
Abstract
Objective
To evaluate the effects of an educational intervention, the elective course “Humanistic Values and Contemporary Medicine,” on medical students’ empathy levels and to examine the predictive value of demographic and educational variables.
Methods
A cross-sectional survey was conducted among 112 medical students using a modified Toronto Empathy Questionnaire assessing empathy in both personal and clinical contexts. Demographic and educational data were collected and analyzed for associations with empathy scores.
Results
Most students recognized the importance of empathy, but only a subset had received formal education on the topic. Enrollment in the elective course was significantly associated with higher empathy scores. Gender showed a nearly significant effect, with female students tending to score higher. Other factors, including clinical training, living arrangements, and personal experience with chronic illness, were not significant predictors of empathy.
Conclusion
Empathy is amenable to structured educational interventions and should be intentionally cultivated during medical training to support future physicians’ interpersonal competencies and emotional resilience.
Keywords
Introduction
The Importance of Empathy in Medical Education and Practice
Empathy in medical practice is a multidimensional construct that includes cognitive understanding, emotional resonance, and compassionate action.1,2 As Goleman 3 defines, it is the capacity to perceive and understand others’ emotions, intentions, and perspectives and respond appropriately. It integrates cognitive and emotional components—recognizing another's state and sharing their experience to some extent—thus enabling compassionate action. 4 Empathy is foundational to patient-centered care, enhancing trust, adherence, and clinical outcomes; 5 physicians who show empathy build stronger therapeutic alliances and deliver more effective, ethical care. 6
Unlike sympathy, which involves emotional identification, medical empathy requires recognizing patient emotions while maintaining professional boundaries. 7 Over-identification may contribute to burnout, whereas detachment can harm care.8,9 Empathy should therefore be seen not only as a personal trait but also as a professional skill that can be developed through structured training and reflective practice.10,11 Given its central role in both clinician well-being and quality patient care, fostering empathy must remain a key priority in medical education and training.
Fostering Empathy in Medical Training: Essential Skills for Future Physicians
Empathy has emerged as a core competency in contemporary medical education, integral not only to effective communication, but also to diagnostic accuracy and therapeutic relationships. 2 However, despite its significance, sustaining empathy during training is challenging. Numerous studies have documented a decline in empathy as students’ progress through medical school, attributed to stress, workload, sleep deprivation, and emotional desensitization. 9 The structure of the curriculum and the clinical environment exert significant influence on whether empathy is preserved or diminished during medical education. 12
Educational efforts to counter empathy decline must be both theoretical and experiential. Emotional intelligence theory posits that empathy is a fundamental component of emotional awareness and social competence. 3 Higher emotional intelligence is consistently associated with greater empathy and improved clinical performance. 8 Accordingly, curricular interventions that enhance emotional intelligence—such as communication training, reflective writing, and ethics seminars—can promote a more compassionate approach to care. 11
Importantly, the integration of the humanities into medical education offers a powerful means of addressing pressing challenges, such as empathy decline and burnout. 13 By presenting diverse perspectives on human experience, the humanities help students engage with the emotional and ethical complexities of care, fostering emotional intelligence, self-reflection, and resilience. 14 They also play a direct role in mitigating burnout and compassion fatigue by nurturing mindfulness, humility, and emotional depth. 15 In response to these needs, we developed and implemented an elective course, titled: “Humanistic Values and Modern Medicine” at our university's School of Medicine. This course provides an innovative framework for cultivating empathy, cultural sensitivity, and professionalism through a structured yet adaptable curriculum that integrates digital tools and experiential learning.
