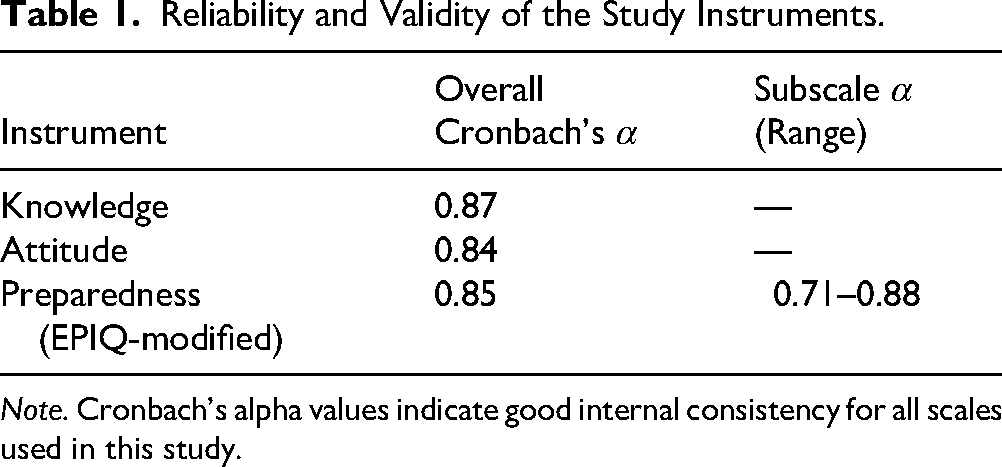
Note. Cronbach's alpha values indicate good internal consistency for all scales used in this study.
EPIQ subscale reliabilities ranged from acceptable to excellent, including:
Decontamination (α = 0.82) Triage (α = 0.79) Incident Command System (α = 0.81) Psychosocial Support (α = 0.76)
Intervention: Tabletop Exercise
A structured 120-min TTE was designed around a realistic CBRN mass-casualty scenario, consistent with national hospital emergency response protocols and WHO guidelines. The training was delivered in small groups of 10-12 participants to enhance engagement and interaction, and was facilitated by 2 certified disaster preparedness instructors using standardized materials. The exercise consisted of 3 sequential components:
A structured presentation introduced essential CBRN concepts, including threat categories, PPE, step-by-step decontamination procedures, and functional roles within the Hospital Incident Command System (HICS).
Participants engaged in a multi-stage, narrative-driven simulation depicting a combined chemical and biological incident. The scenario involved an industrial explosion resulting in the release of an unknown neurotoxic chemical, followed by the discovery of a suspected deliberate release of a Bacillus anthracis (anthrax) simulant in the same area. Participants were required to respond to evolving operational challenges, including:
Activating the HICS and establishing an incident command post Performing surge triage under resource constraints for patients with mixed symptom presentations Organizing and operating safe decontamination corridors for ambulatory and non-ambulatory patients Making time-critical decisions on isolation, prophylaxis, and internal/external communication amid diagnostic uncertainty Managing psychosocial responses and addressing a surge in “worried-well” individuals.
Participants engaged in structured brainstorming, assumed key HICS roles (eg, Triage Officer, Decontamination Team Leader), and collaboratively mapped critical response tasks.
A facilitator-moderated discussion guided participants through reflection on decision-making processes, team dynamics, and operational performance. Key learning points and evidence-based best practices for CBRN response were clarified and reinforced.
Data Collection Procedure
Data were collected at 2 time points using supervised, paper-based questionnaires. A baseline assessment was conducted 1 day prior to the intervention, followed by an identical post-intervention assessment 1 week later to evaluate retention of knowledge, attitudinal shifts, and changes in perceived preparedness. All data collection sessions took place during work hours in a quiet, dedicated hospital room to minimize interruptions.
