
Abstract
Purpose
This systematic review for medical professionals aimed to characterize the pleiotropic effects of emotional intelligence (EI) training programs, with an emphasis on the transfer of leadership skills and their impact on the performance of physicians, healthcare organizations, and patient care.
Major Findings
Of 4034 articles, 40 articles were included for the final review, including 26 from the United States, with a total of 2373 participants (1431 medical students, 692 residents, and 250 physicians). All 40 articles (19 on medical students and 21 on residents/physicians) reported using quantitative and/or qualitative methods of assessing EI among the participants with 7 being randomized and 31 considered moderate to strong evidence. Only 2 studies demonstrated the beneficial effect of EI training on patient satisfaction (Kirkpatrick 4C) and 3 studies on organizational benefits (Kirkpatrick 4A); 19 studies demonstrated effects on participant's performance, such as reduction of stress and burnout (Kirkpatrick 4B). Nearly all studies scored 2 or more on the scale for best practices, with 5 studies scoring 6/7. Bar-On Emotional Quotient Inventory (EQ-i 2.0) was the most frequent tool to gauge improvements in participant EI (9 studies); a mean improvement of 4% to 8% in EQ-i 2.0 total score was reported after EI training.
Conclusions
Healthcare institutions and organizations need to incorporate EI training while developing their leadership development programs. EI can be built over time through direct practice and coaching and is important for future initiatives in medical curricula, raising hospital competitiveness, improving hospital disaster resilience outcomes, implementing effective digital healthcare, and addressing socioeconomic and racial health disparities. Several of our findings are supported by moderate to strong evidence, including 7 randomized studies. However, more research is necessary to standardize EI training approaches; EQ-i 2.0 may be preferred in future studies to ensure standardization and comparability of EI assessment between programs.
Keywords
Introduction
Physician Leadership, defined as “the ability to effectively and ethically influence others for the benefit of individual patients and populations,” has been identified as a priority in modern healthcare. 1 There has been a growing interest in developing physician leadership training in the past 20 years.2,3 Soft skills such as professionalism, empathy, interpersonal skills, critical thinking, and stress management are essential components of physician leadership and can be highly consequential for healthcare systems. 4 Despite this, professionalism has been identified as one of the most challenging-to-teach competencies, 5 and there have been well-observed declines in empathy during the clerkship years, 6 suggesting that current programming is inadequate for sustaining professionalism and empathy levels in the healthcare system.
Emotional intelligence (EI) has been touted as an all-encompassing construct to address these soft skill gaps in physician leadership education. 7 There is ample literature suggesting either strong associations between soft skills and EI or that the terms are essentially interchangeable. 8 EI refers to the ability to “monitor one's own and others’ feelings and emotions, [and] to decipher those feelings to guide one's thinking and actions.” 9 Since its inception, the body of literature has grown considerably with the developments like the Bar-On and Goleman models, which both define ability EI as an “array of non-cognitive skills, capabilities, and competencies,” and trait EI as “a constellation of emotional self-perceptions located at the lower levels of personality.”10,11 While measuring ability EI is beneficial for researchers and faculty interested in leadership skills requiring strong emotional abilities such as decision-making, problem-solving and negotiating, trait EI has been beneficial in developing equally important leadership competencies of self-efficacy and task-related stress management. 12
Despite the evidence supporting EI as a key component of leadership skills, it is underrepresented in healthcare leadership training curricula. 13 Two prior systematic reviews show positive outcomes for physician training to increase EI.14,15 However, few included studies used validated tools for measuring overall EI, and the majority reported singular EI components. Additionally, these systematic reviews are focused mainly on medical students and residents and provide insufficient data on EI training of attending physicians. Finally, these reviews focus only on ability EI and lack evidence related to trait EI in healthcare leadership. Therefore, we aimed to summarize and interpret contemporary evidence of EI training within healthcare educational curricula for medical students, residents, and physicians over the last 20 years to provide timely and relevant evidence for collaboration, innovation, and next steps in healthcare leadership training. Our primary aim was determine what changes in EI, behaviors, perceptions, and clinical practice are seen in medical students, residents, and physicians who participate in EI leadership training programs.
