
Abstract
Background
Case-based collaborative learning (CBCL) is an instructional method designed to promote active learning (AL). In CBCL, students learn the basics independently and apply their knowledge to case scenarios collaboratively. While theoretically the cognitive principles underlying AL in CBCL should be generalizable, implementation is shaped by local and cultural contexts. This study explored the feasibility of implementing CBCL at the University of Guadalajara, Mexico, where lectures dominate higher education and passive learning is the norm.
Methods
This study used a quasi-experimental design and an explanatory mixed-method approach. Ninety-nine fourth-year medical students, enrolled in a virtual evidence-based medicine (EBM) course, were assigned into a group taught via CBCL or a comparison group taught using lectures. Both groups covered identical EBM content: framing clinical questions, database searching, critical appraisal of randomized trials and diagnostic studies, evaluating systematic reviews, and applying evidence to patient care. Students’ knowledge (cognitive skills) and attitudes (affective dimensions) were assessed using course exams, survey data, and focus groups. Thematic analysis was used to explore the intervention's impact and feasibility.
Results
Both groups performed comparably on the knowledge assessments (CBCL 10 vs CL 9.5 out of 10, P = .72). Themes from self-determination theory were identified as underlying concepts for how specific instructional design (ID) elements influenced student perception of the CBCL intervention. Qualitative results showed how ID elements promoting autonomy (eg, clear objectives, readiness assessments), competence (eg, solving clinically relevant problems), and relatedness (eg, collaborative group work) were associated with intrinsic motivation.
Conclusion
CBCL proved feasible and valued by students accustomed to lecture-based approaches. Our findings led to a conceptual model linking specific ID elements in CBCL with motivational domains. This model can guide educators seeking to adapt CBCL or similar AL approaches to their local context and inform future research.
Keywords
Background
Active learning (AL) is grounded in the cognitive sciences and aims to model the way we teach on the way we learn.1–3 AL comprises a broad range of teaching strategies that engage students through discussions and problem-solving to generate deep understanding and sustained retention of content.4,5 As medical knowledge is rapidly expanding, AL methods provide an opportunity to help students develop critical thinking skills and learn how to teach themselves. In medical education, AL is particularly valuable for building higher-order competencies such as clinical reasoning, information appraisal, and evidence-informed decision-making—skills that demand iterative practice and collaborative application rather than passive memorization. 4 Early studies have found that AL strategies improve retention, strengthen analytical skills, and promote self-regulated learning, 6 compared to methods focused on content delivery that offer little opportunity for active engagement of the learner, such as lectures. 1 Multiple reviews support the effectiveness of AL approaches in health profession education such as flipped classroom, 7 team-based,8–11 problem-based learning,6,12 and case-based collaborative learning (CBCL).13–15 A 2020 meta-analysis of 198 schools in a wide range of educational settings found an overall positive effect of the flipped classroom, an AL strategy, on academic performance. 16
While the cognitive principles that drive AL methods should be universal to human cognition, we also know that teaching and learning are inherently “situated” activities, where outcomes are influenced by context such as local culture, available resources, and the specifics of instructional design (ID). 17 The implementation of AL methods requires many ID decisions, such as what questions to pose for discussion, what content to select for preparation, whether to include formative testing to allow for self-assessment, to name a few. Most medical educators have little to no training in ID and were often educated in traditional settings with little emphasis on AL. This is reflected in the range of challenges that have been reported with implementing AL methods. For students used to lectures, the increased cognitive effort required with AL strategies may decrease motivation and engagement, 18 and make it challenging for faculty to manage an AL environment. 19 Faculty and institutions may also struggle with the increased time needed to create meaningful AL lesson plans, faculty training, and inadequate infrastructure like suitable rooms or technology.20,21
It is, therefore, critical that we continue to assess and refine AL strategies in ways that consider local context and culture, particularly where these strategies have not been tried before. To date, there is no unified framework informed by educational theory to guide the ID and implementation of AL strategies. 22 In addition, in settings such as Mexico, where the teaching is mostly teacher-centered and lecture-based, 23 and with significant heterogeneity in the quality and strategies implemented across educational institutions, 24 there are only limited studies on the use of AL. This issue raises questions about the feasibility and acceptability of AL strategies in such environments.
