
Abstract
Purpose
Traditional discussions of race-related health inequities in medical education often focus on the racialized individual, neglecting the role of systemic racism and other oppressive structures that drive resource inequities. Structural competency equips healthcare providers and trainees to critically analyze how structural racism creates health disparities.
Method
This study used focus groups with medical students (n = 56) and key informant interviews with faculty (n = 9) at a single academic medical center to explore experiences and perceptions of discussions about structural competency and the health effects of structural racism in small group learning communities. Activity Theory served as the analytical framework to understand environmental factors shaping these discussions, highlighting primary and secondary contradictions within the model activity system.
Results
The analysis revealed several tensions within the activity system that impacted discussions about race, structural racism, and inequities including, (1) questions of whether structural competency should be an explicit medical school outcome, (2) persistent biases in the curriculum, (3) faculty discomfort and limited expertise in leading discussions, (4) questions about who bears responsibility for facilitating these conversations, and (5) implicit and explicit rules shaping which types of knowledge are prioritized.
Conclusions
These findings inform the development of educational tools and faculty support strategies to enhance teaching and learning around structural competency in medical education.
Introduction
In medical education, race is often represented as an innate genetic determinant despite a lack of scientific evidence to support this characterization. 1 Traditional discussions of race-driven health disparities focus on the racialized person without accounting for racism and other forms of oppression that result in an inequitable distribution of resources, leading to poor health. This mischaracterization perpetuates harmful myths, contributes to health disparities, and has real clinical consequences. For example, a 2016 study revealed that White medical students and residents held false beliefs about biological differences between Black and White patients, which in turn influenced their clinical decision-making around pain management. 2 These issues reflect broader, systemic challenges in addressing structural racism within medical training.
Due to the national attention to a long-standing Black Lives Matter movement during the racial reckoning following the murder of George Floyd, the medical community has begun to examine structural racism in medical education and demand that race as a biological construct be removed from medical pedagogy.3,4 Organizations such as the AAMC 5 and AMA 6 have released statements that pledge to confront systemic racism and acknowledge racism and police brutality as a public health issue, following the lead of organizations like the APHA which declared law enforcement violence a public health issue in 2018. 7 As a result, medical schools have begun to integrate discussions of structural racism into traditional medical pedagogy using structural competency as a framework.8–11 Structural competency trains clinicians to recognize how upstream factors—such as housing policy, food systems, policing, and zoning laws—manifest in downstream health outcomes such as hypertension, depression, and trauma. In addition, to be structurally competent, one must also develop the skillset to generate strategies to respond to and address structural drivers of health, both in and beyond the clinic. 8
While structural competency has gained popularity in medical school curricula, there remains a critical gap in the literature: few studies have explored how discussions of structural racism unfold within the specific learning environments of medical schools. In particular, there is a lack of in-depth qualitative analyses that examine the contextual and relational dynamics influencing these conversations, especially within Learning Communities (LCs)—longitudinal, small-group settings designed to foster mentoring, identity formation, and collaborative learning.12–14 Like all communities, within the LC, there is a social and cultural context that impacts learning. 12 Though intended to be inclusive spaces for critical reflection and peer dialogue, LCs are situated within larger institutional cultures that may inhibit or shape discussions of race, power, and inequity in unexamined ways.