Methods
Search Strategy
The literature search was conducted in the PubMed and Google Scholar databases in March 2024. We considered additional databases, but based on the scope of our topic (EI training in medical education), we found that PubMed and Google Scholar comprehensively index the relevant medical education literature. Prior systematic reviews on similar topics have also relied on these databases. 7 The reporting of this review conforms to the Preferred Reporting Items for Systematic Review and Meta-Analysis 2020 guidelines 16 (see Supplementary Digital Content 1) and was not registered on PROSPERO. Ethics approval was not required. The research question was defined using the PICO framework (Population, Intervention, Comparison, Outcome): Population – Medical students, residents, and physicians; Intervention – EI or leadership training programs; Comparison – Not Applicable; Outcome – Changes in participant EI scores, behaviors, and clinical/organizational outcomes. The search strategy was developed and finalized collaboratively by the study authors and was overseen by UB with expertise in systematic reviews. The databases were systematically searched from 2004 to 2024 on articles containing EI educational interventions for undergraduate medical students, postgraduates, and practicing physicians. The following search expressions were used: “Emotional Intelligence” AND (“healthcare” OR “leader” OR student OR Medical OR resident), and (“emotional intelligence” OR “emotional competence” OR “emotional quotient”) AND (“physician” OR “resident” OR “med student”) AND (training OR program) (See Supplementary Digital Content 2). No filters were applied during screening in either database.
Inclusion and Exclusion Criteria
Studies were included if they (1) reported non-traditional medical curricula that explicitly aimed to teach or practice EI abilities/skills, characteristics, or competencies in their objectives, (2) were experimental or quasi-experimental, cohort studies, case-control studies, or randomized controlled trials, (3) included medical students, residents, or physicians, and (4) were peer-reviewed full-text articles published