
Abstract
Purpose
The addition of ultrasound training to undergraduate medical education (UME) curricula is on the rise. Despite widespread adoption, there is little focus on the learning theories that guide implementation or how student learning is transferred from one training setting to another. Using our school's UME ultrasound curriculum, we studied how changes implemented in the pre-clerkship curriculum (grounded in specific learning theories) influenced student learning and performance during clerkship rotations.
Materials and Methods
This was a retrospective study of an existing educational database of student responses and ultrasound submissions obtained during clerkship rotations. Data were collected using Qualtrics, de-identified, and exported to Excel for data analysis.
Results
After the curriculum change students reported requiring less assistance in the process of obtaining their ultrasound images while the quality of student obtained images remained the same. When broken down by clerkship, there were noted variations in image quality and need for assistance with students on the surgery clerkship showing the greatest increase in independence during the study period. Analysis of assistance by clerkship showed substantial differences in the type of assistance provided.
Conclusion
Theory-based curriculum change in the pre-clerkship setting can have a measurable impact on student learning behavior in the clerkship setting. The results of this quantitative study provide evidence to guide further qualitative research to better understand how students apply pre-clerkship learning experiences in the clinical environment.
Introduction
The design and execution of a medical school curriculum is a complex task. Medical school administrators and educators routinely acknowledge the impossibility of covering everything that is essential for future doctors to know before they graduate. Topics that need to be covered expand, while the time to teach them does not. It is therefore important that innovations and additions to the curriculum are assessed with explicit connection to the learning theories that inform them and the clinical environment in which they are used. A review of the literature demonstrates that this has not always been the case.
Ultrasound and other hands-on learning activities have grown in popularity as a part of early undergraduate medical education (UME) training.1–10 Studies have proliferated to evaluate the potential benefits of adding training to an already packed medical school curriculum.1,4,5,7,8 A 2018 to 2019 survey conducted by the Liaison Committee on Medical Education (LCME) found 95 of 131 (72.5%) of schools surveyed had included ultrasound in at least 1 year of training. 11 When surveyed, students report a desire for ultrasound training in the medical school curriculum.9,12–14 Wang et al 9 concluded that even without previous experience, students desire ultrasound training because they see the potential for application in their clinical practice. In their systematic review of the literature Davis et al 14 found that most studies describe stand-alone activities with success measured primarily in student satisfaction and pre-quiz post-quiz format. While this supplies information on the immediate impact of an ultrasound activity it does not provide data on how students might use these skills in future learning and practice.
Only a few studies report on long-term training, and even these studies focused more on curriculum implementation than on long-term learning outcomes.1,8 Hoppmann et al 8 describe a robust 4-year, integrated ultrasound curriculum at the University of South Carolina School of Medicine, but their description focuses primarily on the process of curriculum integration and student satisfaction without details on learning outcomes. Further absent from the ultrasound literature is the transfer of learning from one learning environment to another. 15 If the goal in teaching students how to use ultrasound is future application in a clinical context, then measuring the isolated skill of reproducing ultrasound images during a protected teaching session may be inadequate as it omits the realities of a busy clinical environment with multiple competing demands and sick patients.
Also lacking in the literature are discussions about why specific curricular decisions were made. Current published studies report what was done as part of an ultrasound curriculum initiative, rather than elucidating why a curriculum change was made. 16 Our literature review did not identify any discussions of UME ultrasound education that utilized specific learning theories to guide curriculum decisions. A stronger focus on educational theories that inform ultrasound curricular decisions would allow other educators to evaluate the value of implementing a similar approach and debate the relative merits of adding an additional curricular element in an already time-constrained UME schedule. There is no literature that describes either the impact of ultrasound teaching in the UME setting or how medical students integrate isolated teaching sessions into the larger context of their clerkship experience.
Given these gaps in the UME ultrasound literature, we sought to gain a better understanding of the utilization of our pre-clerkship ultrasound curriculum by students within the context of their broader medical education journey. Specifically, we examined how intentional changes in our curricular approach affected student actions during clerkship. We operated based on the premise that teaching a skill in the preclinical phase of learning was only valuable if it contributed to future learning and clinical practice. A recent change to our pre-clerkship ultrasound curriculum allowed us to examine how a theory-driven change in one portion of the curriculum influenced students’ learning and practice during clerkship ultrasound activities.