Data Analysis
Data were analyzed using IBM SPSS Statistics version 26. Descriptive statistics (means, standard deviations, frequencies, and percentages) summarized participant demographics and outcome measures. Normality was assessed using the Kolmogorov-Smirnov test, supporting the use of parametric analyses.
Paired-sample t-tests with 95% confidence intervals were used to compare pre- and post-intervention scores for knowledge, attitude, and preparedness. Cohen's d was calculated to interpret effect sizes (small = 0.2, medium = 0.5, large ≥ 0.8).
To account for potential confounding factors, an ANCOVA was conducted with post-test preparedness as the dependent variable, pre-test preparedness as a covariate, and age, gender, and work experience as fixed factors. Pearson correlations explored bivariate relationships among post-test knowledge, attitude, and preparedness scores, and partial correlations controlling for age and work experience assessed the robustness of these associations. Statistical significance was set at P < .05.
Ethical Considerations
This study was approved by the Ethics Committee of Gerash University of Medical Sciences (Approval Code: IR.GERUMS.REC.1402.). Written informed consent was obtained from all participants following a full explanation of study objectives, procedures, potential benefits, and risks. Confidentiality and anonymity were ensured, and participants were informed of their right to withdraw at any time without penalty or employment consequences. All procedures adhered to the ethical principles of the Declaration of Helsinki.
Results
Participant Characteristics
All 60 nurses completed the study without attrition. The mean age was 29.6 ± 4.7 years, with the majority being female (66.7%), single (58.3%), and holding a bachelor's degree in nursing (70%). Most participants (75%) reported less than 10 years of clinical experience, reflecting a relatively young workforce (Table 2, Figure 1).
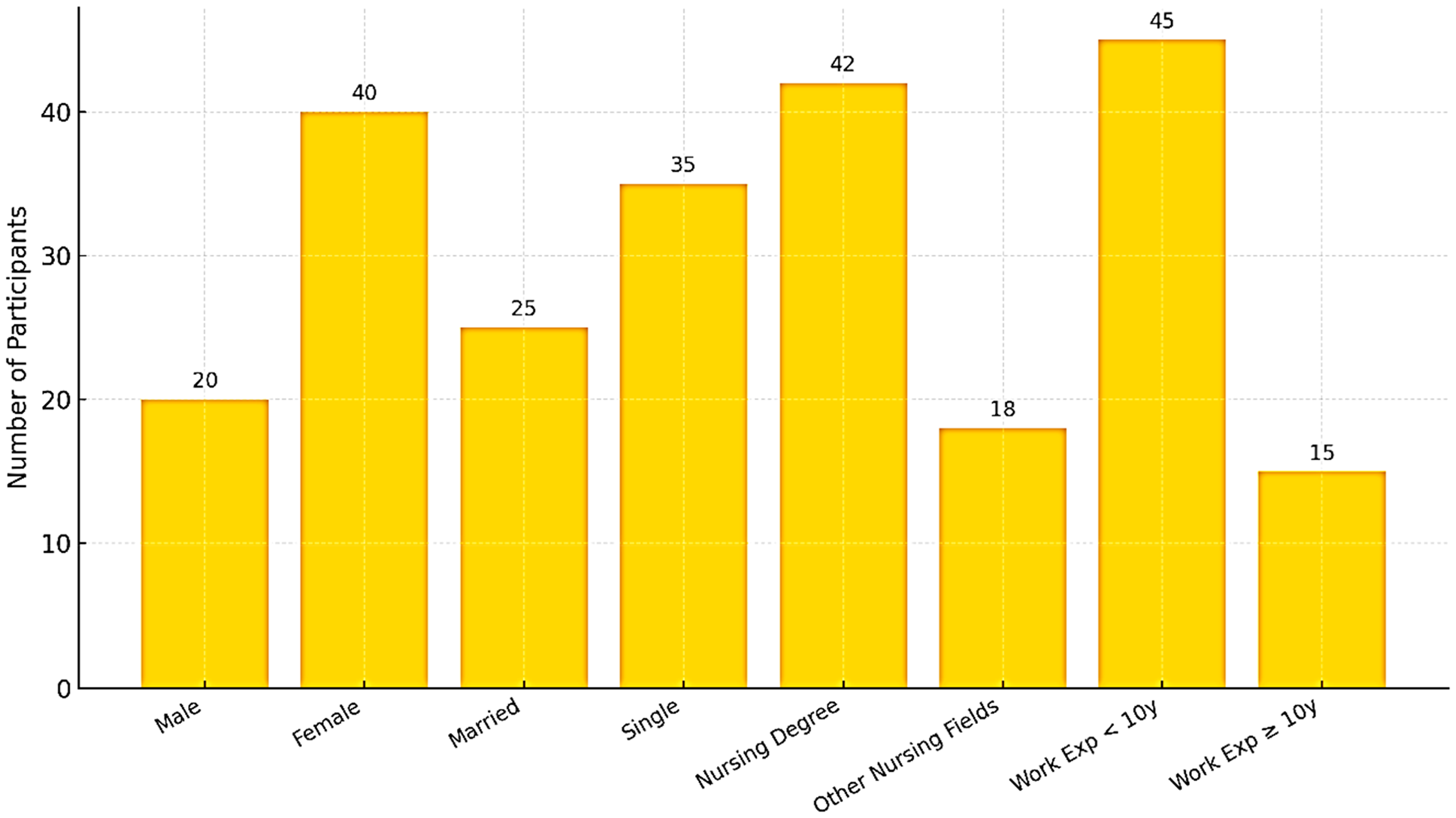
Demographic characteristics of participating nurses (N = 60), including age (mean and standard deviation displayed), gender, marital status, educational level, and years of professional experience.
Demographic Characteristics of Participants (N = 60).
Effect of the Tabletop Exercise on Knowledge, Attitude, and Preparedness
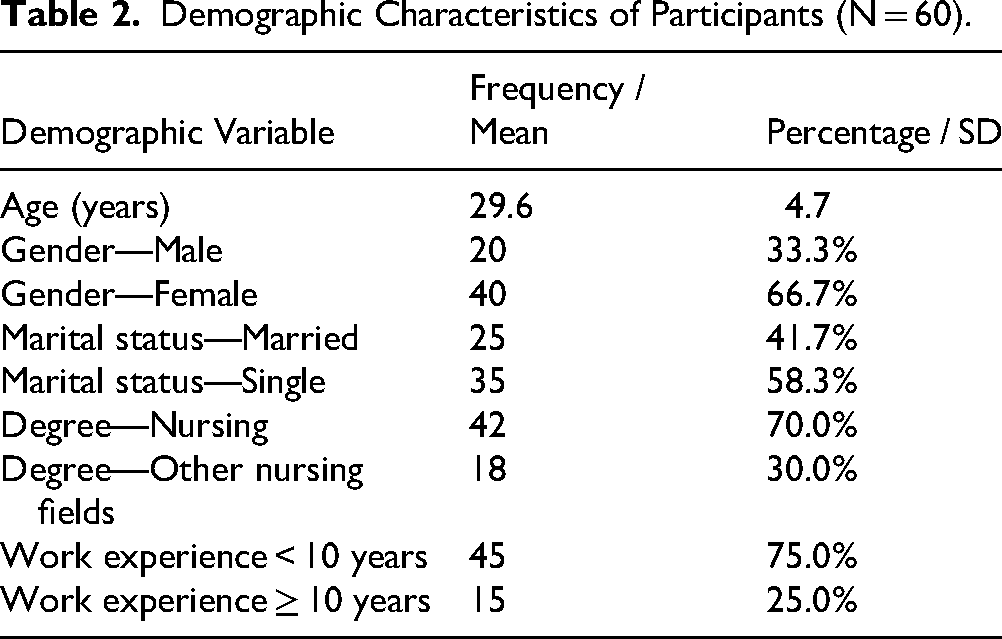
Statistically significant improvements were observed across all outcome domains following the TTE intervention (Table 3, Figure 2).