in English. Studies were excluded if they: (1) did not report on outcomes relatable to a modified New World Kirkpatrick model, 17 (2) taught or tested on EI measures other than Mayer and Salovey's definition of ability EI, Goleman's mixed model EI definition and Petrides and colleagues definition of trait EI (Figure 1), (3) analyzed multiple curricula or pooled other healthcare providers with physicians, and (4) were review articles, conference abstracts, or letters to the editor. Studies with quantitative data were assessed and excluded if they (1) utilized instruments without confirmed validity when measuring EI and (2) did not include both pre- and post-intervention data for validated tools.
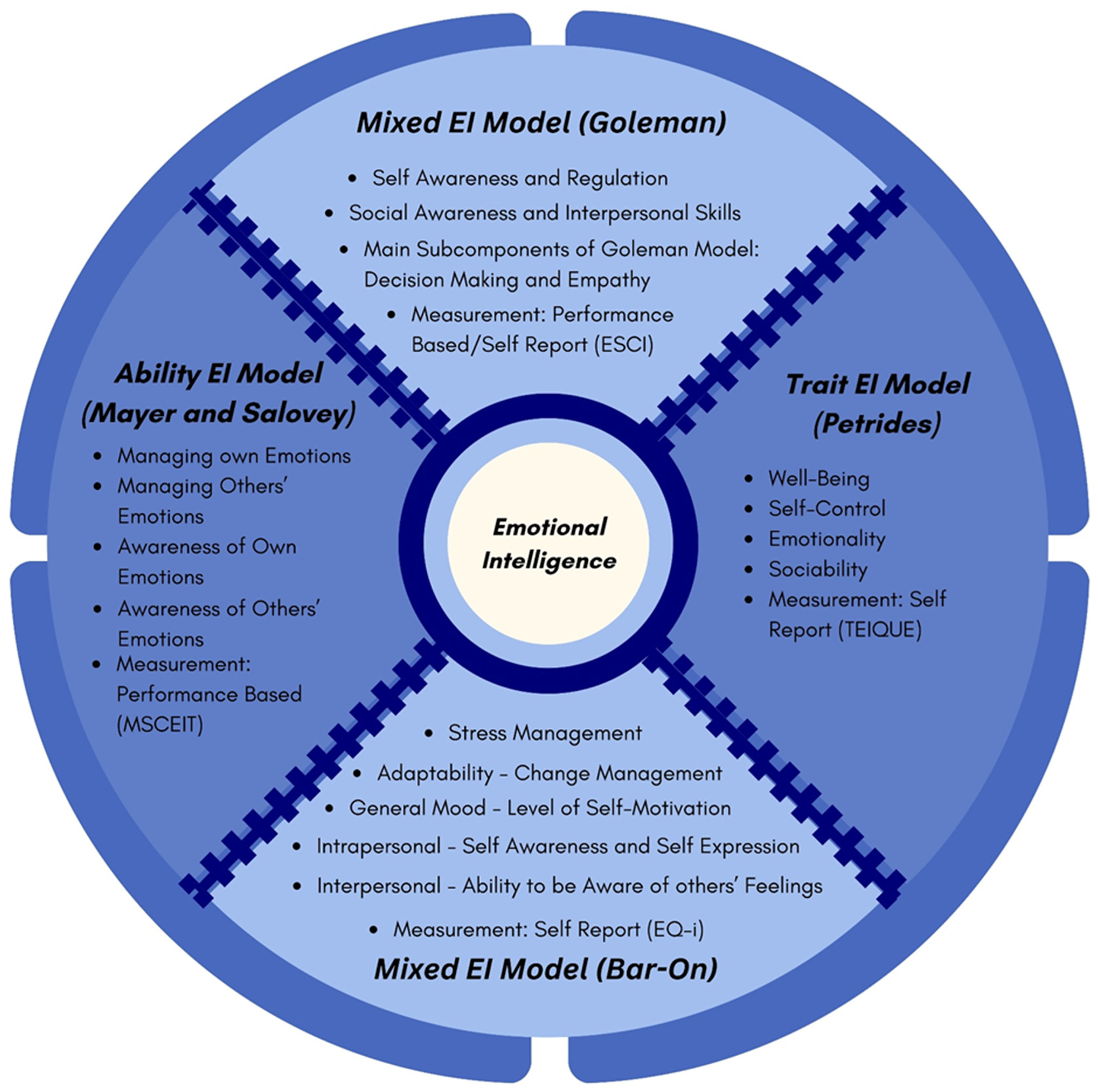
Utilized contemporary models of EI. Legend: Each program tested on a specific EI model that correlates to a set of cognitive domains and is associated with leadership competencies. The diagram presents the four different EI models and their integral characteristics: the Mixed EI Model (Goleman), the Ability EI Model, the Trait EI Model, and the Mixed EL Model (Bar-On). EI, emotional intelligence.
Title and Abstract Review
Following the initial screening with the specified keywords, the articles were reviewed based on their titles. After preliminary selection, each abstract was read, and if it met the inclusion criteria, the full text was analyzed to obtain the final list of studies (Figure 2). Three review authors performed this. All authors worked independently during this activity, and one author resolved disagreements.

PRISMA flow diagram for screening and selection. Legend: The PRISMA flow diagram details the selection process of the studies included in this review. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Full-Text Review
Data extraction was done using a standardized table. The table included the Author, Year of Publication, Kirkpatrick Level, Participants, Selection Method, Format of Intervention, Time of Intervention, Outcome Measure, Outcome Measurement Tool, and Key Findings. Several authors independently extracted the data from included studies, and one author confirmed such data.