Background
In 2012 the Medical College of Georgia (MCG) began implementation of a comprehensive point-of-care ultrasound (POCUS) curriculum. In 2016 the curriculum expanded from a focus on pre-clerkship training to include core clerkship ultrasound requirements. During specified core clerkships, students acquired images relevant to each rotation (Table 1). All images were reviewed and graded by qualified ultrasound faculty. This longitudinal program was implemented across a distributed campus model throughout the state of Georgia serving over 200 students per class (Figures 1 and 2).17–19 Substantial resources—equipment, instructional hours, and faculty expertise—are devoted to this program. Initial student ratings that most studies focus on are useful, but long-term retention and application are the critical outcomes for judging whether such resource investment is justified. An ultrasound curriculum integrated throughout the entirety of medical school offers a unique opportunity to evaluate how teaching in the pre-clerkship phase influence students’ learning behaviors during clerkship rotations.

Ultrasound Educational Breakdown by Educational Year.

Medical College of Georgia Campus Locations.
Medical College of Georgia Core Clerkship Ultrasound Assignments.

In 2019 we revised the pre-clerkship ultrasound curriculum relying heavily on the educational theories of Kolb and Vygotsky to shape curriculum decisions. Using Vygotsky's Zone of Proximal Development (ZPD), the curriculum changes were designed to enhance students’ independent ultrasound use during clerkships and deepen their understanding of its integration into comprehensive patient care. While making targeted modifications to the pre-clerkship ultrasound curriculum, deliberate maintenance of clerkship requirements continued unchanged. This article outlines the theoretical framework behind the pre-clerkship curricular changes and evaluates their impact on student performance and application during clinical rotations.
Our school's Division of Experiential Learning was also created in 2019 and is responsible for guiding training in the areas of ultrasound, telemedicine, and simulation. Drawing on the educational theories of Dewey, Piaget, Kolb, and Vygotsky, the Division emphasizes active learning, reflection for the transfer of learning, and peer-to-peer interaction. 15 The theoretical orientation of the experiential learning teams focused on progressive skill developement. 20 Vygotsky's zones of development framework particularly informed an understanding of how medical students learned an entirely new skill while advancing from novices to independent practitioners. Vygotsky posited that learners move along a continuum of development or specific zones of development as they learn. 21 Initially a learner is completely unable to do a task or action, such as performing an ultrasound. Over the course of teaching interactions, learners move to the point where they can do a task with assistance, such as ultrasound with direct instruction. Eventually students are able to perform the task or skill independently. While ultrasound is the specific skill addressed in this article, an improved theoretical understanding of how curriculum influences skill development from novice to independent practitioner has direct relevance to other areas of medical training.
The pre-clerkship POCUS curriculum changes were specifically designed to prepare students for successful ultrasound application during clerkship (Table 2). Revisions relied heavily on the concepts outlined by Kolb and Vygotsky guiding students toward the increased independence required for clerkship.20,22 In our curriculum students initially progress toward independence in the relative safety of the classroom where foundational skills are evaluated and students benefit from hands-on feedback by an experienced faculty member. Clerkship represents a significant contextual shift, with greater autonomy, and daily interactions with real patients rather than standardized ones. By design, clerkship rotations offer less structure, and students are conferred greater independence in deciding how to pursue learning opportunities and complete the requirements of each clerkship. For the ultrasound requirements, support in this transition is provided through a structured image feedback system that delivers timely assessments and quickly identifies any missed clinically significant findings. The aim of our analysis was to evaluate student-reported need for help from others as they moved into the clerkship environment. Since the goal of the curriculum change was to help students become more independent learners, our analysis focuses primarily on how much assistance students reported while obtaining their images.
Legacy Pre-Clerkship Ultrasound Curriculum Compared to 18-Month Revised Pre-Clerkship POCUS Curriculum.

*Vascular access lab now being taught in another portion of pre-clerkship procedural curriculum.
