
Abstract
Introduction
The impact of sex and gender on health is increasingly recognized and incorporated into medical curricula. However, while there is general consensus about the content to be taught, limited attention has been paid to teaching formats. Hence, in the present study we used an action-based research approach to investigate students’ preferences in learning about sex- and gender-sensitive medicine (SGSM).
Methods
We applied a qualitative multimethod action-based approach to identify a suitable teaching format for SGSM based on students’ preferences. Our study consisted of 3 phases. In the first phase we asked (bio)medical students about their methodological preferences regarding SGSM education. In the second phase, we interviewed teaching experts to identify teaching formats matching the students’ preferences. In the third phase, we designed and executed a 1.5 h SGSM seminar based on the students’ preferences and the experts’ input and evaluated its reception with a focus group and written feedback.
Results
Although students expressed learning preferences in line with state-of-the-art teaching standards, the topic of SGSM added a layer of complexity to their execution. Students expressed distinct learning preferences for the topics of sex and gender. Especially in learning about gender, they requested immersive learning experiences, structural safety in the learning space and a balance between self-directed learning and structural input. The experts suggested experience-based or transformative learning formats. The teaching experiment based on these suggestions resulted in an ambivalent experience for (bio)medical students. It proved to be engaging and instructive, but self-direction challenged the students’ expectations about the learning process, which felt uncomfortable to some participants.
Conclusion
Our experiment demonstrated that topics touching upon the personal and professional identity of students, such as SGSM, place learners in a potential position of vulnerability. Medical students reported a preference for experiential learning formats yet lack the familiarity with them. For curriculum design, this implies that SGSM should be taught through a combination of experiential methods and structured input, embedded within a safe learning environment that supports both self-reflection and the acquisition of factual knowledge.
Introduction
Over the last decades the impact of sex and gender has been increasingly recognized in the field of medicine 1 along with a growing awareness for the role of structural inequities in the healthcare system. 2 A growing body of clinical knowledge is available, and structural interventions at the level of professional societies, 3 regulatory agencies, 4 journals,5,6 and funding bodies7–9 are providing support and legitimacy to a topic long shunned in medical teaching.
Medical teaching and post-graduate training should include state-of-the-art knowledge to prepare future doctors for the complexity of their daily practice. A growing focus on structural and intersectional aspects affecting patients’ needs and wellbeing, cannot be sex- and gender-evasive. Furthermore, medical students request training in sex- and gender-sensitive medicine (SGSM)10,11 since they perceive the topic as relevant to their future practice. SGSM focuses on policies, programs, or interventions within medicine that explicitly address the culturally defined roles, duties, rights, responsibilities, and accepted behaviors that are associated with one's sex and/or gender and the associated power relations. 12 Challenges to a systematic implementation of SGSM in medical curricula are multifactorial, but lecturers and trainers play a significant role. 13 Verdonk and colleagues have reported that lecturers might have limited expertise with the topic, consideration for its relevance or perceive it as a political rather than a content-based issue. Nevertheless, some medical faculties worldwide have successfully implemented SGSM content in mandatory teaching formats13,14 sometimes even at the full curriculum level. 15 However, the applied teaching formats are generally frontal lectures, which notoriously focus on knowledge transfer rather than application. 16 Also, students’ didactic preferences have not been explored.
Teaching SGSM differs from many other topics in the medical curriculum. Since sex and gender are not just (bio)markers, but integral components of people's identity,17,18 future physicians are confronted with a high degree of complexity. They have to learn about biological mechanisms and their impact on diagnosis and treatment, 1 while critically reflecting the role of gender in actions and communication. 19 The topic furthermore implies self-reflection, as it touches upon the learner’s own identity, opinions, and potential stereotypes. 20 Learning about SGSM can be both clinically-relevant as well as personal, potentially blurring knowledge asymmetries in a patient-physician encounter.
The same challenges and dynamics are found in other identity-related topics in medical education, such as racism and diversity in medicine.21–23 For example, Powell Sears (2012) emphasizes the importance of using an intersectional framework to strengthen cultural competence education. Wong et al (2021) argue that decolonizing the medical curriculum through cultural safety and critical consciousness can humanize medicine and address systemic inequities. Cocksedge et al (2014) demonstrate that targeted teaching of communication, disability, and diversity can improve skills and support sustained learning among medical students. Taken together, these studies illustrate that teaching formats in this field range from broad faculty-development initiatives to specific courses focusing on cross-cultural communication and diversity. These parallels underline why SGSM education likewise requires careful consideration of teaching formats that move beyond a purely biomedical focus.
The 2 main challenges in teaching about racism that also apply to SGSM, seem to be the dominant focus on the biomedical perspective while overlooking other relevant psychosocial factors, and a mismatch between knowledge and skills provided in medical education compared to real-world medical practice. 24 Furthermore, quantifying learning and measuring outcomes is more challenging given the complexity of topics like race and gender, which are rarely captured adequately by standard assessments such as multiple choice questions.24,25
The Dutch Ministry of Health supported the integration of SGSM in 2002 by requesting the integration of gender mainstreaming in all 8 medical curricula. 13 However, implementation success varied and challenges were encountered at the policy, organizational, and cultural level. Uptake of gender mainstreaming proved easier within “more interdisciplinary problem-based or case-based and biopsychosocial curricula than in more traditional lecture-based, disciplinary, and biomedical curricula.”26,27 Interdisciplinary and interactive formats do appear more suitable for the topic, but this would require innovative forms of teaching. To identify whether there was a match between structural assumptions and the practice of teaching, we designed the current exploratory project. We sought to (a) identify how students wanted to learn about SGSM, (b) how these preferences could be matched with available teaching methodologies, and (c) if the preferred teaching format expressed in (b) actually meets students’ preferences (a) in practice.