Contextualizing racism is essential to meaningfully identifying inequities and interrogating power structures within medical education and LCs. For this reason, we use the term minoritization rather than “racial or ethnic minority.” Minoritization reflects a socially constructed process, perpetuated by interlocking systems of structural oppression and shaped by societal perceptions of racial and ethnic identities. This framing emphasizes that disadvantage is not inherent to particular groups (eg, Black, Indigenous, people of color), but rather produced through systems that systematically privilege certain identities over others.15–17 In this context, present-day manifestations of structural racism may exert a shared influence across students with different generational or immigration backgrounds. 18 Further, perceived identity, how society identifies individuals, has been shown to be a powerful determinant of lived experience and access to opportunity. 19
In this project, we addressed a critical gap by examining the contextual factors that influence discussions of structural racism and structural competency within LCs at one academic medical center. We sought to understand medical student and faculty perceptions (thoughts, feelings) of the role LCs play in these discussions. We used Activity Theory 20 (AT) to analyze the contextual complexity in which medical students and faculty learn and interact within the LC. Activity Theory, more recently known as Cultural Historical Activity Theory, offers a framework for studying the “complexity of interactions between individuals and their environment by identifying the components of an activity system.” 21 A key component of AT as an analytical tool is its capacity to unveil contradictions, including “historically accumulating structural tensions within and between activity systems.” 22 Contradictions are “illuminative hinges through which participants in an activity can reflect on their activity system's developmental trajectory and understand its dynamics.” 23 Contradictions may help unveil tensions that undermine learning in the LC and also trigger opportunities for transformation and restructuring of the activity system (LC). Activity Theory therefore provides an ideal analytical tool to study the role that context might have in guiding conversations of structural competency and structural racism in the LCs.
The information identified in this study can further our understanding of medical student and faculty perceptions of an ideal learning environment to carry out discussions of structural racism, structural competency, and the contextual factors that influence these discussions. We hope to add to the literature on antiracism curricular efforts in the LC and to help medical educators develop tools for teaching structural competency.
Methods
This qualitative study was approved by the University of Kansas Medical Center Institutional Review Board as study #00146685.
Medical Student Focus Group Discussions: We conducted 9 Focus Group Discussions (FGDs) from August 2021 through December 2021 with students from the 8 different LCs at our institution. Inclusion criteria: Medical student at the University of Kansas Medical Center. Participants were recruited from a student population across 3 campuses. Students volunteered to participate in optional FGDs in response to recruitment emails distributed to student organizations. We used stratified random sampling to recruit students by LC, race/ethnicity, year, and campus. Students self-selected into focus groups labeled as “racially minoritized” or “nonminoritized” based on their own perceived experiences of race and structural inequity. Each FGD included 5 to 7 students and was composed of (i) racially minoritized students, (ii) White students, or (iii) Both racially minoritized and White students. We use the term racially minoritized to refer to students from racial and ethnic populations underrepresented in medicine who experience the present-day impacts of structural racism, and the systemic barriers embedded within medical education. 24 Our use of binary classification—minoritized versus nonminoritized—is intended as a pragmatic framework to describe students’ experiences within a medical education system shaped by structural racism. At our institution, the number of students from racially minoritized groups is small, and we are committed to protecting their confidentiality. Asking students to further describe their multigenerational identities, such as self or parental immigration status, would risk identification.
Key Informant Interviews with faculty: We conducted Key Informant Interviews (KIIs) June 2021 through November 2021 with faculty who facilitate LC discussions and serve as a Problem-Based Learning (PBL) case facilitator and coach. We used a purposive sampling strategy to recruit, via email, 9 LC faculty of diverse race, ethnicity, and gender identities.
Semistructured interview guide: The interview questions for both students and faculty focused on their perceptions of the ideal LC to discuss structural racism and environmental factors (race of faculty, gender of faculty, social context, political context, their socialization, knowledge, attitudes, and beliefs) that may impact the discussion.
Three racially diverse members of the research team who were experienced qualitative researchers (KB, NM, and MAL) facilitated the FGDs and KIIs via zoom. Key Informant Interviews were scheduled at participants’ convenience. Focus Group Discussions were conducted during a time that was determined to be mutually convenient for student volunteers. Students were not compensated. Students were told that they could sign off at any time during the call should they experience discomfort from the discussion. We also shared a resource with all students, in case they were uncomfortable, a staff psychologist (multicultural specialist). It's important to not, these discussions occurred within a sociopolitical climate marked by significant national discourse and support for diversity, equity, and inclusion. Written informed consent was obtained prior to both FGDs and KIIs. The sessions lasted approximately 60 min, were recorded with participants’ permission, and transcribed verbatim by a trained research assistant. Transcripts were checked for accuracy and completeness by a faculty team member.