Abbreviation: POCUS, point-of-care ultrasound.
Methods
This was a retrospective, observational research study that utilized an existing educational database of student ultrasound responses from clerkship rotations. Student responses were collected using the Qualtrics XM (Provo, UT) survey instrument. Students submitted 3 sets of still images for each clerkship assignment. Images were reviewed and graded by a single sonographer (BE) based on a scoring rubric (see Supplemental Appendix B for details of scoring rubric). Responses and ultrasound scores were exported to Excel (Redmond, WA) and de-identified prior to data analysis. The institution's IRB approved this study as exempt.
At the time of this study, the Medical College of Georgia had 5 regional campuses and more than 350 clinical sites across the state where students completed clinical rotations and were expected to complete their ultrasound images (Figure 2). Almost all sites utilized handheld ultrasound probes (Philips Lumify, Bothwell Washington) connected to Android tablets which were available for students to obtain images. In certain circumstances, students used hospital-owned equipment to obtain de-identified ultrasound images for submission.
During each rotation, students were required to obtain images and transmit these for review. There were no restrictions on whom students could consult for help to complete their ultrasound images, but they were required to obtain images from real patients. Accompanying the ultrasound images, students provided information about the patient presentation (no Protected Health Information (PHI) included), reported any help they received while acquiring their images, and commented on whether the assignment helped them understand how to apply screening guidelines to patient encounters (Supplemental Appendix A). All images were assessed by a single sonographer (BE) employed by the university who then sent feedback to students and reviewed images for pathology. If pathology was noted during review and was not identified by the student, then the student and faculty preceptor were both contacted, made aware of the findings, and provided with recommendations on how to discuss these findings with the patient. Since inception of this program over 10,000 sets of images have been submitted by students without adverse outcomes or patient harm.
Statistical analysis was performed in R9.4 (SAS Institute, Cary, NC). Nonparametric tests were used to compare the distribution of image scores in each clerkship (Wilcoxon Two-Sample Test). We performed a Shapiro-Wilk normality test on the distribution of the test scores, which rejected the normality (P < .01). Chi-square tests were used to determine association between the differences in the percentage of students who reported assistance in each clerkship rotation. Two sample t-tests were used to evaluate students’ rating of assignment helpfulness. Categorical variables, including need for assistance, were described as percentages and compared using the chi-squared test. Students were categorized as not requiring assistance only if they exclusively selected “No assistance required” (Figure 3 lists question from survey and the full survey found in Supplemental Appendix A).

Student Survey Reporting Assistance in Acquiring Ultrasound Image.
Results
Data from 198 students in the legacy curriculum from the MCG class of 2022 and 201 students in the revised 18-month curriculum from the MCG class of 2024 were compared. The class of 2023 experienced a hybrid curriculum during the transition and, during their second year, engaged in a remotely delivered curriculum due to the COVID shutdowns. Data from the class of 2023 served as a washout period between the 2 analyzed classes.
Comparison of Ultrasound Image Scores
Variation occurred in the total number of submissions received from different clerkship rotations and in submissions between the 2 years. The reasons for these variations are multifactorial and due to differences in how requirements are enforced at the clerkship level. Ultrasound image scores are listed pre and post curriculum change (Table 3 and Figure 4). Table 3 lists total number of submissions evaluated in each of the 2 classes broken down by clerkship. This data prompted changes to how individual students’ clerkship submissions were monitored. For example, real-time feedback was increased if a student did not submit all of their required images.