Methods
Study Design
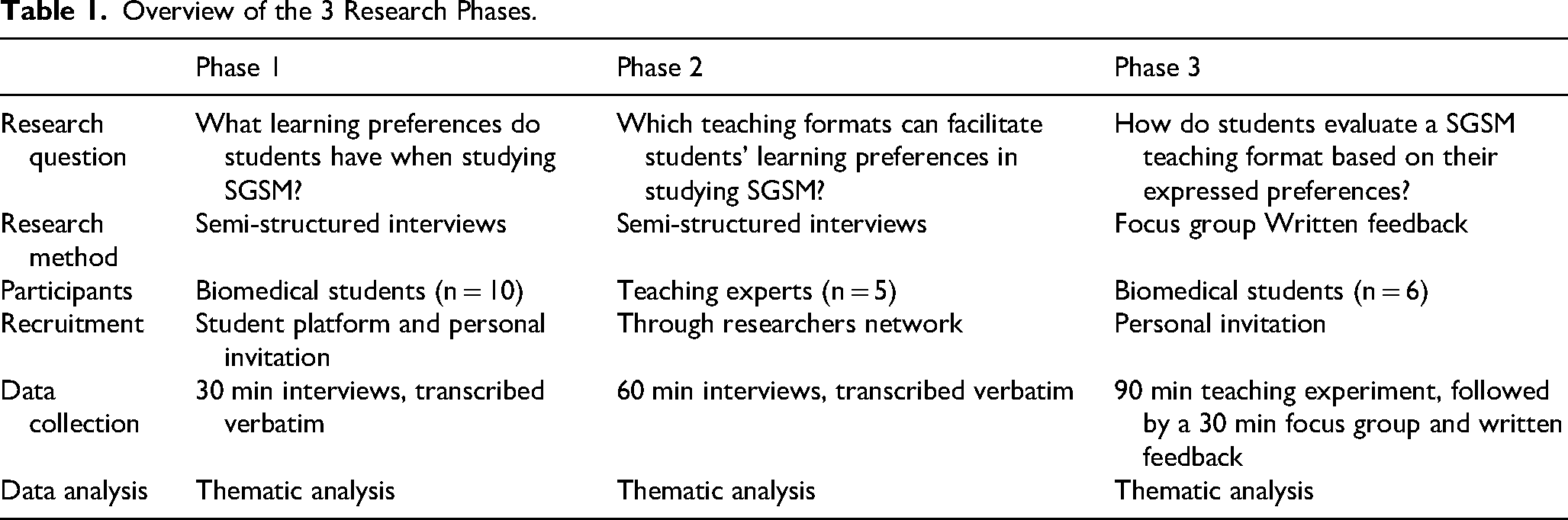
We designed a qualitative multimethod study based on a Participatory Action Research approach (PAR). PAR involves a cyclical process of research, reflection, and action to improve an existing situation based on input from relevant stakeholders. 28 Our core focus was the question: “How would students like to learn SGSM and which teaching formats can facilitate this process?” The study consisted of 3 consecutive phases (see Table 1). In Phase 1, we explored (bio)medical students’ SGSM learning preferences through semi-structured interviews. In Phase 2, we interviewed teaching experts to match teaching formats with students’ preferences. In Phase 3, we designed and implemented a 90-min SGSM teaching experiment, followed by a focus group and written feedback to capture students’ experiences with the newly developed format.
Overview of the 3 Research Phases.
Participants
Participants consisted of medical students, students of biomedical sciences and teaching experts. At our faculty, medical students and students of biomedical sciences are taught together during the bachelor phase of the curriculum; to emphasize this specificity we address the participants as “(bio)medical students” unless only one group is involved. Across all phases, purposive sampling was applied to achieve diversity in gender identity, study year, and affinity with SGSM, as well as professional background in the case of experts. 29 In Phase 1, students were recruited via faculty communication channels and personal invitations from the researchers. In Phase 2, experts were identified through the researchers’ networks and selected for their experience in biomedical teaching and transformative educational methods. In Phase 3, a new group of students was invited to take part in the teaching experiment; none had participated in Phase 1 to minimize bias.
Inclusion criteria for students were: enrollment in the (bio)medical program at Radboud University and willingness to discuss experiences and ideas related to SGSM. Experts were included based on their professional experience with biomedical education and transformative or experiential teaching methods. Exclusion criteria were lack of consent to participate and for students prior participation in an earlier study phase (to avoid repeated input).
Since our focus was on salience rather than exhaustivity we aligned with Weller et al who demonstrated that more than 95% of salient ideas can be captured within 10 interviews or even less when probing extensively. 30 While no formal power calculation was conducted given the qualitative and exploratory nature of the study, the sample size was guided by principles of information power and thematic sufficiency rather than numerical representativeness. Following Weller et al and related qualitative methodology, we considered the number of participants sufficient to capture the breadth of salient perspectives relevant to our research aims.