Analytical Framework
Activity Theory: Activity systems are complex, multi-voice constructions that are continually transformed by the interactions of their elements. 25 The subject is oriented toward its object to achieve its outcome by means of mediating tools. The sociocultural setting that mediates this process is comprised of the rules and division of labor within a certain community. Community refers to the fact that subjects are members of social groups. 26 Tools are mediators of activity and can be classified as primary (ie, physical tools), secondary (ie, psychological), and tertiary (ie, cultural). Rules can be explicit (ie, length of class) or implicit (ie, paying attention while someone talks) and/or consistent with general social norms (ie, participating during class). Division of labor emphasizes that different members of a community contribute to the goal in different ways (Figure 1).

Visual Representation of Engeström’s Activity System. 25
Data Analysis
To operationalize Engeström's Activity System in the context of LCs at an Academic Medical Center, we used Mwanza's Eight-Step Model 27 to model the LC activity system. We employed a thematic analysis approach to analyze FGD's and KII transcripts to unveil contradictions within the Activity System of the LCs. The FGDs and KII transcripts were inductively coded using AT as the framework for analysis by 2 team members to establish intercoder reliability. Codes were categorized into initial themes and grouped into coding categories that reflect the topic areas of the questions asked. This process was iterative. A third member of the team independently reviewed the final codes and themes. All coders are familiar with structural racism, structural competence literature, and AT, thus helping them to recognize subtextual meaning within the transcripts. Thematic saturation was confirmed across 9 focus groups when 3 coders independently agreed that no new structural competence themes emerged in later discussions. Themes were discussed and interpreted among all 5 authors with the following positionality: MAL: Hispanic, White, immigrant, first-generation college graduate; CLF: Black American; MS: Black American, first-generation college graduate; NM: Black African immigrant; KB: White American.
Results
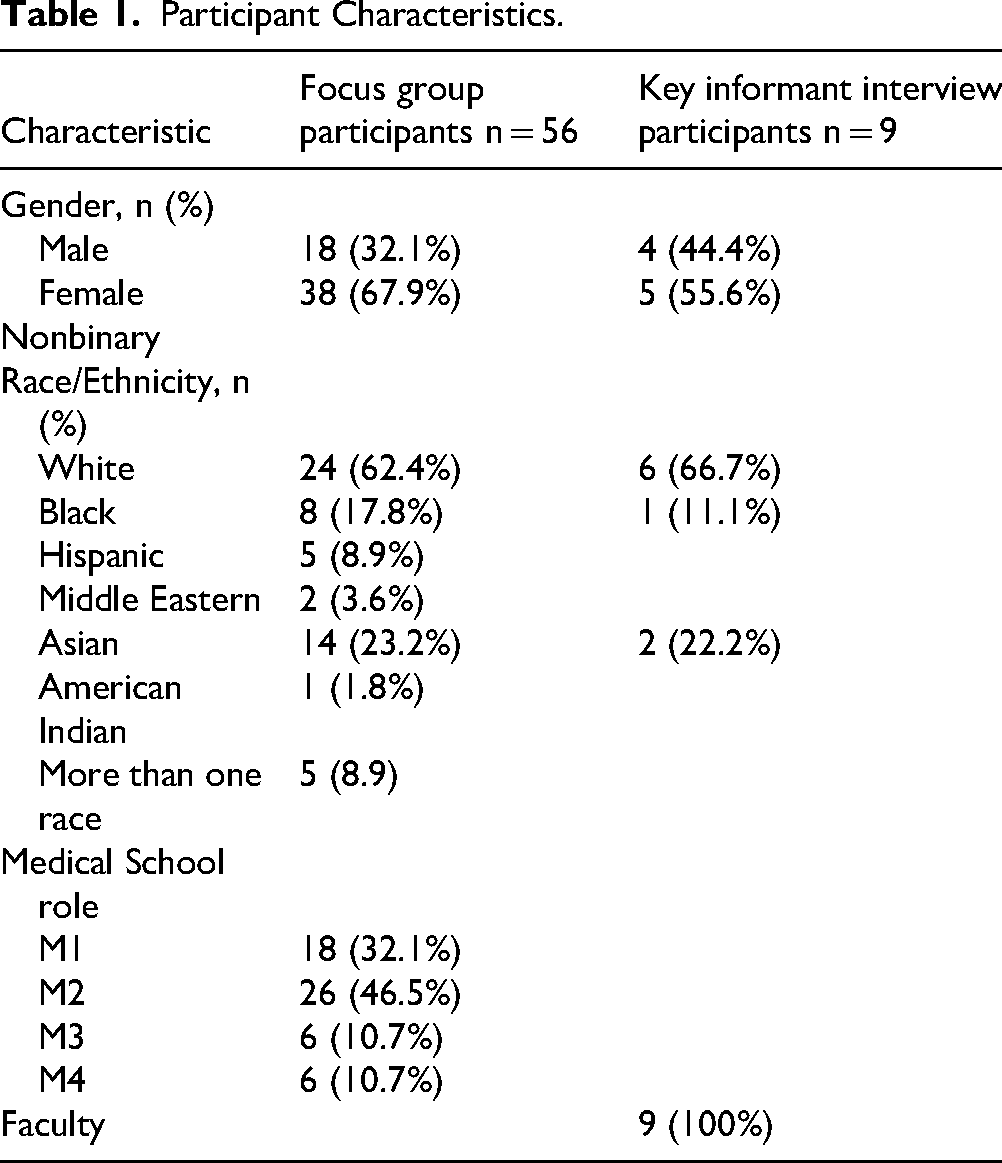
Participants were majority female (67.9%) and White (62.4%) (Table 1). Students from racial and ethnic populations URiM at our institutions were deliberately overrepresented in our study population compared to the medical school population of 20% URiM (unpublished internal demographic report).