In this study, we examined the impact of an AL approach among students who were enrolled in a course on evidence-based medicine (EBM) at the University of Guadalajara, Mexico. Because our setting was in a context where AL was relatively unknown to faculty and students, we aimed to assess the extent to which this AL approach was feasible and acceptable to learners in this context. We chose CBCL, an AL approach developed at Harvard Medical School and intentionally designed to teach medical students.
13
Specifically, we addressed the following research questions:
Are there differences in exam performance between students taught via CBCL compared with those taught by lecture? How do students taught via CBCL describe their learning experiences compared with those taught via lecture and how does this relate to specific ID elements? In what ways, if any, is CBCL acceptable to students accustomed to a lecture-based learning environment?
Methods
Study Design and Ethical Considerations
We conducted a quasi-experimental study using an explanatory mixed methods approach, involving both an intervention and comparison group. The first quantitative phase employed a survey to assess knowledge acquisition and students’ attitudes toward the learning experience. In the second phase, using a qualitative approach informed by phenomenology, we used focus groups (FGs) to deeply understand the students’ experience and attitudes toward learning with CBCL or virtual lectures. This explanatory approach was chosen because it allowed the initial quantitative results to inform the qualitative exploration, providing deeper insights and enhancing the overall interpretation of the CBCL approach feasibility and acceptability in this context.
The project was performed following the Declaration of Helsinki and was reviewed by the Institutional Review Boards of Harvard University (IRB20-1374) and University of Guadalajara (ID # 20-99) and deemed exempt. Participation by students was voluntary, and they were requested to sign an informed consent form.
We drew on the Standards for Reporting Qualitative Research (SRQR) 25 and the Consensus-Based Checklist for Reporting of Survey Studies(CROSS)26 checklists to guide our reporting of qualitative and survey data respectively (Appendixes 1 and 2 in the Supplemental material).
Setting, Participants, and Sampling
The study was conducted at the University of Guadalajara, Mexico, where undergraduate medical training is six years long. In 2020, we recruited fourth-year medical students enrolled in a 2-month-long required course in EBM. This student cohort was ideally positioned since they had completed foundational coursework with the clinical knowledge needed to engage meaningfully with EBM concepts and appreciate the translation of theory into practice. The primary focus of this course was to instill fundamental EBM skills among participants, including formulating answerable clinical questions, searching for and critically appraising evidence, applying the appraised evidence in clinical practice, and evaluating the process. 27 The course was conducted virtually due to the constraints of the COVID-19 pandemic. Based on their schedules, students were assigned to one of the two groups: one taught via virtual lectures and the other taught using CBCL (Figure 1). A minimum sample size of 25 students per group was estimated to be able to detect a small effect size with a power of 90% and an a priori alpha level of .05 (two-sided).

Study Design, Session Design, and Outcome Measures. (A) Students were Divided into Two Groups: Intervention and Comparison (“CBCL”=Intervention Group, Case-Based Collaborative Learning; “CL” =Comparison Group, Lectures) (n=99). The Class Was Conducted Virtually. (B) Preintervention Surveys Assessed Self-Perceived Competence in Evidence-Based Medicine (EBM), In-Class Participation Habits, and Learning Preferences. CBCL Students were Required to Study Recommended Readings and Complete a Readiness Assessment Exercise (RAE) Quiz Before the Synchronous Session, and In-Class Work on Clinical Cases and Specific Questions in Small Groups. Students in the CL Group were Asked to Study the Recommended Readings and Complete the Quizzes After the Synchronous Session and Participated in the Live Session by Answering Poll Questions. At the End of the Course all Students Completed a Final Test to Assess Their Knowledge and Skills in EBM, and were Surveyed About Their Learning Experience During the Course. Students that Attended All the Sessions were Invited to Participate Focus Group Discussions.
Intervention
For both groups, the course curriculum comprised of six sessions and included the same content, they only differed in the teaching methodology, described in detail below. The curriculum was developed by two experienced educators (HB and RIE-P) and supervised by an experienced educator and EBM expert (ND-F). Additionally, the deep knowledge of the Mexican medical-education context provided by RIE-P and ND-F, further ensured both feasibility and cultural fit. The course learning goals were the same for both groups and aligned with the main EBM principles as outlined by Ahmadi et al. 27 All course materials were created and taught in Spanish.
Course resources were hosted on the Learning Management System (LMS) Moodle 3.1. These included recommended readings and multiple-choice questions (MCQ) for each session. For both groups, the 2-h synchronous sessions were facilitated by the same instructor (RIE-P) on Zoom®, which maintained consistency across modalities. In addition, although RIE-P was an experienced educator, he received specialized CBCL training from an expert facilitator (HB) to ensure that the CBCL sessions adhered strictly to established guidelines and methodology.