Outcome measures were assessed using a modified New World Kirkpatrick model, which examines the effectiveness of an intervention using multiple levels of analysis (See Table – Supplementary Digital Content 3).18,19 The model includes 4 levels: Level 1 (learner's reaction to content of the intervention), Level 2a (changes in attitude and perception following the intervention), Level 2B (improvement of skills resulting from the intervention), Level 3 (behavioral development as a result of learning), Level 4A (tangible changes in organizational practice), Level 4B (advantages for participants) and 4C (changes in patient care, quality, safety, etc.). The primary outcome was to assess the change in overall EI. The secondary outcomes were EI subcomponents, including awareness and management of one's own/other's emotions, empathy, interpersonal skills, stress management, decision-making, burnout, and well-being.
Quality Assessment
The Risk of Bias 2 (RoB-2) and Risk of Bias in Non-Randomized Studies (ROBINS-I) Tools were used to assess the methodological quality of each study.20,21 Each article was classified as exhibiting low, moderate, serious, or critical risk of bias and assessed across several domains, including bias due to confounding, bias in selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, bias in selection of the reported result, and overall bias.
Scoring for Adherence to Recommended Best Practices of Formulating Emotional Intelligence Training
A previous review 22 had recommended several best practices, which were used to create a numeric scoring system consisting of 7 elements, with each element weighted equally as 1 point and the maximum score being 7. The seven elements were as follows: longitudinal exposure, multiple teaching methods, internal plus external faculty, access to mentors, interdisciplinary participants, assessment of impact, and evaluation of multiple Kirkpatrick levels.
Grading Using the Best Evidence Medical Education Guidance
The Best Evidence Medical Education (BEME) Collaboration has recommended Guide No. 13 for education practitioners designing systematic review. 23 This guidance advocates classifying the strength of evidence using a 5-point grading system, with Grade 1 being the lowest strength of evidence and Grade 5 being the highest when reporting systematic reviews (Grade 1: No clear conclusions can be drawn. Not significant; Grade 2: Results ambiguous, but there appears to be a trend; Grade 3: Conclusions can probably be based on the results; Grade 4: Results are clear and very likely to be true; Grade 5: Results are unequivocal.). This guidance was used by one author to grade the studies. In case of ambiguity, Center of Evidence-Based Medicine Evidence Levels were used to resolve the differences and arrive at final classification. 24
Statistical Analysis
Descriptive statistics were used to report sample sizes, study characteristics, and intervention formats. When reported by the original studies, pre-post intervention effect sizes and mean EI score changes were extracted for comparison. Effect sizes were interpreted as small (Cohen's d ≈ 0.2), medium (≈0.5), or large (≥0.8) following conventional thresholds. No meta-analysis was conducted due to heterogeneity in study design, outcome measures, and EI assessment tools.
Results
Participants and Interventions
Of the 4034 relevant citations found, 40 articles were included,10,25–62 encompassing a total of 2247 participants (1392 medical students, 578 residents, and 277 physicians). The majority of the studies were conducted and completed in the United States, accounting for 65.7% of the total. Thirty-three studies utilized an observational cohort study design, while 7 employed a randomized control trial design (RCT). The mixed EI model was used in 16 studies, the ability EI model in 8 studies, and the trait EI model in 8 studies. Around 49.1% of all the program participants were female. The average cohort size was 30 students.
Nineteen articles focused on medical students. The most common specialties of residents who participated in the interventions were internal medicine (n = 202), emergency medicine (n = 149), and general surgery (n = 124). Eight articles included physicians in their interventions, including those specializing in pediatrics, gastroenterology, hepatology, primary care, hematology-oncology, colorectal surgery, and head and neck surgery. Fewer than 50% of articles reported on age, ethnicity, sexual orientation, marital status, socioeconomic status, or prior leadership experience of participants. The most common pedagogical method was didactic/lecture-based learning, described in 56% (22/40) articles, followed by discussion-based teaching in 18% (7/40) and exercise-based teaching in 10% (4/40) articles. The duration of the interventions also varied significantly: 15% (6/40) were conducted in 1 day, 7.5% (3/40) were 1 day to 1 week, 10% (4/40) were 1 week to 1 month, 52.5% (21/40) were 1 month to 1 year, and the remaining 15% (6/40) extended beyond 1 year (Figure 3).