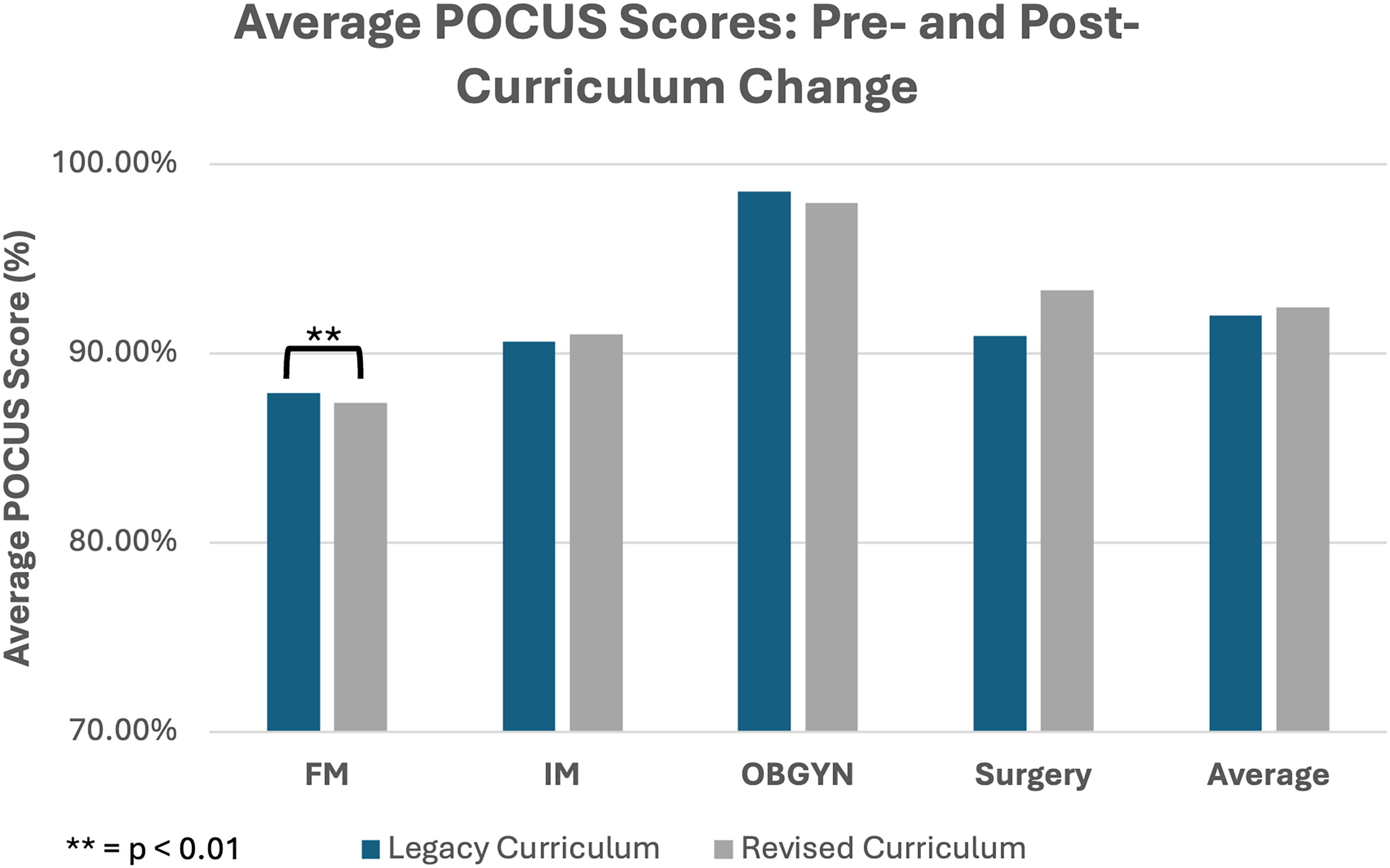
POCUS Assignment Scores for Each Clerkship Were Averaged and Compared Between the Legacy and Revised Curriculum Cohorts (Class of 2022 and Class of 2024). Abbreviation: POCUS, point-of-care ultrasound.
Ultrasound Image Scores Pre- and Post-Curriculum Change.