Data Collection
Data collection included semi-structured interviews (LM and AJ), an interactive teaching intervention (LM and SOP), a focus group (LM and SOP), and written feedback (LM and SOP). The study was conducted in the Netherlands, between June 2021 and March 2022. The interviews were performed using video call due to the COVID-19 restrictions and lasted around 30 min. The teaching intervention took place in a classroom and lasted 90 min. All interviews and the focus group were audio-recorded and transcribed verbatim. Written feedback was collected anonymously after the focus group using an evaluation form. Together, these multimodal data sources provided triangulation across students’ perspectives, expert input, and experiential evaluation. The questions used during the interviews, focus group and written feedback can be found in Supplement 1. Based on the essential elements of SGSM teaching identified by the students and experts, we developed a teaching experiment (see Figure 1).

Development Process of the Teaching Experiment.
The guiding elements for the teaching experiment can be found in Supplement 2. An overview of the teaching experiment program can be found in Supplement 3.
Data Analysis
All qualitative data were analyzed using thematic coding and analysis, guided by the research questions of each study phase. 31 All data were read and coded line-by-line by 2 researchers (LM, AJ) simultaneously using Atlas.ti 9 software. The codes were discussed until consensus was achieved. Codes were clustered and categories and themes defined in peer group sessions with all the researchers (LM, AJ, SOP). An affinity diagram was developed for all data by one of the researchers (LM) and adjusted based on feedback from another researcher (SOP). We did not conduct member checking with the original student participants; instead, credibility and trustworthiness were ensured through independent coding by multiple researchers, iterative peer debriefings, and consensus discussions. Data collection and analysis continued until no new salient themes emerged and the research team agreed that thematic sufficiency had been reached. The Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist was used for data reporting and can be found in Supplement 4. 29 All original quotes were in Dutch and translated to English for publication purposes.
Research Team and Reflexivity
LM is a Dutch female PhD researcher with a counselor background and has extensive training in communication skills combined with broad experience in interviewing techniques. AJ is a Dutch female fourth year medical student and participated as part of her research internship and was trained by LM. SOP is a German-Italian female physician and a professor of SGSM with extensive medical teaching experience in several countries and a chair at the Radboud University Medical Center and the University of Bielefeld. The researchers did not have any previous professional interaction with the participating students in the interviews or the teaching experiment. The teaching experiment was facilitated by LM and SOP and AJ participated as one of the students to reflect on the process from an insider perspective, being a medical student herself. Bias in data analysis due to involvement of the researchers in the data collection was minimized by critically discussing outsider (LM) and insider (SOP, AJ) perspectives.
Results
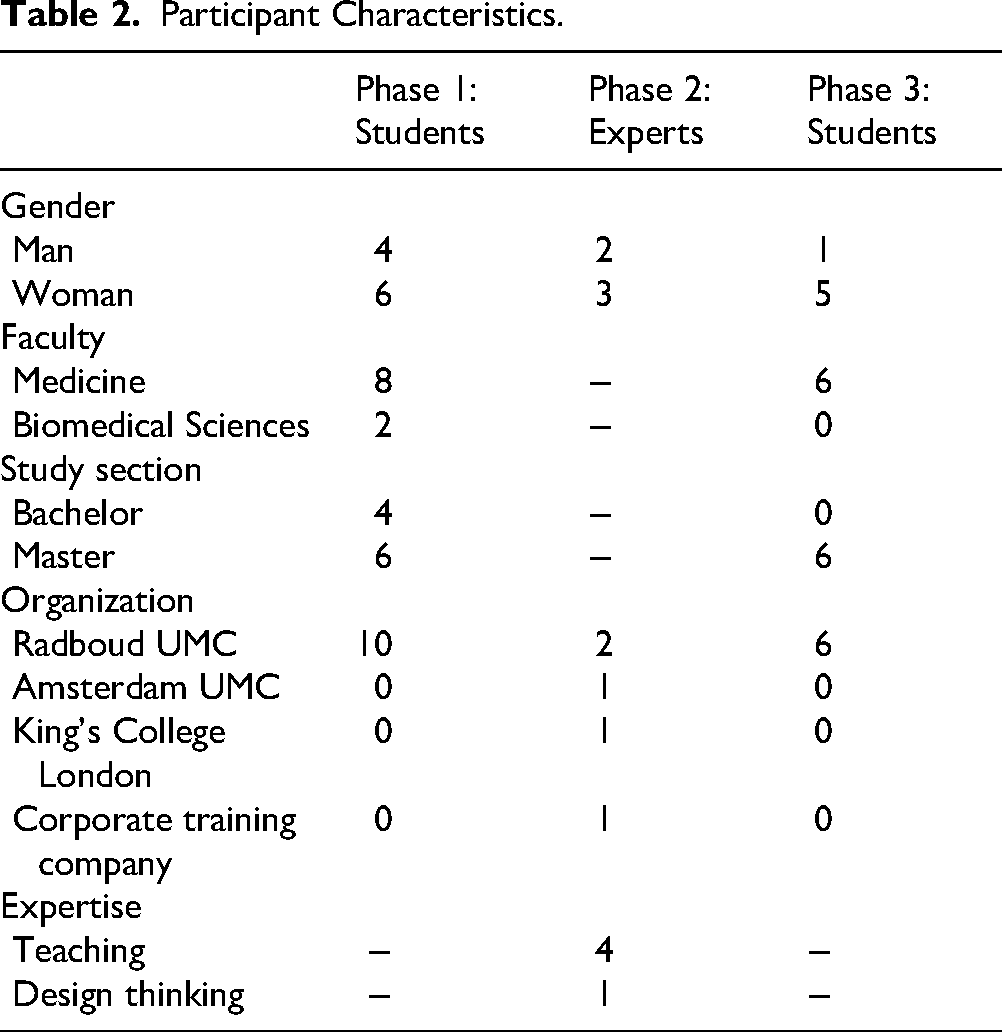
A total of 10 (bio)medical students was interviewed during phase 1 and 6 different medical students participated in the teaching experiment in phase 3. In phase 2 a total of 5 teaching experts were interviewed. Participant characteristics are summarized in Table 2. Below the findings from the 3 consecutive phases are presented. At the end of the results an overview of the findings per phase can be found in Table 3.