Frequency across key study characteristics. Legend: The studies contained a heterogeneous distribution of key study characteristics. Characteristics such as mean training program duration, follow-up time, geographic location, instructor background, curricular format, and main pedagogical methods were summarized. The majority of studies were US-based, 1 month to 1 year in length, in-person, and contained a mix of discussion and lecture-based learning. They were either internal or both internal and external faculty-led.
Risk of Bias
Of the 33 non-randomized studies (see Figure – Supplementary Digital Content 4), 3 (9%) were classified as having a low overall risk of bias. Additionally, 28 (85%) demonstrated a moderate overall risk of bias and 2 (6%) had a serious overall risk of bias. All seven randomized studies (see Figure – Supplementary Digital Content 5) were classified at low to moderate risk of bias.
Strength of Evidence and Best Evidence Medical Education Grades
Half of the studies addressing medical students (n = 10) were prospective cohort studies describing the intervention and its results on selected cohorts, which were considered to qualify for grade 3 evidence according to the BEME guide 23 (Table 1). The rest of the studies included four randomized controlled trials (Grade 5 Evidence), two non-randomized controlled trials (grade 4 evidence), and three cross-sectional studies (Grade 2 Evidence). Thus, n = 16/19 studies had moderate to strong levels of evidence (graded levels 3 to 5). Similarly, regarding studies that addressed the population of residents and physicians, we could find 16/21 studies with grades 3 to 5, including 3 randomized controlled trials and 3 non-randomized controlled trials (Table 2).
Analysis of Included Studies for Quality, Adherence to Best Practices, EI Interventions, Quantitative EI Assessment Tools Used, Post-Training Quantitative EI Improvement, and Effect Size.

EI, emotional intelligence; BEME, Best Evidence Medical Education.
Strength of Evidence According to BEME No. 13.

BEME, Best Evidence Medical Education.
Adherence of Training Programs to Best Practices
Nearly half (n = 10) of the included studies on medical students scored 2/7 on the scale of best practices formulated by adopting the best practices recommended in a previous systematic review. 22 Additionally, one study scored 6/7, one scored 5/7, two scored 4/7, and five scored 3/7 on the scale for best practices. Similarly, almost all studies on residents and/or physicians adhered to 2 or more best practices, with 4 studies adhering to 6/7 of recommended best practices (see Table – Supplementary Digital Content 6).
Quantitative Training Outcomes
Most of the included articles (n = 35/40) reported quantitative results, of which 24 reported solely quantitative results, while 11 were mixed-methods studies that also reported qualitative results (Figure 4A). Specially designed non-validated quantitative surveys were the predominant instruments to assess EI training outcomes for most Kirkpatrick levels except for outcomes related to EI skills (Level 2B) and participant performance (Level 4B), for which most studies used standard assessment tools. Various standardized instruments were used to demonstrate positive improvements in EI skills, including versions of Emotional Quotient Inventory (EQ-i), Jefferson Scale of Empathy (JSE), and MSCEIT. Likewise, various quantitative instruments were used to demonstrate positive participant performance increases, including stress levels, burnout levels, and mindfulness.

Summary of quantitative outcomes and measurement tools by Kirkpatrick scale. Legend: Instances of notable findings and positive outcomes in EI/EI subcomponents were organized by Kirkpatrick level and separated by quantitative (A) and qualitative studies (B). A total of 11 mixed-method studies, five qualitative-only studies, and 24 quantitative-only studies were found out of 40 studies. Quantitative results were reported as positive if the results were found to be statistically significant. Both flowcharts summarize all reported EI training outcomes, followed by the assessment tool used to measure each positive finding and the specific positive findings by Kirkpatrick level. The general trend of EI-related outcomes tended toward positive effects across all Kirkpatrick levels. Full forms for each EI measurement tool abbreviation may be found in the Appendix - Supplementary Digital Content 6. EI, emotional intelligence.