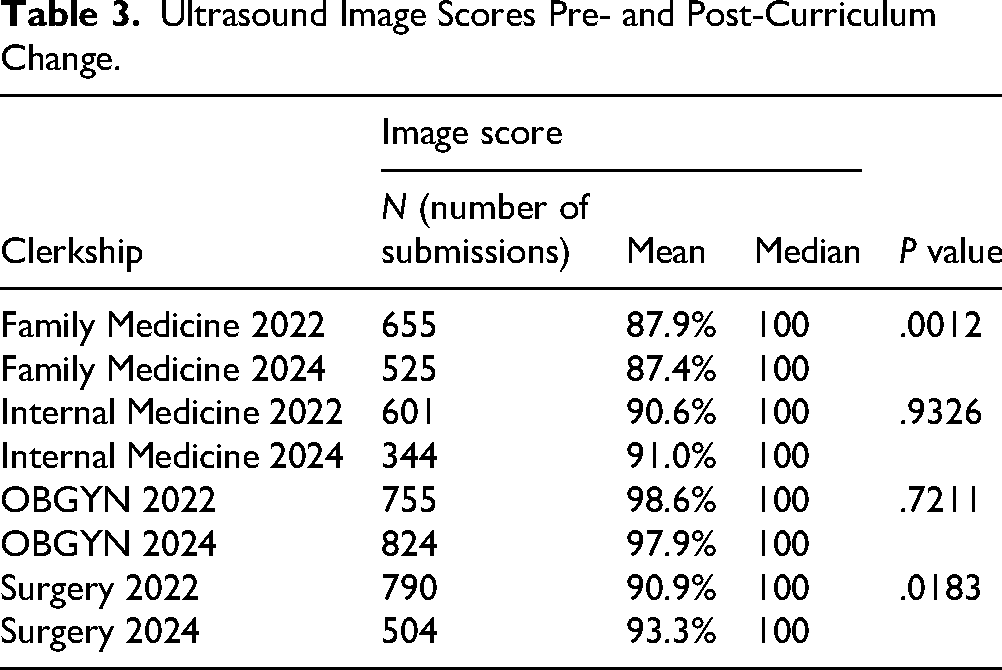
Nonparametric tests were used for statistical analysis. In the Family Medicine clerkship, a score change from 87.9% to 87.4% (P = .0012), indicated statistical significance, but a score change of 0.5 percentage points did not represent a meaningful shift in academic performance on a 4-item evaluation. OBGYN continued to have the highest average performance both in legacy curriculum (98.6%) and revised curriculum (97.9%). Surgery scores revealed positive change from 90.9% to 93.3%, but, as with Family Medicine, a 2.4 percentage change covering only 4 items (see Supplemental Appendix B) was not felt to represent a meaningful change in academic performance.
Amount of Assistance Required
After implementation of the revised curriculum there was a significant decrease in the percentage of students who reported the need for assistance while acquiring their ultrasound images (Table 4 and Figure 5). This decrease was consistent across all clerkships. Overall students reported they required less assistance, decreasing from 57% to 26%. OBGYN students continued to report the greatest need for assistance both before and after the curriculum implementation. Family Medicine, followed closely by Internal Medicine clerkship students reported the least amount of assistance required. The largest change occurred in the surgery clerkship with a 48.9% drop of students reporting a need for assistance acquiring their ultrasound images.

Student's Responses Were Dichotomized Into Received Assistance or did not Receive Assistance for Each Clerkship and Were Averaged for Comparison Between the Legacy (2022) and Revised (2024) Cohorts.
Percentage of Students Reporting Assistance While Acquiring Ultrasound Images.

Percentage (number of surveys submitted).
Abbreviations: FM, family medicine; IM, internal medicine.
Analysis showed that assistance received prior to the curriculum change was primarily peer-to-peer except in OBGYN where assistance came primarily from a sonographer (Figures 6 and 7). Following the curriculum change, peer-to-peer and faculty assistance decreased and the majority of students reported completing assignments without assistance. OBGYN was the exception as sonographers and faculty continued to assist most students.

Type of Assistance that Students Reported Receiving-Prior to the Curriculum Change.

Type of Assistance that Students Reported Receiving Following the Curriculum Change.
Assignment Helpfulness in Application of Screening Guidelines to Patient Encounters
Students ranked whether they found the ultrasound assignment helpful in understanding how to apply screening guidelines to patient encounters. Students were asked to rate the assignment on a scale of 1 (none) to 5 (a great deal) and mean rankings were compared (see Supplemental Appendix A for survey details). Students’ ranking scores did not show significant difference between the 2 periods (Figure 8).