Participant Characteristics.
Initial coding categories for the interview data were guided by activity system analysis, based on the subject, object, tools, rules, community, and division of labor concepts.28–30 Figure 2 provides a visual representation of the LC's Activity System.

Learning Community Activity System.
The subject(s) in the LC Activity System are the faculty who are formally “in charge” of the educational group, have a strong role in establishing the context (culture, norms etc), and are responsible for achieving the outcome.
The object is to graduate physicians who are structurally competent and ready to reduce health inequities (outcome).
The most prominent tool in the LCs Activity System is the curriculum, including PBL cases. Cognitive and psychological tools included faculty knowledge and beliefs about the goals of medical education and the relevance of structural competency and Diversity, Health Equity, Inclusion, and Justice (DHEIJ) content. Students also play a mediating role since discussion during small group didactics relies on their participation. Finally, the medical school culture is a mediating factor in the LCs activity system.
Students occupy a central position within the community as do the Offices of Medical Education, Student and Faculty Affairs, and Diversity, Equity, and Inclusion, as well as several key administrators who all share a common interest in the outcome and object of the Activity System.
The division of labor refers to both the division of tasks (initiating and contributing to the conversation) and the division of power within the LC.
Finally, both explicit and implicit rules were unveiled in this analysis. Explicit rules include assessments that regulate activity by defining expected outcomes, such as licensing exams (for which the required expectation is prioritizing content assessed within those exams), the format of the sessions (ie, PBL and Case-Based Collaborative Learning), and the timing and duration. Implicit rules are connected to the culture of medicine (ie, hard science more relevant than social sciences, dominant positivist discourses).
The FGDs and KIIs revealed preliminary themes within the activity system (Table 2).
Themes Within the LCs Activity System.

Abbreviations: DHEIJ, Diversity, Health Equity, Inclusion, and Justice; LC, Learning Community.
Primary Contradictions were defined as occurring within one Activity System component. Secondary Contradictions were defined as occurring between components within the Activity System. Table 3 provides examples of contradictions and their nature as well as exemplary quotes from the interviews.