Participant Characteristics.
Overview of the Findings in the 3 Research Phases.

Phase 1: Students’ SGSM Learning Preferences
Interactive Learning
Students prefer interactive learning, which encompasses 3 forms for them: direct interaction (case studies, excursions, quizzes, challenges), practice-based learning (observation, patient interaction), and interaction between the different participants (students, lecturers, patients). In the context of SGSM the students emphasize the importance of creating awareness, especially about the impact of gender, through interactive formats such as, for example, discussions with other students, with patients or with doctors with SGSM expertise. Several students would rather be directly confronted with challenges in studying SGSM, instead of being provided normative explanations. This way they expect to be more engaged, enjoy the process more, even if it might be challenging, and learn more overall. Relevance of the topic and useful reflection on their process are key ingredients that make SGSM interesting in their eyes. I think if you would first learn the theory about it, then I think you would have less of a feeling of awareness. That it would have less impact, so to speak. Because then you actually start a conversation already prepared and you might also start asking more specific questions and that doesn't make it fun. You want it to be a kind of puzzle–and if you can solve it yourself with two other people and then lie in bed in the evening and think, oh, yes, yes. And then say that a teacher can clarify and solve that, that makes the puzzle complete for me. (S5, female student)
Recurrence of SGSM
Students have different thoughts on how to integrate SGSM in the curriculum: it could be a permanent course in the curriculum, an elective course, integrated in the regular modules or a combination of those three. Independently of these considerations they emphasize the importance of SGSM as a recurring theme, because it takes (a long) time to develop and integrate a SGSM perspective. One of the motivations for suggesting an elective course is related to potential negative reactions to the content of SGSM. Making it an elective course is thought to prevent students from being impacted by negative peer comments. Students also point out that integration of the topic in other modules requires lecturers to be up-to-date in their knowledge about SGSM and should assume an inclusive perspective. They expect to see a focus on both sex and gender in their training. I do think it is necessary that there is education for it, but I'm thinking now that such a working group would then last a maximum of 2 hours and that it would be about 3 times a year. Yes, and maybe this whole problem say that there is far too little education in this, is that still something that you can just weave into normal education. (S7, female student)
Real-World Learning
Students mostly want to learn ‘where the action is’, for example, in health care facilities. However, classroom-bound teaching is also welcome as long as the format is interactive and inspiring. Students feel that SGSM is about perspective change, hence, they would like to become aware of their perspectives in the “real world.” Examples of these settings could be on the street, in patients’ homes or in a museum. I do think a longer timeframe is helpful for material like this, for a lot of people it's not quite obvious and it's obviously very different from most material we get. Certainly just the difference between sex and gender which is not very much at the forefront of a lot of people's minds yet. And I think in order to really understand that kind of stuff you don't just do it in a week. So I thought if you could do this in a semester or a year in small working groups and maybe incorporate it in professionalism, make it optimal so you have more time to adapt to the material and understand it better, because with people it can just be that you have to think about it a little differently. (S8, male student)
Safe, Challenged and Fulfilled
Feeling both safe and challenged are the 2 primary requests that students hold towards SGSM education. Safety allows to openly explore SGSM which is perceived as a potentially vulnerable and personal experience. At the same time, students long to be challenged, both in terms of content as well as the process. They want to share their opinions, explore the subject autonomously, and want to take ownership for their own learning. They all state that they prefer self-guided formats, rather than frontal lectures. Fulfillment was also mentioned as a desired feeling in the context of their future practice, even if the subject might not seem useful right now. Connecting with patients is a fulfilling experience that transforms their perspective, because it adds affective learning to cognitive understanding. I think for me the most important thing is the feeling where you still have that challenge. And also a safe feeling that the four of you can just get on with the material, with the teaching materials and the teaching. That's just the most fun, really working on it. (S2, female student) But that teacher also just gets angry in class when you haven't done something. I think that is a pity. Because it's not his problem if someone hasn't done something. Then the whole atmosphere is gone. Then no one feels like answering anymore, because they are afraid of giving the wrong answer. (S3, female student)
Small Group Learning
All students prefer to learn in a relatively small groups, between 4-30 students, divided into smaller groups if necessary. Subgroups should be around 4-6 people. According to students, learning in smaller groups creates a feeling of safety and therefore invites active participation of all individuals, especially in a potentially challenging context as SGSM. Simultaneously, students expect their teacher to both create a safe learning environment and provide instructions and guidance during the discussion of difficult topics. They expect the teacher to support autonomous learning, but also to direct when necessary. Engaging patients and their social system (family, general practitioner) is high on the wish list of students, especially in the context of SGSM, as it provides them with an opportunity to practice communication about complex topics. I wrote down trusted people. For example, if this course is in the second year-end or in the second semester of the first year or in the first semester of the third year, at some point you will have a coaching group of people you have known for a while. And I don't know if that's disadvantageous or if it's advantageous, but I think it's advantageous to be able to start talking about a pretty difficult subject and also be open, more open in it. (S6, male student)
Awareness, Understanding and Skills