Quantifying the Effect of Emotional Intelligence Interventions
Of 32 studies that quantitatively reported the EI scores pre and post-intervention, 27 studies demonstrated an increase in any EI score or subscore. Versions of the Bar-On EQ-i were the most frequently used tool (n = 9), and a positive increase in the EQ-i score was revealed in 8 of the 9 studies, which ranged between nearly 4% and 8% improvement of the total EQ-i score. Statistically, the effect size for these EI interventions was likely to be medium or moderate, although small or large effect sizes were reported in a few studies. Fewer studies performed on residents and physicians reported the effect size compared to medical students and tended to report a lower effect size. Eight studies focused specifically on trait EI. Within this, 7 of the 8 studies found statistically significant improvement in trait EI over time (P ≤ .05). Overall, improvements in trait EI were similar to those in ability EI and mixed EI. No Trait EI improvements tended to be greater in the Attention and self-perceived Emotional Repair Scales.
Qualitative Training Outcomes
Overall, 16 articles reported qualitative results, including 11 mixed-methods studies and 5 studies reporting purely qualitative results. Seven studies reported qualitative results using a qualitative survey, often in the form of open-ended questions; semi-structured interviews were used in 6 studies; focused group discussions were used in 3 studies. Qualitative data were analyzed according to various methods, such as thematic analysis (n = 7), content analysis (n = 3), or grounded theory (n = 1). The positive findings according to various Kirkpatrick levels are shown in Figure 4B. Organizational benefits (Level 4A) were emphasized by three studies, with the main element of benefit being better team dynamics (n = 3). Personal benefits (Level 4B) were reported by 9 studies, mainly in stress management (n = 7). No study reported qualitative improvements in patient satisfaction (Level 4C).
Discussion
This study assessed first whether targeted EI training improves the EI and leadership skills of medical professionals and second, whether that translates into improved healthcare outcomes and found the following: 1) EI training programs are generally correlated with improvements in both overall EI and EI subcomponents, 2) Training programs lead to positive behavioral changes related to ACGME core competencies such as professionalism and interpersonal skills and 3) Improvements with EI due to training are correlated with improved physician well-being, resilience, and leadership skills.
This study provides novel insights into the most recent evidence regarding EI interventions in facilitating healthcare leadership and how they can be implemented more effectively, thereby filling important research gaps as the last systematic review on this subject was reported in 2014, 7 while a related systematic review was reported in 2018. 22 Furthermore, the findings from this review align with previous studies, such as Cherry et al, 15 that demonstrate the effectiveness of EI training on EI outcomes.
The present review examined the EI training effects across a broader range of medical professions, including those in the foundational stages of their careers, such as medical students and residents, and those in mature stages, such as practicing specialists (eg, surgeons, emergency physicians, pediatricians). The findings suggest that EI training is crucial in leadership development, regardless of the career stage. However, more studies focused on students and residents than on mature practitioners. It could be speculated that leadership skills inculcated early in the medical career may have a high likelihood of making a durable practical impact. Leadership places many demands on leaders, who are likely to face complex and challenging situations, often unexpectedly. 63 To navigate these situations successfully, a healthcare leader specifically needs to possess EI—which might be lacking in a physician—despite possessing plentiful general intelligence. The previous systematic reviews on the effect of EI training on physicians exclusively focused on medical students.14,15 Another review included studies on both students and residents. However, it did not discriminate between the nature of efforts made for EI training for residents or physicians versus those made for students. 7 It is necessary to examine the cohorts of medical students from those of residents and physicians because they are in different stages of their career trajectories and may need different interventions, according to the MLCF. 64 Therefore, a novelty of this systematic review is that nearly half of its included studies measured the effect of EI training on residents or attending physicians. Hence, this study could generate novel insights on the EI training interventions made for the more experienced physicians, such as residents and physicians, who have more independent and larger responsibilities in the healthcare system. Nevertheless, it is important to emphasize that attending physicians often need to work as a healthcare team; consistently, several studies performed on attending physicians included their coworkers, such as residents and nurses, which was not the case with studies performed on medical students.