Knowledge: Scores increased from 43.95 ± 5.56 to 52.08 ± 14.21, with a mean difference +8.13 (95% CI: 4.1-12.2), t (59) = 4.12, P < .001. Cohen's d = 0.65, indicating a medium effect size. Attitude: Scores improved from 23.47 ± 6.07 to 25.82 ± 6.24, with a mean difference +2.35 (95% CI: 0.12-4.58), t (59) = 2.09, P = .039. Cohen's d = 0.27, a small effect. Preparedness: Scores rose from 92.78 ± 27.91 to 122.82 ± 26.11, with a mean difference +30.04 (95% CI: 19.8-40.3), t (59) = 6.08, P < .001. Cohen's d = 0.89, a large effect size.
Comparison of mean scores in knowledge, attitude, and preparedness related to CBRN events before and 1 week after the tabletop exercise (N = 60). Error bars represent ±1 standard deviation. Statistically significant improvements were observed in all domains following the intervention, with the greatest change seen in preparedness (P < .001). CBRN, chemical, biological, radiological, and nuclear.
Pre- and post-Intervention Scores of Knowledges, Attitude, and Preparedness.

Paired-sample t-test; significance level P < .05.
Preparedness showed the greatest improvement, while knowledge and attitude changes, though smaller in magnitude, were statistically significant. Figure 3 illustrates the overall improvement trends, highlighting the steepest rise in preparedness.

Line chart illustrating the magnitude of change in knowledge, attitude, and preparedness from pre-test to post-test (N = 60). The figure visually highlights preparedness as the most responsive domain to the training intervention, aligning with the paired t-test results.
Correlations Between Knowledge, Attitude, and Preparedness
Subgroup analyses revealed several noteworthy patterns:
These findings suggest that younger and less experienced nurses may benefit more strongly from TTE-based interventions (Table 4).
Pearson Correlation Matrix for Pre- and Post-Intervention Variables (N = 60).

Note. Values represent Pearson correlation coefficients (*r*).
Factors Influencing Post-Intervention Preparedness
To more rigorously assess the influence of demographic factors on intervention outcomes, a multiple linear regression was performed with post-test preparedness scores as the dependent variable. Pre-test preparedness, age, and work experience (in years) were entered as independent variables. The overall model was significant, F (3, 56) = 5.82, P = .002, and accounted for 26.8% of the variance in post-test preparedness (R² = 0.268). As shown in Table 4, pre-test preparedness emerged as the only significant predictor (β = 0.45, P = .001), whereas age (β = -0.18, P = .19) and work experience (β = 0.11, P = .42) were not significant when controlling for baseline preparedness (Table 5).
Multiple Linear Regression Analysis Predicting Post-Intervention Preparedness (N = 60).

Note. Multiple linear regression predicting post-intervention preparedness (N = 60). The overall model was significant, F(3, 56) = 5.82, P = .002, Adjusted R² = .23. CI, confidence interval; SE, standard error.
Multivariate Analysis
To adjust for potential confounders, ANCOVA was performed with age, gender, and work experience as covariates. The intervention effect on preparedness remained significant (F (1,56) = 18.74, P < .001), confirming that improvements were independent of demographic characteristics.
Correlations Between Knowledge, Attitude, and Preparedness
Correlation analysis is presented in Table 4. A strong positive association was observed between post-test knowledge and attitude scores (r = 0.658, P < .001). However, preparedness did not correlate significantly with either knowledge (r = 0.18, P = 0.22) or attitude (r = 0.12, P = .31). Partial correlations controlling for age and experience produced similar results, reinforcing the interpretation that preparedness depends on factors beyond cognitive and attitudinal gains.
Figure 4 displays the scatterplot of post-test knowledge versus attitude scores, visually confirming the strong linear association.