Students distinguish creating awareness, understanding and skills as different outcomes of SGSM teaching. Awareness entails understanding the importance of the subject on their future practice, their personal perspective and how it influences their practice and patients. Understanding focuses on knowing factual content about the impact of sex and gender on health. Skills are referred to patient-provider communication about sex and gender and integration of SGSM into practice. Students emphasize the importance of being allowed to make mistakes during the process in order to learn, both in terms of content as well as in conversations with patients. The perceived individual vulnerability during discussion of the SGSM subject enhances that prerequisite even more. I think that most students look at this with a bit of resistance. But I guess if you have a patient later on in practice who has gender dysphoria, for example, or have a transgender patient and that you know how to deal with that. You know you have to be open to that. That gives you the most satisfaction. That it doesn't come right away but that it comes later. And that then you think: great that I had that education. (S6, male student)
Assessment Variation
The students highlight the role of intermediate learning goals in guaranteeing a progressive integration of SGSM in the curriculum. Additionally, students mention that different outcomes require different assessments. Creating awareness could be investigated through active participation, patients could be asked to assess students’ performance or role play could be used to ascertain communication skills. Some students suggested potential differences in the assessment of sex and gender. According to them, sex could be tested with an exam, while gender would require more nuanced assessment as mentioned before. That you remember and continue to remember […] that the difference between sex and gender is important and that it is actually important in every field, in every area of the medical field say, and can make a difference. (S5, female student)
Phase 2: The Experts’ Input
Experiential, Multidimensional Learning
The interviewed experts recommended an experience-based learning approach with a multidimensional character to meet the students’ educational needs. Multidimensional learning according to them means addressing the cognitive, emotional, social, physical, and spiritual level. This multidimensionality can be achieved using arts-based inquiry, creative formats, and by supporting the application of knowledge and skills to concrete challenges. Interaction and discussion between students, teachers, and patients is crucial and can focus on the content as well as the process of learning. Reflection is perceived as ambivalent. The experts see it as a crucial step in learning, but also as an overused procedure. Useful reflections should have the following characteristics: they should be related to an actual experience, be the result of both a group and personal reflection process and be conducted in a format that suits the student. So music, theater, poetry, literature, visual arts. Art expressions are often ways of looking at the world differently that can do something to you, that can stir you, well. So I very much feel that that could be an entry point to trigger a rich experience. (E4, female expert)
The Safety Paradox
Safety is described by experts as the emotional foundation on which learning can occur. Safety however, has a paradoxical nature as they explain: it carries within itself an element of unsafety. Safety has to be created at the relationship level between the participants, so that a necessary amount of challenge—or “unsafety”—can be generated at the learning level. Only that allows for transformative learning. When a safe learning environment is established, connection between participants can be made. In that connection, space is given to other feelings, like openness, trust, and vulnerability. Vulnerability is considered an ambivalent emotion, that is mentioned both as a barrier and a facilitator for learning. So ultimately, if security is order and actually order is linked to the status quo, it results in insecurity. […] Nothing happens and so there is no communication, there is no dialogue, there is no openness. I think openness is a very crucial word. […] Yes, because indeed safe is maybe just nothing, keeping your mouth shut. […] So actually, the more unsafe it gets, the more likely you are to increase safety. (E2, male expert) The title of our modules that are running every year through the whole 5 years of the program are clinical humanities, wellbeing and volunteering. It is kind of trying to develop them, sort of develop each person. So, it is sort of critical pedagogy in a way. It is kind a nurturing pedagogy, but a challenging one and the end result is hopefully that they get more used to that liminality and uncertainty and complexity that is actually the reality of authentic practice. (E5, female expert)
Cultivating Curiosity and Self-Directed Learning
Curiosity is viewed as the ultimate attitude for learning and is both the starting and endpoint of an optimal learning experience. Autonomy is where students are challenged to take ownership of their learning process. Self-directed learning is associated with a certain amount of frustration which can feel negative, but is associated with a positive and rewarding learning outcome. Implementation of autonomy is challenging however, given the large number of students and different preferences. Negative emotions are mentioned on the part of the lecturers as well as the student. For the lecturer, negative emotion expressed by the students can lead to a feeling of fear of being perceived as insufficiently knowledgeable or non-expert. Being curious is the engine of learning. So if you're not curious, you stay put. Curiosity is in us. That curiosity is a drive to learn. And it weakens at some point. I like that these students want to return to a situation where they can be heartily curious again. (E3, female expert)
Role Modelling Lifelong Learning
Experts emphasize that learning has a relational nature and occurs in interaction between people and their environment. Creating a safe learning environment is crucial and consists of defining the rules, safeguarding space for diversity in thinking and doing, and role modelling desired behavior by the teacher. Role modelling lifelong learning is considered the key ingredient of a capable teacher, more than his/her expertise. Student autonomy is created by following individual curiosity and yet again lays at the very beginning of learning. However, as mentioned earlier, it is exactly this component that is difficult to facilitate given the large group of students. And so as a teacher you also have to realize that in that sense you're also on one hand really that role model, but you're not so much the role model of the expert, but you're a role model of how to be a lifelong learner. (E3, female expert)
Critical Consciousness
