
Abstract
Objectives
The COVID-19 pandemic has underscored the importance of equipping medical specialists from various fields with anesthesiology skills that are essential for medical practice, such as managing acute and chronic pain, preventing substance dependence, caring for critically ill patients, and ensuring airway security. This study analyzes the presence of these anesthesiology competencies in the curricular frameworks of medical residency programs in Brazil, Spain, and the United Kingdom, all of which have universal healthcare systems, to assess how effectively these programs prepare future specialists with these crucial skills.
Methods
We analyzed curriculum frameworks for medical residency programs and specializations in all 3 countries, focusing on anesthesiology competencies. All relevant documents, available on official government websites, were reviewed between July 1, 2023 and December 28, 2024, using Kripka's methodology.
Results
Significant differences were found in competencies related to stratifying anesthetic-surgical risk (P = .027), recognizing and analyzing palliative care (P = .023), mastering the basics of conscious sedation (P = .009), multidisciplinary teamwork (P < .001), and mastering the technique of local anesthesia (P < .001). Despite these differences, the number of anesthesiology competencies was similar across all 3 countries.
Conclusions
This study identified a potential gap in resident training for crucial skills such as pain management, sedation, airway management, and hemodynamic monitoring. These are essential for high-complexity procedures. The findings suggest a need for curriculum revisions and potentially an increase in specialty program slots focused on caring for critically ill patients.
Introduction
Medical practice, encompassing the development of the doctor-patient relationship and technical procedures within a social context, 1 aims to improve human quality of life through preventive measures to avoid illness, therapeutic interventions to treat pathologies, and palliative care to alleviate suffering when a cure is not feasible. 2 It spans all stages of life, from birth to death, and can be applied individually or collectively. In exceptional situations, such as pandemics, medicine must address underlying conditions, requiring the application of competencies acquired throughout undergraduate and postgraduate education to ensure comprehensive and effective care.
The COVID-19 pandemic highlighted the need for a global healthcare workforce with standardized competencies across all countries. 3 Such standardization would enable more effective responses in the most affected regions. The critical need for specialized medical training also became evident, particularly in managing patients with severe respiratory failure syndrome requiring oxygen therapy. 4 Oxygen delivery can be administered noninvasively, using nasal cannulas and noninvasive positive pressure ventilation in milder cases, or invasively through tracheal intubation in more severe cases—a procedure that requires advanced airway management, an essential skill of specialized professionals such as anesthesiologists, surgeons, intensivists (critical care physicians), and emergency physicians. 5
The management of critically ill patients requires a multidisciplinary approach that begins at the primary care level and extends through emergency services to intensive care. This includes the establishment of care protocols and response systems, such as rapid response teams for tracheal intubation and the use of extracorporeal membrane oxygenation (ECMO). 6 Countries with well-developed healthcare systems—characterized by adequate surgical infrastructure, intensive care units, diagnostic resources, and professionals trained in airway management—achieve better outcomes in the treatment of critically ill patients compared to those with limited surgical capacity. 7 This underscores the relevance of specific technical skills in anesthesiology, not only within the specialty but also as core competencies for physicians in fields like emergency and intensive care medicine, where airway management and sedation are required.
Although anesthesiology workforce shortages are documented in many countries, the United Kingdom (UK), Spain, and Brazil were specifically selected for this study based on two main criteria. First, all these countries have publicly funded universal healthcare systems, which provides a shared structural basis for meaningful comparison. Second, they represent distinct economic and regional contexts that are relevant to the global surgery agenda: the UK is a high-income country with a centralized National Health Service (NHS) 8 ; Spain is an upper-middle-income country with a decentralized public health system, the Sistema Nacional de Salud (SNS) 9 ; and Brazil is a middle-income country from the Global South, characterized by regional disparities in access to care and provision through its public health system (named Sistema Único de Saúde – SUS). 10 These contrasts allow for a comparative analysis of how different public healthcare systems address the training and distribution of anesthesiology professionals under varying socioeconomic and institutional conditions.11-15
In the context of global surgery, which is defined as the study and practice of improving access to timely and quality surgical care, essential medical skills include perioperative care; acute and chronic pain management; palliative care; intensive care; and obstetric, pediatric, and geriatric patient management. 2 These skills constitute some of the competencies necessary for the training of a specialist in anesthesiology; although general practice may encompass a variety of these fields, accurate practice requires advanced training in subspecialty. 8
Since anesthesiologists play an active role in surgical procedures—which are essential for treating one-third of the global disease burden—it is important to conduct studies that examine the relevance of competencies related to surgical specialties, including anesthesiology, in medical education and clinical practice worldwide. 2
In this study, we conducted a comparative analysis of the curricular frameworks of medical residency programs, with a focus on anesthesiology, in Brazil, Spain, and the UK.9,10,16
Methods
Data Collection
A documentary analysis of the curriculum frameworks in medical residency programs and practical training was conducted by 2 independent investigators in a blinded manner, following the sequence illustrated in Figure 1. They examined documents available on the websites of the Brazilian Ministry of Education and Culture, Federal Council of Medicine of Brazil, the United Kingdom General Medical Council, and the Spanish Ministry of Health. The study was conducted from July 1, 2023 to December 31, 2024, using the approach proposed by Kripka. 17 This study adhered to ethical guidelines even though it does not require ethical approval due to research in open databases.

Summary of the Data Collection Steps.