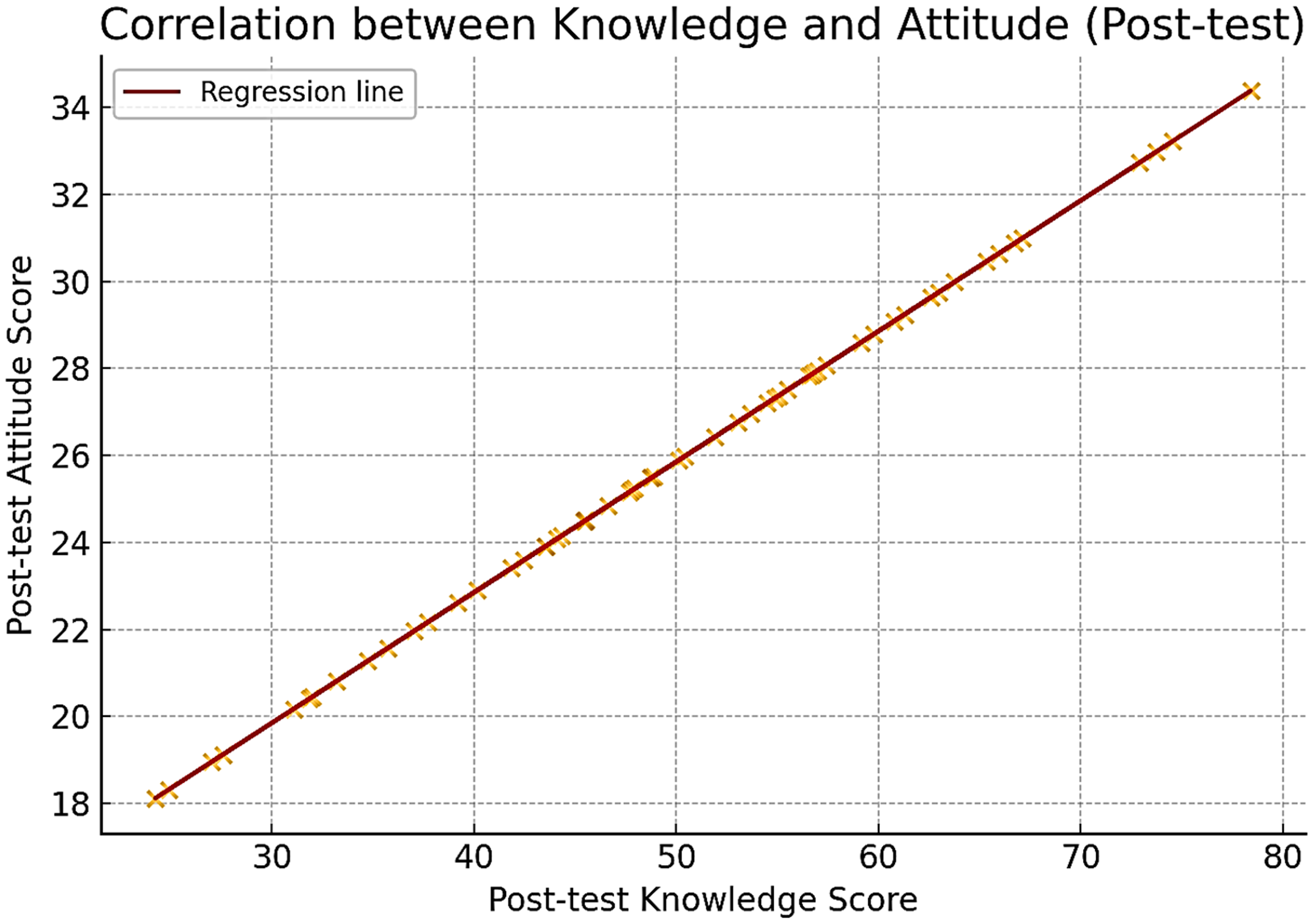
Scatterplot with regression line showing the positive correlation between post-test knowledge and post-test attitude scores among nurses (N = 60). Pearson's correlation coefficient indicates a strong linear relationship (r = 0.658, P < .001), suggesting that increased knowledge is associated with more positive attitudes toward CBRN readiness. CBRN, chemical, biological, radiological, and nuclear.