In the CBCL group, students prepared by studying recommended readings and completing a short MCQ-based readiness assessment exercise before class. During the synchronous session, the CBCL-trained faculty facilitator presented a clinical scenario and introduced higher-order questions (such as application to novel situations or evaluation) to be discussed in small groups. Students were randomly placed in breakout rooms in groups of four to five, with group compositions changing each session. After the allotted time was over (∼5-10 min), all students reconvened in the large group and discussed the small group responses and opinions about the clinical scenario. To consolidate learning for each scenario, the facilitator summarized the most important points and used poll questions to ensure students’ understanding of the topic. This activity was repeated using different case vignettes, approximately three to five times until the end of the session.
In the comparison group the lecturer went over the cases, solutions, and related key concepts in a synchronous session. While the lecturer allowed questions in the chat and used some polls, the cases were not discussed between students since they were not able to interact with each other. To ensure comparability in access to course materials, students in the lecture group had access to recommended readings and readiness materials after the lecture (Figure 1).
Outcome Measures and Data Collection
Three outcome measures were used to assess students’ knowledge acquisition, attitudes toward the teaching methodologies, and lived experience. We used quantitative and qualitative measures to assess these domains. All quantitative instruments were developed following the International Association for Health Professions Education (AMEE) guide recommendations 28 including a literature review, expert review of the items, cognitive interviews, and pilot testing. Following the cognitive interviews and pilot testing, the items were reviewed, and minor adjustments were made.
To assess students’ domain-specific knowledge in EBM we analyzed quantitative data from the final exam scores, which were based on a 20-item multiple-choice questionnaire. The content of the questions was informed by current EBM literature 29 and input from three EBM experts (ND-F, LEC-L, and RIE-P). The questions were developed by two experienced educators (HB and RIE-P) and were structured using Bloom's taxonomy, incorporating both lower- and higher-order thinking skills, in alignment with published recommendations 30 (Figure 1). To evaluate student's attitudes toward the teaching methodologies and their lived experience, we used both quantitative and qualitative data. We developed a survey 28 which included both 5-point Likert-type items and open-ended responses (OERs). 31 Survey domains were selected based on our review of literature and specific aims of the study. This survey was distributed to students online using Qualtrics (Qualtrics, Provo, UT) before and after the course. Survey completion was voluntary and anonymous. The pre-course survey included questions about student self-perceived competence in EBM, in-class participation habits, and learning preferences and experiences. The post-course survey additionally included open-ended questions about self-perceived learning of knowledge and skills, and students’ experience during the course, aiming to gauge a shift in students’ attitudes toward the learning experience.
To further explore students’ experiences of learning in each of the two conditions, we conducted two FG discussions. We employed purposive sampling, targeting individuals with substantial participation (≥5 sessions) and selecting those who responded to the invitations. We held the FGs in November 2020 via Zoom®. FGs were led by DH, who did not participate in the EBM course and had no supervisory or evaluative role with the students. FGs were conducted in Spanish, in a private setting, using a semistructured interview guide, and audio-recorded with participants’ consent. The FG interview guide was developed using the survey results, to gain more understanding of students’ experience. We transcribed recordings verbatim in Spanish, de-identified the transcripts, and translated them into English. Two native Spanish speakers fluent in English (RIE-P and DH) spot-checked the transcription accuracy and translation (Appendix 4 in the Supplemental material).
Data Analysis
Quantitative data analysis compared the intervention and comparison groups using chi-squared tests of independence for categorical data, Student's t-test for parametric data, Mann–Whitney U test, and Wilcoxon rank-sum test for nonparametric data. We performed all quantitative analyses in Stata (v.16.1).
We analyzed the qualitative data from both the FG transcripts and post-course OERs 31 concurrently, using thematic analysis and the framework method, following an inductive stance. 32 Since the FGs offered richer data, these served as the main source for our analysis, while the OERs served to triangulate our findings. 33 The dataset was managed with the electronic application Dedoose (Version 8.2.36). Two authors (DH and RIE-P) read all the FG transcripts and all the survey-based OERs to get immersed in the data and to develop an initial codebook. To assess our use of the codebook, we set a kappa value of .8 as the minimum criteria for acceptable coding and used Cohen's kappa statistics to determine it. Using an inductive approach, DH and RIE-P conducted two rounds of coding for all qualitative data. All disagreements were resolved by consensus.