Average Student Rating of Assignment’s Helpfulness in Understanding and Implementing Screening Guidelines by Clerkship.
Discussion
Integrating ultrasound into the UME curriculum requires substantial investments of time, resources, and faculty effort, making it essential to understand its true impact on student learning. In this study, we examined how preclinical ultrasound instruction influenced student behaviors during clinical clerkships, using ultrasound as a model to explore the broader issue of how learning transfers across educational contexts. Our primary aim was not simply to evaluate ultrasound training in isolation, but rather to consider how curricular activities in one environment shape performance and decision making in another. We view this as a necessary next step in UME scholarship—moving beyond descriptions of curricular innovations toward deeper analyses of how and when learning endures and transfers.
The question of “if” ultrasound should be universally included in the curriculum—a critical question with important implications for cost, access, and equity, is one that lies beyond the scope of our data. Our focus is on what occurs as a result of teaching: how learners’ behaviors evolve over time, particularly when measured at a significant distance from the initial intervention. Such outcomes are inherently more challenging to capture than immediate exam scores or knowledge-based assessments, yet they are essential for understanding lasting educational impact. By framing our findings through experiential learning theory and the zone of proximal development, we highlight the importance of adopting a long-term perspective when evaluating how students apply prior instruction in new clinical settings.
Current literature on UME ultrasound training is almost exclusively focused on evaluating self-reported student ratings of a learning experience and immediate ultrasound knowledge retention after the event.1,3–10,12–14,16 One study investigated long-term retention of general ultrasound skills, while another study described the general use of experiential learning techniques to aid in the transfer of learning.2,15 This current study is the first to apply experiential learning theory to ultrasound education and investigate how it influenced future student behavior. Medical knowledge is an important aspect of early medical school training, but these students must be equipped for life-long learning. Medical providers are increasingly confronted with new information and new technology they are required to integrate into their practice.
Fostering life-long learning means that educators guide students in developing foundational skills and creating safe environments for them to practice these skills independently, receive feedback, and reflect on their learning experience. Through this process (outlined by Kolb's experiential learning theory) students not only learn a specific skill but gain experience in learning independently while engaged in clinical care. Kolb's definition and outline of experiential learning focused on an iterative process of learning through experience.20,22 This is summarized in the frequently used phrase, “learning is a journey and not a destination.” In medical education, and education in general, the focus is often on measuring outcomes. Kolb focused on learning as a continuous process rooted and grounded in experience and reflection. Additionally, in Kolb's model, each student is provided identical information but engages in a unique learning experience where they reflect and apply experiences that establish life-long learning. Kolb is not the only theorist that supports a dynamic approach. The master adaptive learning approach developed by Ross et al 23 is based on similar concepts. Ross et al 23 provides a compelling case for an approach focused on adaptive, self-regulated learners which is essential for CBME to succeed and promote students’ long-term skill and knowledge retention.
Data analysis for this study focused specifically on the students’ shift in the clinical environment from assistance towards independence. Of particular interest was how students increased independent learning, as this most authentically approximated the type of learning they will engage in after graduating from residency. Gaining a nuanced understanding of which foundational training helps students learn independently has important implications for how to prepare students for entering the clerkship environment and how to prepare residents for attending practice.
The reduction in assistance reported by students across all clerkship experiences suggests that students were more prepared to perform ultrasound independently after our curriculum changes. Performing clerkship level ultrasounds on real patients involved a significant increase in complexity (eg, deciding which patient to scan, obtaining consent, acquiring images, and interpreting images to be normal or abnormal) compared to scanning standardized patients or fellow students in a controlled classroom environment. Navigating this change was essential for students to apply classroom clinical skills to the bedside. The observed increased independence suggests that our intentional curriculum changes helped move students further along the zone of proximal development (ZPD). This move brings them closer to self-regulated learning which will be important as they move into residency and attending practice where there are fewer objective assessments and a greater focus on self-directed learning.