Study Aims
This study aims to assess empathy levels among medical students using the Toronto Empathy Questionnaire (TEQ), a validated tool that captures key dimensions of empathy: emotional contagion, perspective-taking, and compassionate responsiveness. 16 By evaluating these components, the study seeks to identify how specific aspects of empathy fluctuate over the course of medical training concern widely documented in the literature and often attributed to emotional fatigue, cognitive overload, and high-stress learning environments. 9 Such insights are critical for the development of evidence-based educational interventions aimed at preserving empathy across the continuum of medical education. 11 A central objective is to explore how empathy levels are influenced by key educational and sociodemographic variables, including gender, stage of clinical exposure, and personal experience with illness, in order to uncover nuanced predictors of empathic development. In addition, the study examines the impact of participation in our humanities-based elective course, Humanistic Values and Modern Medicine, on students’ empathy levels.
Materials & Methods
Materials
The elective course “Humanistic Values and Contemporary Medicine” (MED2135) is a semester-long, humanities-based educational intervention designed to promote empathy, cultural sensitivity, and professional identity formation among medical students. The course combines interactive lectures, guided small-group discussions, and reflective writing exercises with the analysis of literary texts, poetry, visual arts, cinema, and theatrical performances related to medicine and human suffering. Students are encouraged to engage with patients’ narratives, explore ethical dilemmas, and examine the emotional dimensions of the physician-patient relationship. Digital tools and an online portfolio support pre-class reflection and the sharing of personal perspectives. Assessment options include short reflective assignments, oral presentations, or a written essay synthesizing insights gained from the course themes. By integrating exposure to the arts with structured reflection and dialogue, the program aims to counteract empathy decline during medical training and foster more humanistic, emotionally resilient future physicians.
Upon completion of the course “Humanistic Values and Contemporary Medicine,” students were invited to complete a digital questionnaire. The study included both students who had enrolled in the course and those who had not. Inclusion criteria were enrollment in the medical program at the institution during the study period and consent to participate. Students who did not provide consent or did not complete the questionnaire were excluded. The questionnaire included a short demographic section addressing participants’ gender, semester of study, living arrangement, presence and number of siblings, and whether they had a family member or someone in their close social environment with a chronic illness. The study was conducted over the duration of a full semester (approximately 6 months) and was designed as a cross-sectional survey.
The reporting of this study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. A completed STROBE checklist has been provided as a supplementary file.
Structure of the Questionnaire
The questionnaire was divided into two main sections. The first section focused on participants’ self-reported knowledge and attitudes regarding empathy and its role in education, and included the following items: whether participants were familiar with the concept of empathy; their opinion on the importance of cultivating empathy through education; whether they had been taught the value of empathy in any course; and whether they were enrolled in the elective course “Humanistic Values and Modern Medicine.”
The second section consisted of a composite empathy scale, a set of 10 questions adapted from the TEQ. The TEQ was chosen because it provides a concise and reliable measure of affective empathy. 17 It was adapted to include items relevant to both personal and clinical contexts, allowing integration of participants’ demographic and educational variables and better alignment with the local medical curriculum. This section was further divided into two parts: “In my personal life” and “In my professional life” (for students with clinical training experience). Each item in this section was rated on a 4-point Likert scale: Never, Sometimes, Most of the time, Always. Some questions also included the option “I have not interacted with patients yet” to accommodate participants without clinical exposure. Items assessed emotional understanding, responsiveness to others’ discomfort, and perspective-taking both in social and clinical contexts. Several items were negatively phrased and later reverse-coded during scoring. The responses were used to compute a composite empathy score for each participant.
Methods
Empathy Assessment and Scoring
The responses to the questionnaire were collected digitally and exported into an Excel file for processing. Each item on the questionnaire was rated using the 4-point Likert scale with the following response options: Never, Sometimes, Most of the time, and Always, corresponding to numerical scores of 0 to 3. For negatively worded items, reverse scoring was applied to ensure that higher scores consistently reflected higher levels of empathy.
The following questions were included in the questionnaire. Negatively phrased items are marked with an asterisk (*):
When I am upset with someone, I try to put myself in their shoes for a while. When someone feels offended by a comment I made, I find it difficult to understand why they feel that way. I tend to get emotionally involved in a friend's problem. I can quickly tell when someone is feeling uncomfortable.