According to the experts, creating awareness about the importance and content of sex and gender in health care is necessary at the individual and collective level. At the individual level it is part of a students’ personal and professional identity formation. At the collective level it is about generating critical consciousness about socio-cultural aspects in the larger societal and global picture. Developing critical consciousness is seen as the result of critically reflecting on a rich diversity of perspectives by inviting students to explore those perspectives cognitively, emotionally, and socially. It has really been quite heartening to hear first-year students present their ideas and be talking about critical consciousness and reflexivity and critical stands. And then later on in the year when they have been undergoing some volunteering efforts in all sorts of things, I want them to write a critically reflective account of their volunteering. Did it help whoever it was? Why did you do it and what was the need and you know, all of this stuff and they start to get it. So, I am quite impressed because I have never heard clinical students be openly talking about reflexivity. I think most of their clinical teachers wouldn’t understand the term. I think that you know, that idea of transformative learning arguably although it has been around for a long time, I think it is axiomatic of preparing students for real-life complexity. (E5, female expert)
Learning Attitude
The experts see the development of a learning attitude as one of the most important results. This attitude is both about lifelong learning as well as lifewide learning. Staying cognitively flexible and open about yourself, others, your profession, and sources that continually inspire new thoughts, ideas, and understanding is a key attitude for lifelong learning professionals. So actually becoming self-aware also of learning to learn. We often talk about life-wide learning rather than just lifelong learning, which you do anyway. Life-wide learning means that you're also very broadly interested, and sometimes you don't know what will come out of it either. You put yourself in a situation where you're curious about what will come from that. So that you can make connections with very different subjects, but that is so important, and we sometimes forget that. (E1, male expert)
Adaptive Expertise
The focus on learning outcomes is shifting from existing knowledge and skills to generating adaptive expertise. This means that one of the most significant learning outcomes should be students’ ability to work with increasing complexity and having the skills to navigate uncertain questions in order to produce new knowledge and expertise. SGSM is seen as an excellent example to apply these skills. Learning is not a linear process that can be forced. Learning is a multidimensional process that occurs over time and is influenced by the elements of a (learning) situation. Assessment of learning outcomes is one of the most challenging parts of experience-based/transformative learning. It can have the negative effect of reducing learning outcomes to set learning objectives, thereby reducing student engagement and the richness and quality of the result. Adaptive expertise is expertise that you need to deal with situations that are unfamiliar, that are new, that you can't say you can handle or solve with the expertise, the routine expertise that you have developed up to that point. But you will actually have to find new solutions to complicated problems that have no standard solution with all that knowledge and expertise. Sometimes it can lead to new solutions or new solution strategies maybe. (E3, female expert)
Phase 3: The Teaching Experiment
Practice-Focused Interaction
Interaction was mentioned as the core quality of the teaching experience. With interaction students meant both the teaching format itself (designing a patient journey map) as well as the interaction between students themselves and the lecturers. The students appreciated applying the insights to their future practice. They liked this aspect and would like to expand on it, for example by using roleplay more often as one of them suggested. Several students mentioned they would also prefer to use more information or literature in the teaching of SGSM. This could be beforehand and/or during the teaching moment. Good to discuss what you can take away from this into the consulting room. (S1, female student)
Advanced Curriculum
One of the students mentioned it would be best to employ an experience-based SGSM format like patient journey mapping after the first 2 years of the medical curriculum. His argument was that while being interactive, the format could be more challenging and the fear of making mistakes might lead to less engagement in the first 2 years. I think it also depends on the placement in the curriculum. I think in the first or second year of the bachelor's, you don't get the audience on board as much, because you are afraid to give the wrong answer, afraid to lose competence. I notice that in myself, since the third year of bachelor I think: I'll just participate. But the first two years you don't see that as much. (S2, male student)
Challenge, Curiosity, and Discomfort
The experience-based teaching format we used, created a feeling of discomfort for some participants. They reported that both the format as well as not knowing what to expect in advance are in contrast with the typical learning experience in medical education and therefore uncomfortable. However, these feelings were not perceived negatively by the students. They reported feeling challenged by the creative teaching format. This experience of being challenged led to curiosity about the influence of SGSM and was not perceived as a barrier, given the safe teaching environment. It was very uncomfortable, because with medicine you always go into the class going oh, we're going to do this and we're going to do this and in the end you might know a little bit more than you do now, but here you didn't really know anything at all. And now you leave with a whole backpack of information because you did do things, so that's kind of instructive. It's not necessarily right or wrong, better or worse, but just different. (S3, female student)
Open Atmosphere
Students described the atmosphere as open and comfortable, even though they didn’t know each other or the lecturers. The comfortable atmosphere led to sharing thoughts and opinions openly. The topic of SGSM also invited the students to share their thoughts, since it is perceived as a topic that isn’t necessarily about giving the right answer. Students appreciated the ability of the lecturers to create an open atmosphere as well as give clear instructions. I also didn't feel very much like I could give wrong answers. It's a little less black and white than other subjects. (S4, female student)
Applicable Insights
Looking at the learning outcomes students mention increased knowledge, a broader perspective, seeing possibilities for implementation in practice (especially in patient consultations) and curiosity. The experiential learning process the students went through led to an increased understanding of the patients’ perspective.