The OB/GYN clerkship saw only a minimal change in the number of students reporting assistance while the other clerkships had a reduction of over half. This can be explained by 2 main factors. The first is that the OB/GYN ultrasound training was removed from the pre-clerkship curriculum, so students have minimal exposure to this prior to entering clerkship and little chance to progress through the ZPD in this skill. The second, and more relevant factor, is because students are performing ultrasounds on pregnant women and all these exams are done under the direct supervision of an ultrasound tech or faculty member/resident (see Figures 6 and 7). This creates fewer opportunities for students to scan independently and is likely the reason that OB/GYN imaging scores are consistently the highest. Students have the opportunity for an expert to review and correct their images prior to submission. Our decision to remove OB/GYN from the pre-clerkship curriculum was primarily based on challenges in recruiting enough pregnant SPs to adequately train 250 students prior to clerkship. Currently, there are no specific plans to modify the curriculum to push this training earlier. However, our findings indicate the existing approach would result in moving OB/GYN students toward independent scanning further in their training journey, during residency.
Family medicine (FM) clerkship rotations consistently had the lowest opportunity for students to interact with faculty or residents who were trained in ultrasound. Most students rotated in community practices where family medicine faculty had ultrasound machines (made available for these medical school clerkship assignments) but no formal ultrasound training. 17 Students rotating in a family medicine outpatient office saw more patients 1:1 with an attending and had an opportunity both in ultrasound and in their clinical experience for increased independence. For both pre- and post-curriculum change students reported the lowest need for assistance during their FM clerkship.
Interestingly, these findings show students were divided on whether ultrasound assignment was a helpful way for them to understand specialty-specific screening guidelines. Each clerkship ultrasound assignment was crafted to connect directly to screening guidelines for that specialist. For example, abdominal aortic aneurysm (AAA) screening in designated patient populations is recommended during primary care visits. There are several possible reasons students failed to make connections. A mean score in the neutral range (Figure 8) suggests these connections may not be as clear to the students as they are to the faculty and instructors who have a broader perspective of ultrasound integration into clinical care. Students may not make connections simply because the connection is not made explicitly during instruction. Lastly, the ratings in this area may reflect the greater challenge of navigating learning tasks in a complex clinical environment. The single survey item raises further questions about clinical integration, but this one question is too limited to draw any definitive conclusions.
Experiential learning theory helps identify major areas of focus and opportunities for growth. 20 The theory suggests that student reflection on a learning experience will impact experimentation and incorporation of it into future learning. Knowing this emphasizes the importance of supporting students as they gain independence and assisting them make explicit connections between ultrasound and clinical practice.
While we emphasized that a specific goal or endpoint is not the focus of experiential learning, the image quality scores should not be fully ignored. Integrating ultrasound into clinical practice requires 3 fundamental steps:
Image acquisition (acquiring high-quality images) Image interpretation (normal vs abnormal) Clinical integration (application of findings in the context of the specific patient presentation)
If a learner cannot acquire appropriate images, then they will never be able to interpret them or integrate them. While image scores were not the focus of the ultrasound training, it is essential to monitor students’ ability to acquire accurate images. Following the curriculum change there was little variation in students’ image scores. Scores were quite high prior to the change and remained high after the curriculum change. The stability of imaging scores was reassuring and indicates that students continued to acquire images successfully but with less help. Our curriculum change was not designed to improve image acquisition scores but the stability of scores served as a quality check to curriculum changes.
Limitations
The data acquired for this educational project was self-reported by students. We could not verify how much assistance (if any) they received. Additionally, ultrasound scores do not influence clerkship grades and students receive full credit for completing the assignment regardless of image quality. Some students may have asked for less help in the name of expedience without attention to how “good” their images were. More independence in and of itself does not mean that students were fully invested in the experiential learning cycle. More research needs to be done in this area.
We were limited to using students’ ratings of how helpful this assignment was in applying screening guidelines. We were forced to make assumptions about how they interpreted this question and framed their answers on a 5-point scale. Future research utilizing a qualitative approach based on student interviews would clarify how students view and reflect on their ultrasound training as part of a larger clerkship experience.