Studies performed on residents or physicians tended to report more outcomes than those on medical students only. This could partly be explained by the fact that none of the studies including medical students, only evaluated outcomes related to organization (Level 4A) and patient care (Level 4C), perhaps because the students are not full-time hospital workers and do not have independent patient care responsibilities. These Kirkpatrick Level 4C findings are especially important as patient satisfaction remains the ultimate goal of all healthcare interventions.
Moreover, we identified several randomized and non-randomized controlled trials on the subject, which could not be identified in the previous reviews on this topic.7,22 Therefore, it could be emphasized that our findings indicate that the evidence base for the effect of EI training on medical students has shown improvement in numbers as well as the quality of studies being reported over time. In addition, the findings of scoring for adherence to best practices indicated that nearly half of the investigators of the studies that reached scores of 3 or greater have made serious efforts to make their programs effective. Notably, most reviewed studies reported adopting a longitudinal structure of interventions and using multiple teaching methods aligned with the principles of experiential learning. 22 However, some best practice recommendations remain neglected while designing the interventions, such as access to mentors and the use of external faculty.
Though all included studies covered EI training interventions, the training curriculum varied grossly between studies. Similarly, the effect sizes observed in these studies also varied greatly, although they mostly pointed to a benefit in terms of outcomes related to participants’ knowledge and behavior.
Numerous tools were used to assess the EI levels of participants in these studies, confirming the findings of previous reviews.7,22 Based on these findings, it can be suggested that EI interventions on medical students can likely improve their overall EQ-i 2.0 scores by as much as 10%. Thus, an EQ-i 2.0 score of 90-110 reflects an effective functioning skill, while that below 90 is too low, suggesting need for improvement; scores of 110-120 reflect enhanced skills, while those over 120 constitute an abnormally high skill. 58 In our review, only 8 studies specifically used the trait EI model. These studies demonstrated positive but more heterogeneous results, possibly reflecting differences in how trait EI is conceptualized and measured. By contrast, studies using ability EI or mixed models reported more consistent improvements, especially in Kirkpatrick Level 2B and 4B outcomes. These differences suggest that future programs may benefit from explicitly aligning their goals (eg, emotional self-awareness vs decision-making) with the appropriate EI model.
In this review, all studies on medical students reporting EQ-i 2.0 scores had scores between 90 and 110 both before and after the EI intervention. These findings suggest that the average EI levels of medical students may not be too low or high, although they can still benefit from EI interventions. Particularly, those with EQ-I 2.0 below 90 can be selected to optimize the benefits of the intervention. Five studies utilized the JSE to examine the efficacy of EI interventions in preventing the fall in empathy levels of medical students as they advanced in medical education, a phenomenon described in the literature. 37 Three studies in this review37–39 revealed that the JSE scores did not fall longitudinally after the EI intervention. Instead, their empathy either persisted or showed a marginal increase.
Furthermore, certain program features were associated with higher adherence to best practice guidelines and stronger reported outcomes. These included longer program duration (eg, ≥ 1 month), use of multiple teaching modalities (eg, didactics, reflection, simulation), and access to mentorship. Programs that integrated interdisciplinary learning and evaluated outcomes across multiple Kirkpatrick levels were also more likely to receive higher evidence grades. We recommend that future EI curriculum designers prioritize these features where feasible. Specifically, embedding longitudinal exposure, providing mentorship, and employing validated EI assessment tools may enhance both participant outcomes and organizational impact. The EQ-i 2.0 and MSCEIT appear to be particularly promising for measuring intervention effects.