After coding, we examined the data using a co-occurrence matrix. We identified themes that emerged from the data via iterative discussion between all researchers (AS, HB, DH, and RIE-P). The categorization of the thematic analysis identified Self-determination theory (SDT) as the theoretical link.34,35 Then, to be consistent with the literature on SDT, we refined the codebook with new codes related to SDT (Appendix 3 in the Supplemental material), performed a third-and-final round of coding, and re-evaluated the results. This iterative process enhanced the depth of the analysis by allowing themes to be refined through multiple rounds of reflection and consensus. Ultimately, this iterative approach led to the final themes that coalesced in the conceptual model (Figure 2).

Theoretical Model for How Specific Instructional Design Elements Can Foster Motivation in Case-Based Collaborative Learning (CBCL) and Lectures. The Model Explains How Specific Instructional Design Elements Impacted Motivation. Lectures (On the Left) and CBCL (On the Right) Promoted Autonomy by Encouraging Self-Directed Learning, eg, Through Open Access to Course Resources in the Learning Management System, and by Offering Guidance on Key Learning Objectives in Class. However, Lectures were Limited in the Degree to Which They Fostered a Sense of Competence and Relatedness When Compared to CBCL. The Instructional Elements of the Lectures Implemented in Our Study Only Included In-Class Polls and Postsession Quizzes to Support Competence, While CBCL Additionally Incorporated Clinical Cases Worked in Small Groups. Peer Interactions in Small Groups Explained Why Relatedness was More Fulfilled in CBCL. Besides the Importance of Instructional Design, Psychological Safety was Important to Foster Engagement, Including in Student-Led Small Groups. The Figure Also Highlights How Traditional Lectures are Centered on the Teacher (Dotted Rectangle) and Typically Do Not Include Additional Instructional Resources or Peer Interactions, Potentially Limiting Internalization of Motivation. Note. “Competence” Here Reflects Learners' Perceived Mastery and Confidence (a Motivational Construct), Rather than Differences in Objective Test Scores
Throughout the qualitative analysis, reflexivity was maintained by the first two authors, who deliberately surfaced and documented factors that could shape their interpretations, namely, their dual roles as course facilitators and medical educators, prior conviction in the value of AL, shared cultural perspectives on Latin American teaching and learning, and institutional affiliation (Harvard Medical School). These influences were tracked in analytic memos and routinely challenged during team debriefs to enhance rigor. Furthermore, we broadened our lens by incorporating multiple perspectives, assembling a diverse team of researchers and medical scholars, and reinforced trustworthiness through ongoing analytic memos, detailed audit trails of coding decisions, and frequent collaborative discussions of emerging findings.
Results
Quantitative Results
All 154 fourth-year medical students in the EBM class were invited to participate in the study. Ninety-nine students (64.3%) volunteered and filled in the informed consent, 53 females (53.53%) and 46 males (46.46%). Participants’ mean age was 22 years (SD = 3.26), with no statistically significant differences (P = .72) between groups.
Knowledge Acquisition
All students (n = 99) completed the five short multiple-choice quizzes and one final exam. In both assessments, scores did not show a statistically significant difference between students participating in both groups. The final exam score was 10 out of 10 points in the CBCL group and 9.5 points in the lecture group (P = .067). The final exams’ internal consistency was acceptable (Cronbach's alpha = .68) given the short length of the instrument, with low difficulty (.95, SD = 0.06) and low discrimination (.14, SD = 0.16), as indicated by the item analysis.
Feasibility, Acceptability, and Attitudes Toward the Learning Experience
A total of 96 students (97.0%) completed the pre-course survey, while 92 (92.9%) completed the post-course survey. Table 1 summarizes students’ attitudes toward the learning experience by reporting baseline perceptions, the association with each condition (Δpre-post), and the comparison of impact between interventions (Δpost-CBCL − postlecture).
Results from the Preicourse and Postcourse Surveys in the CBCL and CL Groups. Questions are Presented in Descending Order Based on CBCL’s Group Effect Size.

Abbreviations: CBCL, case-based collaborative learning; CL, comparison group, lectures.
*** p-value < 0.001.
Cohen effect size: small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8).