The 2 study periods were separated by over a year of transition time, and there were many other changes that occurred both in the curriculum and in clinical care in the post-COVID era. We could not fully account for or control these changes that may have influenced how students completed their ultrasound assignments. Although no changes were made to the clerkship assignments between study periods, the stability of image scores suggests a comparison of the 2 time periods was a reasonable approach. In addition, sampling the same students across 4 different clerkship experiences adds veracity to the study.
The lens used to analyze this data was very specific, focused on Vygotsky's ZPD and experiential learning theory. As such, the data and trends were influenced by this frame of reference. These theories were used in redesigning the curriculum and were appropriate to use in the analysis. However, there are many other learning theories and approaches that could be applied to this data with different conclusions. Our analysis is not meant to convey the absolute truth but to highlight one way in which learning theory can be put into practice.
Our focus on learning theory and the Zone of Proximal Development (ZPD) as frameworks for evaluating behavior change means we were not able to address all aspects of ultrasound implementation. While ultrasound integration is expanding across UME curricula nationwide, critical concerns around equity, resource allocation, equipment costs, and safety protocols require dedicated study. The scope of this article and our current data prevent detailed examination of these considerations, though we plan future publications to address them based on our extensive experience implementing a statewide program that serves students training in rural and underserved communities.
Conclusion
Medical education innovation does not occur in a vacuum. It is essential to understand how curriculum changes influence future learning. Training clinicians to work in complex medical environments requires assessments focused on how learning transfers between contexts and moves beyond testing information delivered at a single point in time from a controlled environment.
Experiential learning theory highlights the importance of contextualizing learning within students’ broader experiences. Curriculum decisions grounded in theory provide deeper insight into long-term impacts and allow for analysis that moves the focus from what students know to what students do. Our research demonstrates students’ progress along the zone of proximal development as they transition from pre-clerkship to clerkship, maintaining ultrasound skills while gaining independence, preparing them for application in residency and beyond.
Future qualitative research exploring the student perspective on ultrasound application in clerkship could more clearly illuminate the reflective process that students engage in when applying a skill to a new situation.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251378849 - Supplemental material for Clinical Learning in Translation: Analysis of Pre-Clerkship Ultrasound Training on Student Learning Behaviors During Clerkship
Supplemental material, sj-docx-1-mde-10.1177_23821205251378849 for Clinical Learning in Translation: Analysis of Pre-Clerkship Ultrasound Training on Student Learning Behaviors During Clerkship by Daniel Kaminstein, Nicholas Orris, Erin McBride, Michael Bowler, Lifang Zhang, Hongyan Xu, Rebecca Etheridge, Ann-Marie Kuchinski and Matt Lyon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251378849 - Supplemental material for Clinical Learning in Translation: Analysis of Pre-Clerkship Ultrasound Training on Student Learning Behaviors During Clerkship
Supplemental material, sj-docx-2-mde-10.1177_23821205251378849 for Clinical Learning in Translation: Analysis of Pre-Clerkship Ultrasound Training on Student Learning Behaviors During Clerkship by Daniel Kaminstein, Nicholas Orris, Erin McBride, Michael Bowler, Lifang Zhang, Hongyan Xu, Rebecca Etheridge, Ann-Marie Kuchinski and Matt Lyon in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors would like to thank Billy Bruss for the help with research coordination and Maggie Needham for preparing and submitting this article for publication.
Two of the authors, NO and EM, were in their final year of medical school when this manuscript was conceptualized, written, and submitted. At the time of publication, they have each graduated and are now in their first year of residency training.
Ethics
There are no ethical or financial conflicts of interest in connection with this article. This study received ethical approval, IRB 1285120, and determined as exempt from IRB review by the Augusta University Committee B Internal Review Board.
Author's Contribution
DK, ML, RE, NO, EM, AMK, and MB conceptualized, designed, and participated in the analysis, and initial writing. DK and AMK took primary responsibility for editing and finalizing the manuscript. NO, EM, and MB performed the initial data analysis and literature review. LZ and HX guided statistical analysis, interpreted data, and contributed to writing. DK, RE, and ML were responsible for guiding the ultrasound curriculum revision and RE reviewed all student ultrasound submissions. The authors declare accountability for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and analyzed during the current study are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.