In a conversation, I tend to focus on my own thoughts rather than on what the listener might be thinking. I usually remain calm when I see a stranger in pain. I can tell if someone is interested or bored by what I’m saying. I try to understand what patients are thinking by observing their non-verbal communication and body language. I tend to get emotionally involved in a patient's problem. In an emergency situation, I remain calm and composed.
Based on the participants’ responses, an overall empathy score was calculated for each individual, enabling a quantitative overview of empathy levels across the sample.
Statistical Analysis
Preprocessing of Data and Selection of Demographic Variables for the Multiple Regression Model
All preprocessing steps were conducted using Python version 3.11, utilizing the pandas library for data cleaning and manipulation. Demographic variables were initially selected based on their theoretical relevance to empathy, as supported by existing literature. Among several candidate predictors—including number of siblings, gender, clinical rotation years versus non-rotational years, living arrangement, previous coursework on empathy, belief in the value of empathy training, and exposure to chronic illness—only those predictors that exhibited no conceptual overlap within the demographic context were retained for the multiple regression model. The final predictors were gender, coded with female as the reference category; clinical rotation years versus non-rotational years, with non-rotational years serving as the reference group; living arrangement, comparing those who do not live alone against those who live alone; having siblings versus none; personal or close experience with chronic illness versus none; and participation in the elective course “Humanistic Values and Modern Medicine,” where non-participation was the reference group.
Multiple Regression Model
Prior to fitting the multiple regression model, key assumptions were checked to ensure validity. Linearity was assessed by examining group means of the dependent variable across predictor categories. Independence of errors was tested using the Durbin-Watson statistic. Homoscedasticity was evaluated by plotting residuals against fitted values. Normality of residuals was confirmed through histograms and Q-Q plots. Multicollinearity was checked using variance inflation factors, and outliers or influential points were identified with Cook's Distance. A statistical significance threshold of P = .05 was used to determine meaningful predictor effects.
Results
Demographics
Of the total 112 participants, 67.9% were female. In terms of semester distribution, 8.0% were in their first semester, 27.7% in the third, 46.4% in the fifth, 1.8% in the seventh, 2.7% in the ninth, and 13.4% in the 11th semester. Regarding living arrangements, 63.4% lived with their families, 28.6% lived alone, 5.4% with a partner, and 2.7% with friends. As for family structure, 89.3% reported having siblings, while 10.7% did not. Among those with siblings, 62.5% had one sibling, 22.3% had two, 8.9% had three, and 6.2% had more than three. Finally, 62.5% of participants stated that they currently have or have had a person with a chronic illness in their family or close social environment.
Educational Background and Perceptions of Empathy
The vast majority of participants (97.3%) reported that they understood the meaning of empathy, while 2.7% were unsure and none stated that they did not know it. Most respondents (90.2%) considered the cultivation of empathy through the educational process to be important; 8.0% regarded it as less important, and only 0.9% considered it unimportant or were unsure. When asked whether they had been taught the value of empathy in any course, 44.6% responded yes, whereas 55.4% answered no. Additionally, 40.2% of the participants were enrolled in the elective course Humanistic Values and Modern Medicine, while the remaining 59.8% were not. These results are summarized in Figure 1.