Students in both groups agreed that the course topic was relevant to their careers and perceived a meaningful gain in competence through the course. In both groups, students felt similarly comfortable sharing their thoughts in class, but only students in the CBCL group grew more comfortable to not only share but also to challenge ideas over the time of the course (P ≤ .001). Additionally, students in the CBCL group shifted their preference toward a more learner-centered teaching approach (moderate effect size, d = 0.6). Finally, this group of students also considered preclass activities extremely important for their learning and seemed to complete the preclass assignments diligently (large effect size, d = 0.8).
Qualitative Results
The qualitative data consisted of two sources, the OERs in the pre- and postcourse surveys as well as two FGs,—one per group—with four participants each. Prior to full analysis, we assessed interrater reliability for the codebook as kappa of .81. Quotes are labeled by student number, study condition (CBCL or lecture), and data source (OER or FG).
Using thematic analysis, we identified 33 initial codes, which were then further examined using the framework method (Appendix 3 in the Supplemental material). Specifically, we used co-occurrence matrices to explore the connections and frequency of shared excerpts among codes, indicating a possible thematic association between them. The four most frequent co-occurring codes among the CBCL group were: behavioral engagement, emotional engagement, internally regulated motivation, and peer interaction for the lecture group, the most commonly noted codes were: impact of asynchronous activities, postclass quizzes, behavioral engagement, and externally regulated motivation (Table 2).
Frequency Matrix for the 10 Most Co-occurrent Codes, Comparing CBCL and Comparison Groups. Data Based on Qualitative Analysis of Focus Group Discussions. Codes were Organized According to the Number of Co-occurrences, for Codes with Equal Frequency Alphabetical Order was Also Applied.

Abbreviation: CBCL, case-based collaborative learning.
Differences in students’ lived experiences between both groups were linked to ID decisions and were shown to be associated with their emotional and behavioral engagement as well as the extent to which they described more external versus internal motivation. During the analysis we identified SDT as a theoretical framework that could link learning experiences and perceptions for both groups. SDT is a theory that explains human motivation and how it is influenced by three innate psychological needs—namely a desire for autonomy, competence, and relatedness.34,35 As described in SDT, motivation is a spectrum spanning from amotivation, to extrinsic motivation, and intrinsic motivation. Amotivation refers to a complete lack of motivation. Extrinsic motivation includes motivational states that range from being exclusively driven by external demands—such as rewards and punishments—to more internally regulated states where some values have been internalized. Intrinsic motivation is the inner force that leads to engagement in an activity for inherent satisfaction. Per SDT motivation across this spectrum is regulated by variations in the domains of autonomy, competence, and relatedness, all three of which became evident during our data analysis via inductive reasoning (Table 3).
Illustrative Quotes Related to Self Determination Theory Elements in CBCL and Comparison Groups.
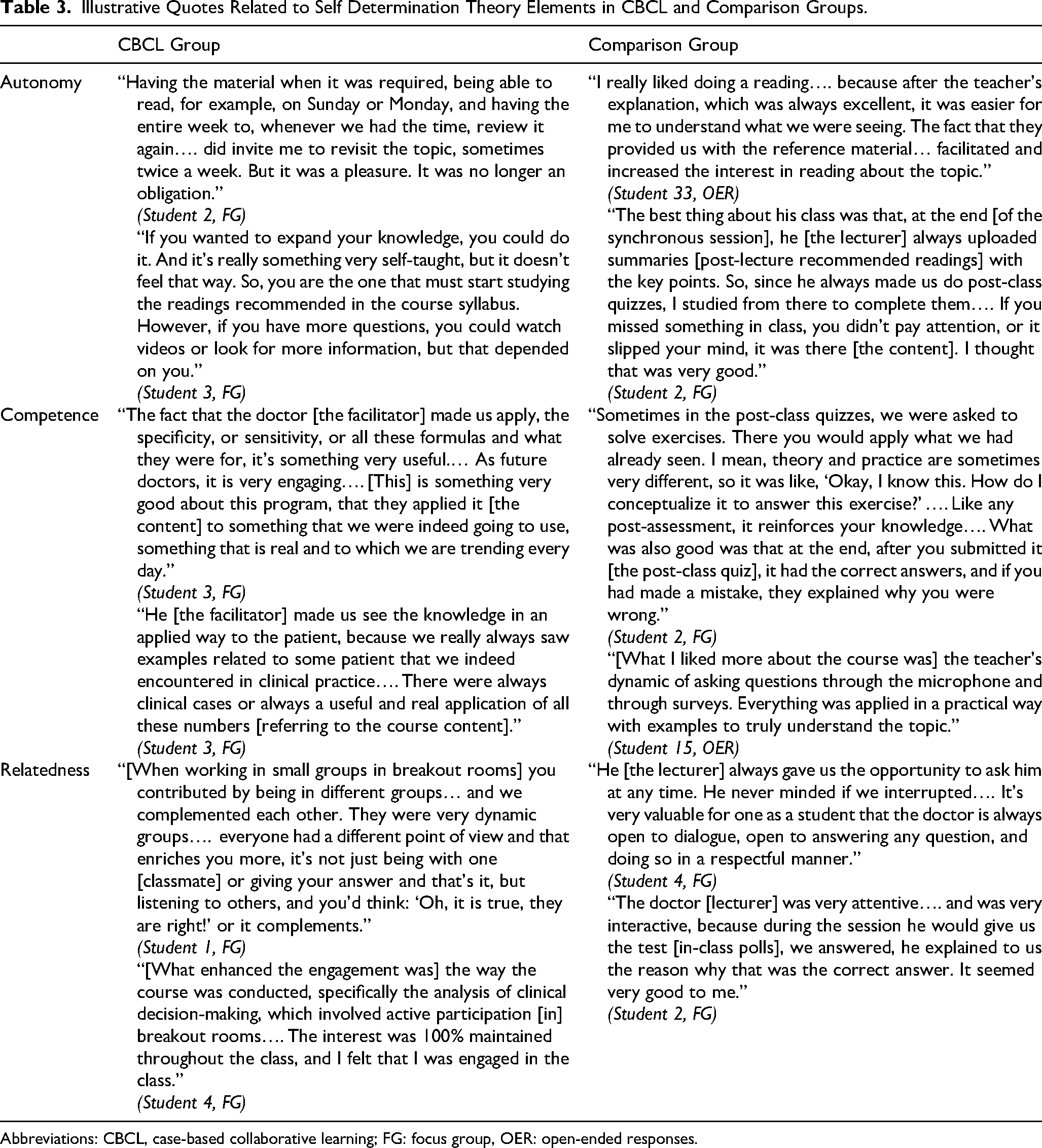