Discussion
This quasi-experimental study evaluated the impact of a structured CBRN TTE on hospital nurses’ knowledge, attitudes, and perceived preparedness. While the findings indicate promising improvements across these domains, interpretation must be contextualized within the study's single-group, pre-test/post-test design, which precludes definitive causal inferences. Factors such as testing effects or concurrent external influences cannot be entirely ruled out as contributors to the observed changes. Nevertheless, the results provide valuable preliminary evidence on the potential of TTEs in nursing education for CBRN preparedness.
Interestingly, there was no significant correlation between post-test preparedness and gains in knowledge or attitudes, despite a strong correlation between knowledge and attitude themselves. This dissociation suggests that “preparedness” in a CBRN context is a multifaceted construct, influenced more by task-specific self-efficacy, practical confidence, and familiarity with operational protocols—elements cultivated through repeated hands-on practice. This aligns with the theory of planned behavior, which posits that attitudes and intentions do not always translate into perceived behavioral control.
The multiple regression analysis further supports this notion, showing that pre-test preparedness was the only significant predictor of post-test preparedness. Nurses with higher baseline self-confidence were better able to integrate complex scenario learning, whereas age and work experience were not significant predictors. This finding indicates that TTE benefits are accessible across diverse demographics, contingent on initial readiness rather than seniority.
Limitations
The primary limitation is the quasi-experimental, single-group design, which introduces threats to internal validity such as testing bias and maturation. The absence of a control group prevents definitive causal conclusions. Additionally, reliance on self-reported measures for preparedness is a limitation, as self-assessment may be influenced by social desirability bias and may not reflect actual behavioral competence. The single-center setting and short follow-up period limit generalizability and the evaluation of long-term retention. While the study was well-powered for primary outcomes, subgroup analyses should be interpreted cautiously due to smaller sample sizes.
Conclusion and Future Directions
Despite these limitations, the study provides preliminary evidence that TTEs are practical, resource-efficient tools for enhancing CBRN preparedness. The differential impact—strong on preparedness, moderate on knowledge, and minimal on attitudes—underscores the need for a blended training approach. Future research should include randomized controlled trials comparing TTEs with active control groups, incorporate objective performance-based assessments (eg, observed drills, skills checklists), and evaluate long-term retention. Integrating TTEs with hands-on simulations and inter-professional exercises is likely essential for developing comprehensive, high-fidelity competency against CBRN threats.
Footnotes
Authors' note
Bita Soleimani, Health Care and Treatment Department of the Oil Industry of Bushehr, Bushehr, Iran; Erfan Yarmohammadinezhad, National Emergency Organization, Ministry of Health and Medical Education, Tehran, Iran.
Acknowledgements
The authors wish to thank Gerash University of Medical Sciences for administrative support and all participating nurses for their valuable contribution to the study.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Ethics Committee of Gerash University of Medical Sciences (Approval No.: IR.GERUMS.REC.1402). Written informed consent was obtained from all participants prior to data collection. Participation was voluntary, and confidentiality of the participants’ information was strictly maintained. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for Publication
Not applicable. This manuscript does not contain any individual person's data in any form (including images, videos, or identifiable personal details).
Authors’ Contributions
All authors contributed to the study conception and design. PN and EP led data collection and analysis. MD and PoN provided supervision and critical revision of the manuscript. ME and ZK assisted with statistical analysis and preparation of figures. BS and EY conducted the literature review and contributed to manuscript drafting. All authors read and approved the final manuscript and are accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality restrictions but can be obtained from the corresponding author upon reasonable request.