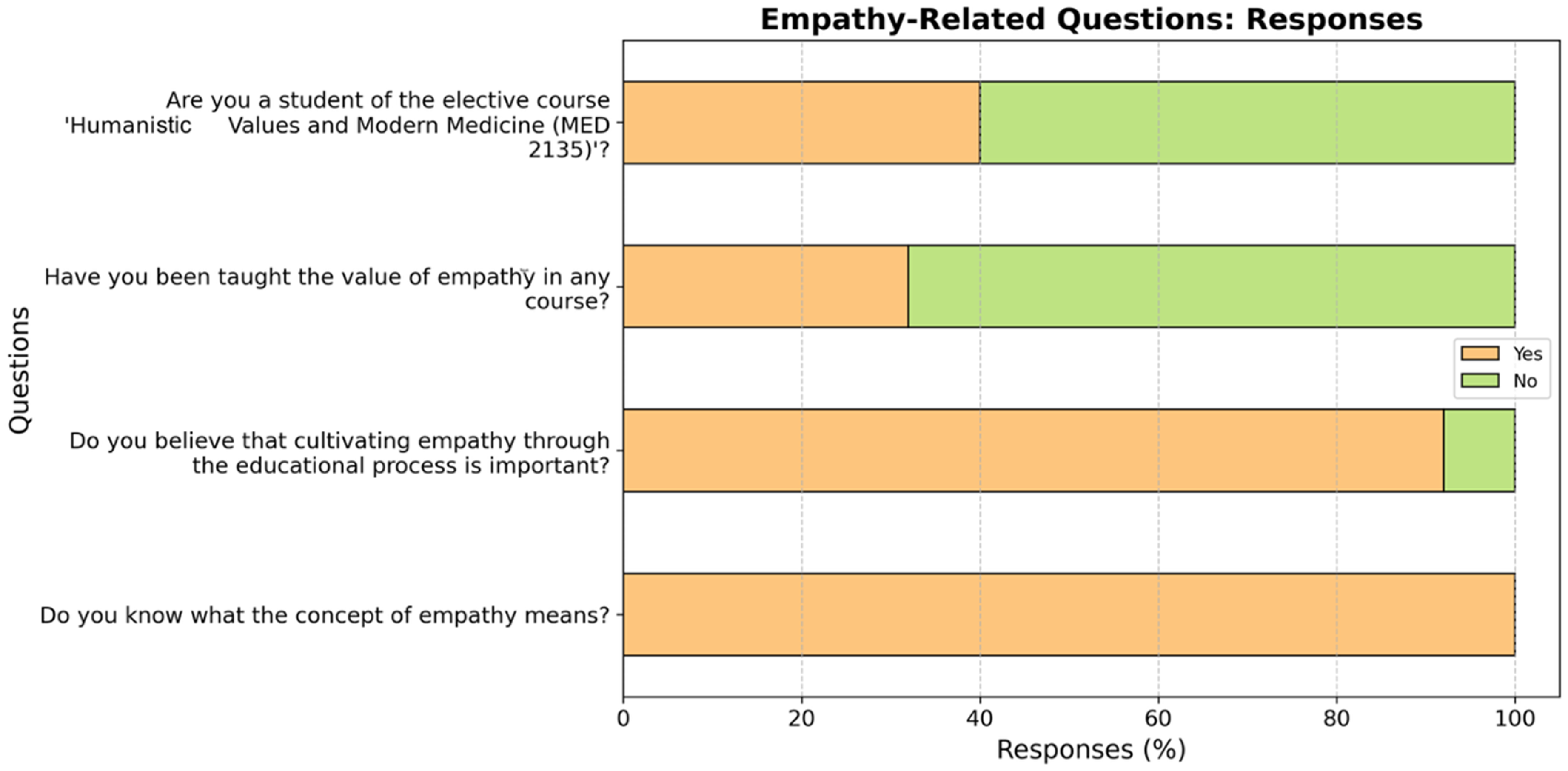
Student responses to empathy-related questions regarding educational background and perceptions of empathy.