Abbreviations: CBCL, case-based collaborative learning; FG: focus group, OER: open-ended responses.
“Autonomy” is defined as the psychological need to self-direct your own learning. It was addressed in the curricula for both groups with suggested readings and quizzes—preclass for the CBCL group and postclass for the lecture group—combined with guidance from the syllabus and faculty. The asynchronous component allowed students to work at their own pace and follow their own learning goals (Table 3).
“Competence” refers to the psychological need to be effective and competent through activities or challenges related to domain expertise. This aspect was also present in both groups, but in different contexts. Students in the lecture group particularly commented on in-class polls, quizzes, and readings distributed after class as a chance to test their understanding and apply what they had learned. Students in the CBCL groups were additionally challenged with clinical cases aimed to be solved in small group discussions (breakout rooms). They commented particularly on the clinical relevance of these cases and how they could see themselves using this knowledge as future doctors (Table 3).
The third element of SDT is “relatedness”: this denotes the psychological need to connect or interact with others. To be fulfilled it an academic setting, it is necessary for the students to have an interaction with faculty or peers. In the lectures group, no interaction between peers was intentionally planned at any point of the session. Since the class was conducted virtually, students truly did not have a chance to interact with each other before, during or after class. The only direct connection they engaged in was with the lecturer, where students reported experiencing a safe space to ask questions and receive guidance or feedback (Table 3). Some students in the lecture group mentioned they would have liked to discuss with their peers. I find the point about analyzing clinical cases in a group very good. There are things that you might have missed at first, and another person could write it down…. I don't know, dedicating an hour of a class to do that, having previously read the article, and then just analyzing them [the clinical cases] as a team, maybe I feel like that would work. (Student 2, CL, FG)
In the CBCL group, students interacted extensively with the facilitator and their peers. Small group discussions were the most important component in creating a connection between students and in fostering teamwork. Breakout rooms were something I was not used to as I had never participated in a similar dynamic before. But I liked it a quite a bit because we all had the opportunity to participate, contribute knowledge and clarify doubts. I also believe it was beneficial as it reminded me of the importance of knowing how to work in a team. (Student 23, CBCL, OER)
While most students seemed to enjoy the breakout group discussions, some individuals expressed dissatisfaction with their peer interactions and subsequently decreased in-class engagement. No one took into account my participation [in small group discussions]. And it turns out that I was the one who was right… With the people I was assigned [in small group discussions], on some occasions, not all, it's like they don't lend themselves to listening to opinions that weren't from their clique. (Student 3, CBCL, FG)
Within our study, motivation played an important role in shaping students’ lived experiences and revealing differences between the CBCL and lecture groups.