Learning Community Activity System Contradictions.

Primary contradictions emerged within the community about the object (to graduate structurally competent physicians) of the system. Faculty often commented on the lack of clarity surrounding the purpose and need for conversations on structural competency, and students reported classmates openly questioning the value of these conversations and content. One faculty member noted a tension between checking off a list versus deeply delving into the topics, saying: … “there's really different goals in terms of the priorities of the session… is it the goal to get done *in the shortest amount of time to get the bare minimum of what the, for example, PBL writers wanted? Versus is this an opportunity to really dive into some really complex topic, you know, medication coverage and access? And what are the boundaries to getting rheumatoid arthritis treatment versus is it just to be like, well, the first line choice is fill in the blank medicine and check the box, move on to task number two.” (Faculty 1) “The point is to build skills, to be able to, to be able to think critically about this moving forward and being self-reflective. And I think if you've never had to practice that because we've made it so, you know, generic for lack of a better word” (Faculty 2)
It also became clear that there are tensions in understanding the object of LCs among members of the community with different identities as well as where the division of labor lies when addressing topics around the object. This was highlighted when a minoritized student voiced their concern: “But when that small group member says, I don't know why we have to hold these discussions about race and like sensitivity training, racial sensitivity training, all these things and they're looking at you, one of two minority members in that group. It really makes you think, right? It really makes you think like, do you?” (Minoritized Student 1) “when it says were there any racist implications. I feel like it's just kind of a token thing like we put it, we put it in there, so we're thinking about it.” (Nonminoritized student 1)
These sentiments were based on the perceived lack of prioritization of DHEIJ content reinforced by the (perceived) lack of time for this type of discussion and the need to move quickly through it to get to content perceived as core.
The interviews also revealed a clear lack of comfort by faculty in having conversations with students about structural competency. Participants expressed uneasiness with basic terms and a need for pedagogical tools to manage conversation in the classroom. One nonminoritized faculty member said, “I don't really have a good understanding of what is out there for what this person or that person or this group is talking about when they're discussing when they put those two words together (structural racism).” (Faculty 3)
Besides terminology, faculty reflected on how their own training did not address bias, racism, and other forms of social oppression and commented on tendencies to avoid such topics altogether as a result. One minoritized faculty member noticed that their colleagues lacked an understanding of the connection between historical racism, present-day inequities, and a meritocratic approach to American life, “And, you know, once you learn the history, then you can empathize. But I think people generally, have no idea about the history of the African-American people and what they have to deal with every day. And so they don't understand. They say this is the United States of America. This is the land of opportunity. The opportunities are there. Why don't you just grab them like everybody else?” (Faculty 4)
Additionally, faculty comments reflected disconnect between perceived “minor” (racial stereotypes or a lack of racial and ethnic diversity in medical cases) and “major” acts of racism (explicit racial discrimination or social oppression like mass incarceration of people of color). For example, one nonminoritized faculty member stated “Eliminating racist elements within the PBL, I think we were in many instances trying to create a mountain out of a molehill. Well, I think if you read books like The New Jim Crow, there are enough very obvious issues of structural racism within our society that we can actually address and deal with.” (Faculty 5)
Although LCs are supposed to be spaces where students reflect on all aspects of care during nonhierarchical conversations,
25
our analysis revealed major tensions regarding the division of labor within the LCs. Conversations revealed what appeared to be an unconscious division of labor when it comes to DHEIJ topics, with the onus placed on students of color to “educate” others on the topic rather than on the group to coconstruct knowledge as a community. Students of color felt the burden to lead conversations on DHEIJ topics and constantly advocate for minoritized groups regardless of their intersectional identities. White students expressed uncertainty that discussing racism was beneficial. One nonminoritized student stated, “these conversations can be unsafe and traumatizing for people. So, if one group of people like the white people in a group feel comfortable talking about racism in a way, like they may think that they're doing good by talking about it and bringing it up, but it can be harmful to people of color.” (Nonminoritized Student 2)
Finally, several implicit rules were uncovered during the interviews, particularly unspoken rules about how to “do and teach” medicine. Faculty felt pressure to “follow the company line” and focus on traditional epistemological approaches to what constitutes “science.” Participants’ comments revealed tensions between positivist paradigms and new frames of reference with several participants questioning and comparing DHEIJ content to “traditional science” or as one participant put it: “we listen to it because it's, quote, science. But it's not always, if that makes sense.”