Expectation Management and Knowledge Transfer
However, in contrast to some preferences expressed in the interviews, the participating students preferred (and are used to) knowing the content, goal, and expectations beforehand, rather than being confronted with a less predictable teaching format. Enhancing critical thinking and reflection was seen as potentially opposed to more common knowledge transfer activities. But is your goal then to get us to ask questions or just to teach us something? (S3, female student)
Discussion
In contrast to previous work in the field of SGSM teaching, the present study was designed to explore students’ learning preferences and their feasibility adapting existing teaching formats. Students’ learning preferences align with state-of-the-art teaching trends, such as a preference for interactive learning, in small groups, with recurring topics of growing complexity throughout the curriculum.31,32 The topic of SGSM, however, adds multiple layers of complexity that should be taken into account when matching learning preferences with suitable teaching formats. First, the students envision different teaching and testing needs for sex and gender. Sex should be more focused on factual knowledge transfer and tested accordingly, while gender should be explored as an immersive subject, which affects the patient and the future practitioner. Second, the immersive approach should encompass specific learning experiences; such as immersive learning, critical self-reflection, and open endedness of outcomes. Third, the vulnerability generated by the experiential approach needs to be compensated by structural safety, which acquires an essential role in SGSM teaching. Fourth, in practice, lecturers need to find a balance between self-direction of the students and provision of formal SGSM input. Overall, the findings point towards the need for an expansion of the current training formats for SGSM to transmit its operational complexity to the future physicians.
Initially, the students described many teaching preferences in line with the envisioned formats of modular medical curricula. They wish to experience immersive teaching, ideally with patients and in a care context. They prefer small group settings and mentioned how a complex topic, like SGSM, should be explored multiple times throughout the curriculum, allowing a growing depth of understanding. To date, most implementation experience with SGSM into medical curricula happened in the context of modular formats, possibly satisfying these generic preferences.13–15
The participating students describe the topic of SGSM as relevant to their future practice, as previously reported. 33 Interestingly, they distinguish between sex and gender and point out that understanding of the complexity and interconnectedness of the 2 variables requires distinct approaches. The students allocated sex-related information in the “knowledge-transfer” area and suggested that this content could be assessed by multiple choice questions upon examination. Gender-related content, on the other hand, was described as a challenging, complex theme, which needs a different teaching and assessment format. This appears to be in line with the fact that sex-specific knowledge is amenable for quantitative testing, while gender-related knowledge might be more apt to qualitative testing, such as skills lab or OSCE sessions. 34 Although not always explicitly, the students clearly described the personal dimension of gender. It appears as a subject that does not only affect their future patients, but themselves as well. It became apparent that their current understanding of gender is a limited one, often restricted to gender identity. Broadening their understanding of the concept is likely to lead to more perceived relevance to their practice. Although sex and gender are incorporated into some medical curricula,13–15 the personal dimension of gender for the future healthcare providers is rarely a topic. Extended reflection on the role of gender for the future practitioner themselves is lacking and students clearly voiced a desire to explore the subject and its implication for practice.
In addressing the subject of sex and gender using suitable teaching formats, students point out several structural requirements. They want to address the topic through discussion, self-directed learning and, ideally, with open-ended outcomes. They wish to develop their own opinion and approach, and would prefer not to be offered a predefined explanation of what gender is. The topic of gender especially is viewed as personal and touching contributing to a heightened degree of vulnerability. Rejection or ridicule in the peer group could be personally hurtful. In this context, the students stress the importance of safety of the teaching space, a topic only recently emergent in medicine. 35 The students expect the teacher to create this safe space for exploration where they can feel challenged and develop their own opinion about SGSM. The creation of a safe environment in medicine has been explored for the care context,35,36 but rarely for the teaching context. 37 Discussion of safe learning spaces are common in the social sciences and humanities,37,38 but obtain much less attention in the natural sciences. However, given that medicine is re-discovering the impact of social determinants on health, 39 lecturers might have to equip themselves with a new set of teaching tools to properly support students in learning about this field.
The results are also in line with the self-determination theory, which features autonomy, competence, and relatedness as the core components of motivation in human development. While autonomy and competence were mentioned during the interviews and are accounted for during (bio)medical education, relatedness appeared to be a crucial factor. Relatedness is understood as the process where “people tend to internalize and accept as their own the values and practices of those to whom they feel, or want to feel, connected, and from contexts in which they experience a sense of belonging.” 40 This can be facilitated by a constructive learning relation between students and teachers. However, different experiences and perceptions in the context of SGSM between students and teachers can also challenge the sense of relatedness. This emphasizes the crucial and complex role of safety in studying SGSM. Future research should also explore the preferences of teachers of SGSM, given that the topic also touches upon their personal and professional identity.
Last, our teaching experiment has demonstrated how the preference for immersive learning might conflict with the desired experience in practice. The students in our experiment enjoyed the format, but also questioned it, as it did not match their expectations. Quite possibly, it might also simply not match their experience, since the most common formats in medical curricula are often frontal teaching. For lecturers, it might be challenging to tailor the complex SGSM teaching experience to a student group with potentially different needs. Offering an open-ended safe discussion session might still be unsettling to some learners, yet in the context of transformative learning, leaving the comfort zone is essential to the experience. 41 The experiential SGSM learning experience might, thus, be different depending on the learner and future work should explore the ideal balance between self-guided learning and structured input in SGSM.
Strengths and Limitations
The present work is exploratory in nature and draws on interdisciplinary approaches. This allowed us to uncover novel questions for SGSM teaching, but the results have to be contextualized. We worked with a small group of students, who were most likely motivated to discuss the subject of SGSM and might, hence, not represent the overall opinion of medical students. A limitation of this study is the relatively small and purposively selected sample, which may restrict transferability. However, given the qualitative and exploratory design, the sample size was considered sufficient to capture the range and depth of perspectives relevant to the study aims. Furthermore, our study population was based in a specific context in the Netherlands, which might limit its generalizability. The group was mixed in terms of gender, but most participants identified as white and cisgender, which is, however, representative of the local student population. We approached the study assuming that structural factors could be relevant to teaching purposes of SGSM and specifically asked about the topic. This could potentially generate a social desirability bias in the participants, who might not spontaneously point out the role of structural factors in SGSM learning unless prompted. Although thematic sufficiency was reached, we acknowledge that additional perspectives might have emerged with a larger or more diverse sample.