Toronto Empathy Questionnaire
When participants are upset with someone, 22.3% always try to put themselves in the other person's shoes, 42.0% do so most of the time, 35.7% sometimes, and none reported never doing so (see Figure 2). When someone feels offended by a comment they made, 64.3% of participants reported that they sometimes find it difficult to understand why, 26.8% never have this difficulty, 8.0% do most of the time, and 0.9% always do. Regarding emotional involvement in a friend's problem, 44.6% said they do so most of the time, 33.9% sometimes, 17.9% always, and 3.6% never. When it comes to recognizing when someone feels uncomfortable, 38.4% said they always can, 51.8% most of the time, 8.0% sometimes, and only 1.8% never. In conversations, 66.1% of participants admitted they tend to focus more on their own thoughts than on what the listener might be thinking, while 23.2% never do so and 10.7% do most of the time. When witnessing a stranger in pain, 28.6% never remain calm, 40.2% sometimes do, 23.2% do most of the time, and 8.0% always stay calm. In terms of understanding whether someone is interested or bored by what they’re saying, 62.5% of respondents said they can usually tell, 25.9% always can, 10.7% sometimes, and only 0.9% never. Observing non-verbal cues in patients, 44.7% always do so, 43.4% do most of the time, 9.2% sometimes, and 2.6% never. Emotional involvement with a patient's problem was reported as frequent by 30.3%, occasional by 44.7%, constant by 9.2%, while 15.8% said they never do. Finally, in emergency situations, 60.5% of respondents stated they remain calm and composed most of the time, 28.9% sometimes, 9.2% always, and only 1.3% never.

Student responses to selected items from the Toronto Empathy Questionnaire (TEQ).
Multiple Regression Results
A multiple linear regression analysis was conducted to predict Toronto Empathy Scores based on gender, clinical rotation years, living arrangement, having siblings, experience with chronic illness, and enrollment in the elective course “Humanistic Values and Modern Medicine “ (see Table 1). The overall model was significant, F(6, 105) = 4.31, P = .0006, with R² = 0.197.
Multiple Linear Regression Analysis Predicting Empathy Scores (TEQ) from Sociodemographic and Educational Variables.

The bold values indicate statistically significant differences (P < 0.05).
Gender (female) had a positive, but marginally non-significant association with empathy scores (B = 1.49, P = .054). Clinical rotation years (7th-11th semester), living arrangement, having siblings, and experience with chronic illness were not significantly associated with empathy (all P > .05). Enrollment in the elective course was significantly associated with empathy scores. Participants not enrolled in the course scored significantly lower in the TEQ (B = -2.91, P < .001).
Figure 1 illustrates participants’ perceptions and educational background regarding empathy. Notably, the majority of students (97.3%) reported understanding the concept of empathy, and 90.2% recognized the importance of cultivating empathy through education. However, less than half (44.6%) had received formal instruction on empathy, and only 40.2% were enrolled in the elective course “Humanistic Values and Modern Medicine.”
Figure 2 presents responses to selected items from the TEQ. The data reveal that most participants frequently engage in perspective-taking and emotional involvement in personal contexts, with 64.3% sometimes finding it difficult to understand others’ feelings when offended, and 44.6% emotionally involved in a friend's problem most of the time. In professional or clinical contexts, students generally demonstrated awareness of non-verbal cues and maintained composure in emergency situations, with 60.5% remaining calm most of the time.
Discussion
This study contributes to research on empathy in medical education by assessing self-reported empathy among medical students and factors influencing it. Results show moderate to high empathy levels, with a significant positive association between participation in the elective course “Humanistic Values and Modern Medicine” and higher empathy scores. This supports the view that empathy is a skill that can be nurtured through structured education involving reflective thinking, exposure to suffering narratives, and discussions on the physician-patient relationship. 13
These findings align with Giannari et al's 13 framework, which positions empathy as a core element of clinical practice and medical professionalism. They highlight limitations in traditional technical medical training and propose a four-part model to develop empathy: motivation, skill development, empathetic organizational culture, and personal commitment, aiming to transform individual attitudes and institutional culture.
The elective course exemplifies this model by fostering humanistic values and resilience, reflecting Giannari et al's recommendations. Gender approached statistical significance, with female students tending to score higher on empathy, consistent with earlier research. 18 Other variables such as years of study and personal illness experience showed no significant association, suggesting that quality reflection and interaction matter more than mere frequency of clinical exposure.