Discussion
Equipping the next generation of physicians with the tools needed to improve equity in healthcare requires more than focusing on high-quality, evidence-based, guideline-directed care and enriching the curriculum with DHEIJ content. We must cultivate an environment conducive for both faculty and students to critically reflect and have open conversations about the intergenerational and intersectional impact of racism on present-day health inequities.
Despite the potential of LC's to be safe spaces to have challenging conversations about equity, our analysis revealed many environmental factors hindering structural competency discussions in the LCs, both from the perspective of students and faculty. Even highly motivated faculty members felt ill-equipped and unsure about the perceived value of these discussions within the culture of medicine.
Since structural competency curriculum content is relatively new, most faculty engaged in undergraduate medical education received their own training at a time when positivistic epistemological approaches to scientific knowledge were the norm. Medical faculty trained in positivist paradigms often favor clear-cut, data-driven topics such as anatomy or evidence-based medicine, while social and structural factors—such as racism—are downplayed as they are harder to quantify and don’t align with traditional scientific models. Therefore, many students entering medical school currently might feel more comfortable talking about structural inequities and racism than the faculty leading the discussions. In this study, we observed faculty members exhibiting disconnect between historical acts of racism and the intergenerational and intersectional impact of racism on present-day health inequities. There also appeared to be a disconnect between perceived “minor” and “major” acts of racism and a lack of understanding that both cause harm and should be addressed due to the combined and compounding effects of interpersonal and structural racism.31–33 The disconnect experienced by faculty might also reflect faculty attitudes and beliefs fostered by the culture of medicine, which values a positivistic rather than relativist or critical paradigm analyses. This culture, which elevates ideas of professionalism, including racialized and gendered norms implicit in the definition, 34 may be why some white students believe that antiracism discussions are not safe or even appropriate spaces for them. Though this work began in 2020, the current sociopolitical context around DHEIJ content may further widen this gap among faculty.
Consistent with the literature, many of the racially minoritized students in this study reported feeling “tokenized” or having to pay a “minority tax” by the implicit expectation they bear the burden of leading these conversations regardless of their intersectional identities or how connected they felt to the issue at hand. They thus face the risk of exposing themselves to vulnerability (having their experiences minimized), stereotyping (eg, angry Black women), racial fatigue (feelings of loneliness, anxiety, and depression), and burnout.35–37
Finally, although there have been recent calls for a greater emphasis on diversity, equity, and inclusion in medical education, including from the AAMC, 38 undergraduate medical education remains heavily focused on standardized assessments centered on biological and clinical content. This emphasis reinforces the false distinction between clinical and social excellence, implying that clinical competence can be achieved without addressing the structural and social contexts that shape health. We argue that this separation is problematic for both faculty and students and undermines efforts to prepare physicians who are truly equipped to advance health.
We make the following recommendations for medical schools working on antiracism-focused education, based on the perspectives of students and faculty in our study:
The mission and vision of the institution, its educational goals, and assessments should reflect the value that the school places on DHEIJ content. Institutions must ensure that antiracism practices are woven consistently through all they do rather than in isolated spaces. Institutions can add evaluation items for small group learning reflective of structural competency skills including (1) identifying the influences of structures on patient health and the clinical encounter; (2) generating strategies to respond to the influences of structures in the clinic and beyond; (3) describing and practicing structural humility in and beyond the clinic. Items on a rubric can send the message to both faculty and students that such skills do matter. Open the door to authentic knowledge exchange with colleagues in the humanities, particularly regarding assessment methods. Despite the momentum gained by the “health humanities” and their potential to enhance empathy and practitioners’ understanding of illnesses in their social context, methodological and institutional challenges persist for empirically measuring student performance.