Future Directions
Our findings suggest several practical strategies for advancing SGSM teaching. These include integrating short, recurrent modules across the curriculum rather than relying on single sessions, combining factual knowledge transfer (eg, sex-related biological content) with experiential formats (eg, case-based discussions or patient-journey mapping) for gender-related content, and providing explicit lecturer training in how to create psychologically safe learning environments. Future studies should examine how these approaches perform in larger cohorts and explore how assessment methods can be aligned with both factual knowledge and reflective, experiential learning.
At the same time, our pilot was deliberately designed as exploratory proof-of-concept work. To build on this, we have already conducted a multimethod qualitative follow-up study (Modderkolk et al, 2025), which demonstrated the interrelation of different safety types (social, psychological, cultural) in SGSM learning environments. These findings further highlight the centrality of safety in transformative SGSM pedagogy and provide a foundation for larger-scale validation studies. 42
Our study shows that experiential or transformative teaching formats are a potentially fruitful direction for teaching SGSM provided several elements are ensured. Overall, the descriptions of the students highlight the complexity of teaching SGSM. It is a subject which draws on traditional biological knowledge, yet challenges lecturers to generate safe spaces where medical students can reflect on their stereotypes and societal norms. This points to a need for new forms of teaching, possibly new paradigms and potentially new testing formats for SGSM teaching. The experiment we performed is a first step in developing a teaching format that focuses on the learning preferences and the multi-layered complexity of the topic for future practice within a standard timeframe typical for medical education. Seeing the format's potential and the required adjustments based on the feedback served as a stepping stone to developing a week-long summer school dedicated to sex and gender in health, further developing and testing teaching formats that can be integrated into medical education. Exploring the students’ wishes and preferences in the context of SGSM can be transferred to other complex subjects the future physicians will face in their future practice. If social determinants are perceived as intertwined and intersecting, future doctors will need sound tools for critical (self-) reflection to offer the best care and SGSM could be an ideal example to develop and test these tools.
Conclusion
Students express several learning preferences when studying SGSM, ranging from immersive learning experiences, to small group learning and distinct approaches in teaching and testing the concepts of sex and gender. Experts match the students’ preferences with experience-based or transformative teaching formats, balancing the need for immersive learning with a safe learning environment. Execution of the preferences in practice creates an ambiguous experience, for some resulting in uncomfortable, yet instructive experiences. The enhanced vulnerability experienced by students related to potentially personal topics like SGSM should be balanced by teachers’ skills to create a safe learning environment. The need for safe spaces and structural requirements in studying complex topics like SGSM could also be transferred to other social determinants of health and demand further research.
For curriculum developers, our findings suggest that SGSM is best embedded longitudinally across the curriculum, combining factual teaching on sex with experiential and reflective formats for gender, and ensuring that faculty are supported and trained to provide safe learning spaces.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251396178 - Supplemental material for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study
Supplemental material, sj-docx-1-mde-10.1177_23821205251396178 for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study by Linda Modderkolk, Anouk Jurrius and Sabine Oertelt-Prigione in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251396178 - Supplemental material for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study
Supplemental material, sj-docx-2-mde-10.1177_23821205251396178 for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study by Linda Modderkolk, Anouk Jurrius and Sabine Oertelt-Prigione in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251396178 - Supplemental material for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study
Supplemental material, sj-docx-3-mde-10.1177_23821205251396178 for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study by Linda Modderkolk, Anouk Jurrius and Sabine Oertelt-Prigione in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251396178 - Supplemental material for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study
Supplemental material, sj-docx-4-mde-10.1177_23821205251396178 for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study by Linda Modderkolk, Anouk Jurrius and Sabine Oertelt-Prigione in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205251396178 - Supplemental material for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study
Supplemental material, sj-docx-5-mde-10.1177_23821205251396178 for Students' Learning Preferences in Studying Sex- and Gender-Sensitive Medicine: An Exploratory Multimethod Study by Linda Modderkolk, Anouk Jurrius and Sabine Oertelt-Prigione in Journal of Medical Education and Curricular Development
Footnotes
Abbreviations
Acknowledgments
We would like to thank all participants for the time allocated to the study. Furthermore, we would like to thank Arne van Oosterom and dr. Jur Koksma for constructive discussion and advice on the development of the teaching intervention.
Ethics Approval and Consent to Participate
The study was granted ethical approval by the Medical Review Ethics Committee of the region Arnhem-Nijmegen (dossier number 2021-8167). All methods were carried out in accordance with relevant guidelines and regulations in the Declaration of Helsinki. All participants gave written or verbal informed consent for participation in this study. Some interviews were done online due to COVID restrictions and therefore verbal informed consent was obtained and recorded in the presence of the participant, as approved by the ethics committee. The description of the results are based on the COREQ checklist.
Author Contributions
LM and SOP designed the study. LM and AJ performed the interviews, LM and SOP performed the teaching experiment and focus group. All authors analyzed the data, LM and SOP wrote the manuscript, AJ reviewed the manuscript for important intellection content. SOP acquired funding.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Radboudumc institutional grant (JO-R4939).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.