Limitations
Our review has several limitations. First, despite being a systematic review, it is unlikely that we have evaluated all of the existing literature. A study by Hodzic 65 found significant publication bias/file drawer effects for EI training articles, suggesting that the reported meta-analytic effects would be considerably weaker if unpublished work were included in effect estimates. This raises an important question as to the implementation of EI programs—if many implemented programs are not being published in peer-reviewed journals, is it possible that effects are more negligible than previously thought? This possibility needs to be excluded by encouraging further meta-analytic work with unpublished datasets.
Second, though most included studies appealed to the benefits of EI training, a few found counteracting effects of such skill development systems. A further analysis of these findings and an extension into looking for contradictory evidence would have strengthened the main idea of the study. However, this review specifically focused on the efficiencies and impacts of the current EI training curriculum.
Additionally, the diversity in study designs, such as observational, quasi-experimental, and RCTs, and in the EI assessment tools, such as EQ-i, JSE, and MSCEIT contributes to substantial heterogeneity, limiting the generalizability and comparability of results.
Future Directions
One homogenous aspect was the voluntary nature of the samples in whom these effects were demonstrated; volunteers for medical studies tend to be higher performers, are more likely to receive medical licensing after completing their medical programs, and demonstrate higher certification rates. 66 Though a few studies showcased the efficacy of EI in non-volunteer samples,35,45 future research needs to explore whether EI training can be equally effective in non-volunteer populations.
A randomized controlled design for comparing specific EI approaches/components could help assess which components are the most necessary for programs to implement. Specific approaches, as alluded to previously, may include optimal sample size, duration, learning format, instructor, and curriculum content. This study could help medical training facilities and the public in general understand the “bare minimum” of material that would be needed to benefit medical professionals and, indirectly, patients. The effects of culture on program efficacy, participant race/ethnicity, age, and socioeconomic status may be important considerations. Assessing these effects in allied healthcare providers would be helpful as well. Although much of the recent work focuses on healthcare training programs for nurses and doctors, emergency service providers could be an important population to study.
As echoed in previous reviews on leadership and EI curricula,15,67–69 further studies that dive into the reported behavioral changes, organizational efficiency metrics, and patient benefits (Levels 3 and 4) can provide a deeper understanding of the current curricula and its outcomes. Financial considerations at the implementation and return of investment stages provide another dimension when developing an effective curriculum. Finally, a longitudinal study that measures the growth of leadership skills beginning from medical school would be valuable.
Conclusion
Our systematic review suggests that EI training is associated with an improvement in the EI and leadership skills of medical professionals, while its effect size varies from low to high in a multitude of studies. Curriculum designers aiming to implement EI training should consider integrating longer-duration programs, multiple teaching methods, and mentorship access. Emphasizing measurable outcomes aligned with validated EI models (eg, EQ-i 2.0, MSCEIT) may support standardization and comparability across institutions. Future work should consider formalizing the EI training procedure to determine precisely where institutions in healthcare can guide their workers toward more fulfilling and stable workplace environments. Additionally, formal studies are needed that examine the longitudinal effect of EI training spanning multiple career stages for single individuals and benefits at the patient and organizational levels. With this review, we continue encouraging the field to develop solid empirical work on identifying these strategies.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251380030 - Supplemental material for Systematic Review of Healthcare Curriculum for Training in Emotional Intelligence Within Physicians, Residents, and Medical Students
Supplemental material, sj-docx-1-mde-10.1177_23821205251380030 for Systematic Review of Healthcare Curriculum for Training in Emotional Intelligence Within Physicians, Residents, and Medical Students by Veda Chanda, Samhitha Buchireddy, Aditi Sawant, Sarika Yarrabolu and Utpal Bhalala in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
None
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous 3 years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.