Students in the CBCL group reported motivation as being more internally regulated, reflecting an inner desire to engage with all the course elements. The interaction we had during each class and in all those stages that the doctor [facilitator] guided us through, I think that's what made us want to repeat the following week, look forward to the next Friday, to have that class again…. We felt involved, interested. (Student 2, CBCL, FG)
In contrast, students in the lectures group described motivation mainly as being driven by the questions and activities created by the lecturer and the quizzes and readings available after class—thus, being more externally motivated. You say: “OK, I need to know this because they ask it [in the post-class quizzes]” So, I feel like paying more attention in class. (Student 2, CL, FG)
Based on the results, we iteratively created a conceptual model (Figure 2) to explain and represent how each group experienced the learning process. This model shows qualitative differences between groups and how they impacted the fulfillment of autonomy, competency, and relatedness; and consequently, how motivation and engagement were affected.
Discussion
This study demonstrates the feasibility and acceptability of CBCL in a cultural context where students were accustomed to lectures. Students rated the class highly regardless of whether they were assigned to the CBCL or CL group. Despite students’ having little to no experience with AL, students in the CBCL group completed preclass reading and preclass quizzes, showing the feasibility of this teaching methodology even with students used to lecture-based and teacher-centered approaches that do not require any preparation before class.
When comparing performance, we observed no differences in knowledge acquisition between groups. These findings are consistent with previous research on CBCL 13 and could also be attributed to a ceiling effect resulting from the majority of the students mastering the content. These results contribute to the existing literature, which presents mixed findings regarding the impact of AL on overall knowledge acquisition. 9 Nevertheless, AL can yield significant effects beyond knowledge acquisition and may exert a broader influence on the development of other skills or on the learning process itself. 4
Both lectures and CBCL methods instilled motivation through specific ID features. The ability to freely access course resources on the LMS and to engage with them in self-directed manner created a sense of autonomy compared to the access to knowledge via lectures these students were accustomed to. Using testing (preclass in the CBCL group and postclass in the CL group, to ensure all students had access to the same content) promoted a sense of competence. Using in-class polling in lectures and case discussion alike increased this sense of competence. The opportunity in the CBCL group to discuss cases with peers in small groups created relatedness beyond what we detected in the CL group—where students only interacted with the lecturer. This depended on psychological safety in their small groups, a phenomenon we have observed before in CBCL. 14 The facilitator also guided students on the most relevant aspects of the course and promoted engagement; therefore, influencing all motivational domains described in STD—autonomy, competence, and relatedness.
This is consistent with findings in a team-based learning (TBL) setting, a format that shares some similarities with CBCL. Jeno et al. found that TBL, compared to lectures, provided motivational benefits by enhancing autonomous motivation, competence, engagement, and learning over time. 36 More recently, Stieha et al. linked various AL practices to competence, relatedness, and autonomy, illustrating how ID decisions and practices align with SDT. 37
In our study, specific ID elements (use of quizzes, in-class polls, and clinical cases) influenced students’ competence and perceived usefulness of the course content. It is noteworthy that in traditional lectures at this university, design elements that focus on knowledge application are typically absent. The role of the lecturer is mostly to provide content and answer questions. Therefore, based on the model, we would predict students being mostly extrinsically motivated in this setting (eg, via requirements to pass an exam). These findings align with a recent scoping review that identified agency and a sense of competence as critical factors for student engagement in undergraduate medical education. 38
By comparing two instructional settings, our study suggests that the specific instructional elements operate independently—offering instructors the possibility to combine different instructional elements that fit their educational context in the most meaningful and practical ways. Therefore, our model provides a tool for educators to guide the implementation of AL strategies even in environments that traditionally rely on passive learning methods. Our findings also indicate that when considering AL methods, student motivation might be an important outcome to consider.