The findings emphasize the importance of targeted pedagogical strategies to counter empathy decline during clinical training, often due to stress and burnout. This aligns with recent meta-analyses showing that humanities-based curricula with reflective practice effectively sustain empathy. 19 Future studies should include longitudinal and multi-center designs, as well as objective empathy measures, to further validate and expand these insights.
In the context of medical education in Greece, the standard medical program typically spans 6 years, with formal clinical experience beginning around the third year, depending on the curriculum structure. While our study did not specifically collect data on whether participants were parents or active caregivers for family members, future research could explore how such personal responsibilities might influence empathy development. Regarding the elective course “Humanistic Values and Modern Medicine,” participants were surveyed shortly after course completion, although the timing relative to the survey may vary across students. It is possible that recent enrollment could temporarily enhance empathy scores, whereas students who completed the course in previous years might demonstrate different levels of retention. This raises the question of whether such elective programs should be one-time events or integrated continuously throughout medical training and even into professional practice to foster sustained development of empathic skills. Future studies could examine the longitudinal impact of repeated or ongoing exposure to humanistic and empathy-focused educational interventions on both personal and professional empathy.
Limitations
Despite its contributions, this study has several limitations. First, the cross-sectional design limits causal inferences between empathy levels and the examined variables; longitudinal studies would better evaluate how empathy evolves throughout medical school and in response to educational interventions. Second, self-reported measures are susceptible to response bias, particularly social desirability, which may inflate actual empathy levels; future work could include behavioral or patient-rated assessments for more objective evaluation. Third, the study was conducted at a single institution, which may limit generalizability across different cultural and educational settings. Fourth, while the sample size was sufficient for preliminary associations, no formal sample size calculation was performed, and the study may have lacked power to detect more subtle differences, such as the nearly significant gender effect. Fifth, the study used a modified version of the TEQ to align with the local curriculum and integrate demographic and educational variables; this adapted measure was not formally re-validated, which may affect reliability and generalizability. Finally, the study did not assess factors such as burnout, stress, or emotional intelligence, which may mediate empathy and provide additional explanatory power.
Supplemental Material
sj-doc-1-mde-10.1177_23821205251405320 - Supplemental material for Restoring Empathy in Medical Education: The Measurable Impact of a Humanities-Based Course on Empathy
Supplemental material, sj-doc-1-mde-10.1177_23821205251405320 for Restoring Empathy in Medical Education: The Measurable Impact of a Humanities-Based Course on Empathy by Maria Giannari, George G. Botis, Evgenia-Charikleia Lazari, Eirini Thymara, Nikolaos G. Kavantzas and Andreas C. Lazaris in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors thank Ioannis Kostopoulos and Georgia E. Thomopoulou for their valuable input during the revision of the manuscript. The authors would like to thank Mr. Giannis Raptis and BioAnalytica A.E. for kindly covering the article processing charges (APC) for this publication. The sponsor had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Ethics Approval and Consent to Participate
This study involved anonymous participation of adult medical students. According to the policies of the National and Kapodistrian University of Athens (NKUA) and Greek regulations, anonymous educational surveys that do not collect identifiable data are exempt from formal Ethics Committee approval. All participants were informed about the purpose of the study and provided written informed consent prior to completing the questionnaire.
Consent for Publication
Not applicable (no identifiable personal data are presented).
Authors’ Contributions
MG conceptualized and designed the study, coordinated the research process, and drafted the original manuscript. GGB conducted the statistical analysis and contributed to the interpretation of results. ECL and ET collected the data, contributed to data curation, and participated in data interpretation. NGK and ACL provided critical review of the manuscript, contributed to methodology, and supervised the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
De-identified data are available from the corresponding author upon reasonable request.
Trial Registration
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.