39
Traditional assessment methods in medical education are heavily focused on multiple-choice questions that are not well suited to measure the skills that antiracism curricula instill in future physicians. Ensure the curricular tools that faculty use are free of bias and include learning objectives related to structural competency. There are free, publicly available tools to aid medical faculty in reviewing curricular tools and case studies for biased content.
40
Provide faculty with the knowledge and skills needed to facilitate conversations about structural racism. For instance, our Office of Faculty Affairs and Development offers a Race Talk Workshop focusing on facilitation skills that include knowing accurate and inclusive terms to use when discussing race and ethnicity, preventing and denying lived experience and gaslighting, and the ability to challenge inherited scientific paradigms that represent a biological model of race. Training should include how to critically review and interpret how race has been represented in scientific and medical literature and ways to address shortcomings. Faculty need to understand the history of racism in medicine and science that has contributed to present-day inequities and academic medical centers can offer such training.11,41 Promote a balanced division of labor by highlighting that DHEIJ work is everyone's work.
42
Faculty development should acknowledge the psychological challenges behind stifled speech or “white silence” including lack of confidence and powerlessness,
43
moral threat,44,45 and the fear and defensiveness of identity-based threat.46,47 All students need to see positive faculty role models who have overcome psychological and emotional barriers to proactively discussing racism with competence and humility despite their personal experience with present-day or multigenerational racial harm. Faculty and students could both benefit from shifting focus from how they are perceived in the group (fear of being called racist, fear of saying the wrong thing) to how they can contribute more to the discussion. Moving beyond defensiveness requires self-reflection, racial identity development, and a willingness to lean into discomfort rather than retreat from discomfort and abandon education. Faculty should be instructed not to rely on minoritized students to share their lived experiences as members of particular social groups.
48
Limitations
This study does not explore the contextual associations between racially minoritized students in the LC and nonminoritized students in the LC. The similarities and differences between the comments by minoritized and nonminoritized students need to be further evaluated in a future study. Grouping students by the binary framework of racially minoritized or nonminoritized may obscure nuanced distinctions in lived experience. For example, we have no data on multigenerational identities, such as immigration status, that impact personal narratives of racialized harm and gathering and reporting such data may risk identification of participants. Students opted into this study and represented a small sample of the student body. Our university hosts approximately 215 medical students over 3 campuses across the state. These students likely overrepresent students who see the value in discussing structural racism as part of their medical education. Additionally, the LC Activity System discussed in this study is unique to our institution and may not directly apply to other settings.
Conclusion
The next generation of physicians requires evidence-based tools, DHEIJ curricula, and an environment conducive to conversations that acknowledge health inequity and address resultant disparity. This study highlights opportunities to create LCs that integrate both the clinical and social mission of medicine by examining tensions and instituting structural and interpersonal interventions that resolve them with the ultimate objective of producing well-trained, structurally competent physicians.
Footnotes
Acknowledgments
The authors thank the students and faculty who participated in this study for taking the time to speak with us. The authors thank Breanna Kass for assistance with transcription and administrative support.
Ethical Considerations
This study was approved by the Institutional Review Board as study #00146685.
Consent to participate
All participants completed written informed consent before participating in focus groups and interviews.
Author Contributions
MAL: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing- Original draft preparation. KMB: Conceptualization, Investigation, Data curation, Writing- Original draft preparation. NM: Conceptualization, Methodology, Investigation, Writing- Original draft preparation. MLS: Conceptualization, Writing- Reviewing and Editing. CLF: Conceptualization, Supervision, Writing- Reviewing and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Academy of Medical Educators at the University of Kansas School of Medicine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Our informed consent form restricts the data usage solely to this current study, thus preventing its availability for use by other researchers. However, upon reasonable request, the in-depth interview guides utilized in this study can be provided.