Limitations
This study was conducted in Mexico, where traditional teacher-centered educational approaches are dominant, and students had no prior experience with AL. The lecture format in this study included in-class polls and distribution of resources after class (readings and quizzes) to ensure all students enrolled in this class had access to the same resources. These features set the lectures apart from lectures traditionally used at the University of Guadalajara where the lecture itself is the sole source of content.
The results of the final exam also indicated that most of the students mastered the content at the end of the course, suggesting a ceiling effect. This ceiling effect likely contributed to the low discrimination index of the final exam questions and limited our ability to detect potential differences between the groups.
Delivering the sessions online due to the COVID-19 pandemic created a controlled experimental setting where students in the comparison group did not have any opportunity to interact, effectively isolating this variable. Since CBCL was originally developed for the in-person context, further research is needed to evaluate how our findings may translate to an in-person environment. Nonetheless, while existing literature suggests that online learning can diminish collaborative interactions when compared to in-person settings, a study specifically examining CBCL in a virtual environment found that students’ sense of learning was surprisingly unaffected by the reduced formal and informal interactions with teachers and peers. 39 This suggests that the true impact of the online environment on collaborative interactions is still unclear and warrants further investigation.
In addition to our findings on the learning environment, we also identified SDT elements inductively during our analysis, but this was not the anticipated focus of our study. Further research is needed to investigate the interplay between specific ID elements in CBCL and SDT.
Additionally, our findings may be influenced by self-selection bias and response bias, since participation was voluntary and survey data were self-reported. However, the high consent and completion rates, along with methodological triangulation, support the robustness and relevance of our results.
Finally, we recognize that having only two FGs may have limited the diversity and depth of insights gathered. To address this, we also analyzed OERs from 92 (92.9%) postintervention survey participants, which enriched our findings and facilitated triangulation. Because our goal was to capture a broad range of perspectives and achieve content depth, we did not aim for thematic saturation. Future research should consider additional FGs or individual interviews to further enrich the diversity of insights.
Conclusions
This study provides evidence and a framework on how SDT can inform the ID of such AL interventions. In our model, opportunities for self-directed learning instilled a sense of autonomy. Application problems—as in case discussions or in-class polls—fostered competence. Opportunities to interact with peers and faculty increased relatedness. Together these ID elements drove motivation and internalization—the process of moving from an externally motivated to an internally motivated state which could lead to increased engagement and potentially improve learning. However, since this study was limited to one course at a single institution, testing the model in other settings and disciplines will help confirm its broader applicability. Additionally, more studies are needed to assess the impact of AL interventions on student learning and motivation over time. Our findings highlight the critical role of ID in adopting AL approaches across different cultural contexts and emphasize the need to include motivation and other SDT domains to assess the effectiveness and impact of AL methods.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251385013 - Supplemental material for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study
Supplemental material, sj-docx-1-mde-10.1177_23821205251385013 for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study by Dominique Harz, Ramiro Israel Esparza-Perez, Amy Sullivan, Netzahualpilli Delgado-Figueroa, Luis Enrique Colunga-Lozano, Krisztina Fischer, Melissa Campos-Zamora and Henrike Besche in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251385013 - Supplemental material for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study
Supplemental material, sj-docx-2-mde-10.1177_23821205251385013 for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study by Dominique Harz, Ramiro Israel Esparza-Perez, Amy Sullivan, Netzahualpilli Delgado-Figueroa, Luis Enrique Colunga-Lozano, Krisztina Fischer, Melissa Campos-Zamora and Henrike Besche in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251385013 - Supplemental material for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study
Supplemental material, sj-docx-3-mde-10.1177_23821205251385013 for How Specific Instructional Design Elements Influence the Experience of Case-Based Collaborative Learning in a Mexican Medical School: A Mixed-Methods Study by Dominique Harz, Ramiro Israel Esparza-Perez, Amy Sullivan, Netzahualpilli Delgado-Figueroa, Luis Enrique Colunga-Lozano, Krisztina Fischer, Melissa Campos-Zamora and Henrike Besche in Journal of Medical Education and Curricular Development
Footnotes
ORCID iDs
Ethics Approval
The study was reviewed by the Institutional Review Boards of Harvard University (IRB20-1374) and University of Guadalajara (ID # 20-99) and deemed exempt.
Consent to Participate
Students participated voluntarily and signed a written informed consent form.
Author Contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Upon reasonable request, the datasets utilized and analyzed for this research can be obtained from the corresponding author.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.