Competency Categorization
The anesthesiology residency program in Brazil follows a structured curriculum, comprising 19 competencies in the first year, 13 in the second year, and 17 in the third year. By the end of the program, residents will have acquired a total of 49 competencies. Some competencies are introduced in the early years with a focus on acquiring fundamental skills and progressively increase in complexity throughout training. For example, in the first year, residents learn to gather essential information during preanesthetic evaluations; in the second year, they progress to assessing and planning anesthesia for medium and minor surgeries; and in the third year, they are expected to fully master the preanesthetic evaluation, including patient guidance and the preparation of a final medical report. The analysis identified 27 core anesthesiology competencies to examine their presence in residency programs across Brazil, Spain, and the UK. These competencies were systematically documented in an Excel spreadsheet (Microsoft Office 365, version 18.2405.1221.0) for comparative analysis.
Data Analysis
Frequencies and percentages were calculated, and comparisons between proportions were made via the chi-square test, with a significance level set at P < .05. All graphs and tests were performed using the GraphPad Prism 8.0.1.
Results
Analysis of Medical Residency Programs
First, we investigated the number of medical residency programs of all specialties available in Brazil, Spain, and the UK. Brazil has 55 medical residency programs in specialties and 46 in areas of practice, according to the Brazilian Ministry of Education and Culture and Federal Council of Medicine, totaling 101 programs. For comparison, the General Medical Council of the UK offers 65 residency programs in specialties and 31 in areas of practice, totaling 96 programs, and the Spanish Ministry of Health offers 59 specialty residency programs. The analysis yielded 27 competencies for comparing anesthesiology with other residency programs, as shown in Table 1.
Anesthesiology Competencies After Categorization.
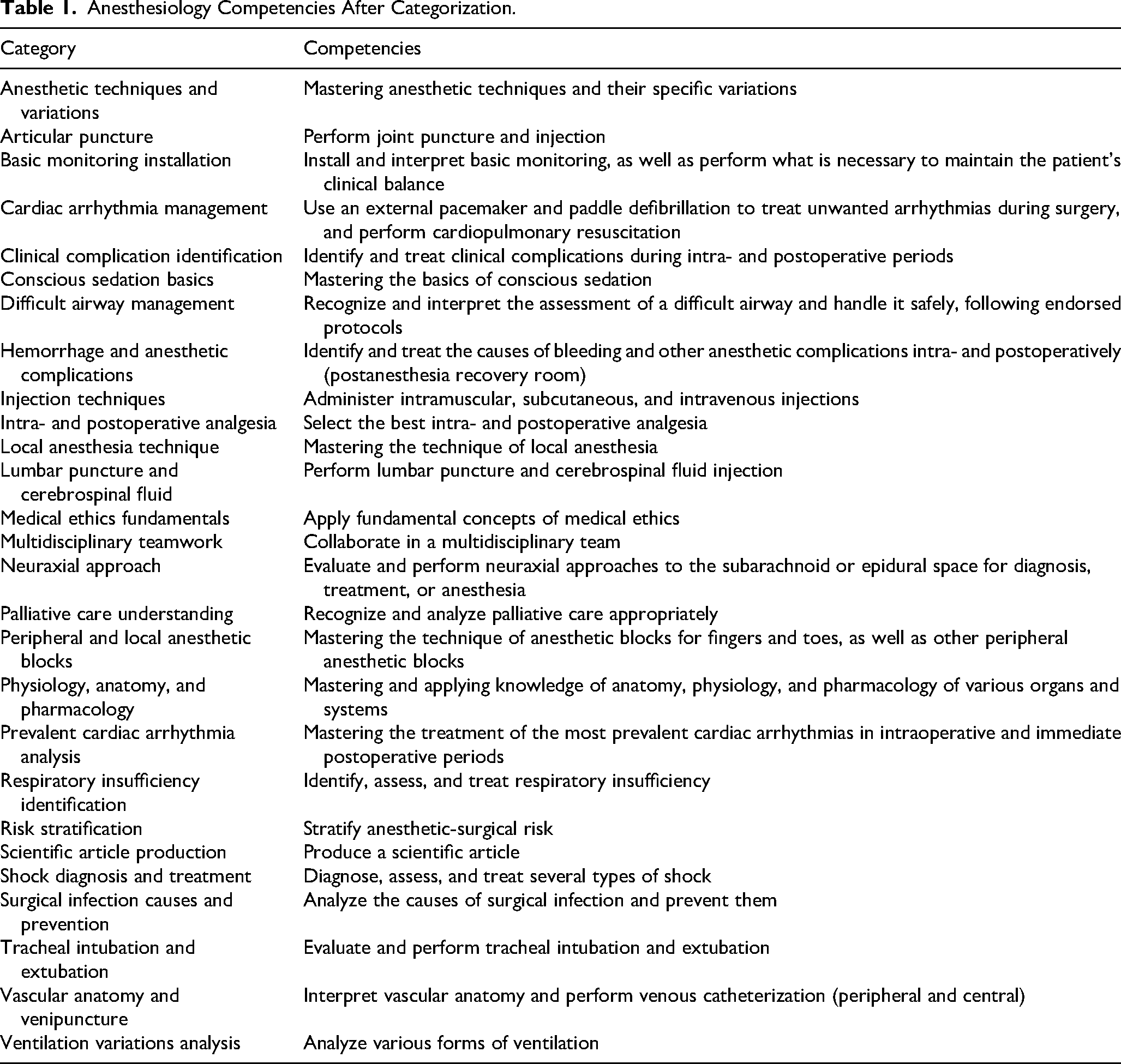
These 27 categorized anesthesiology competencies were identified within the curricular frameworks of 256 medical residency programs across Brazil, the UK, and Spain via binary classifications of “Included” (present) and “Not included” (absent). These competencies were systematically grouped into 5 categories: theoretical knowledge, foundational skills, sedation and analgesia, intensive care, and airway management. Table 2 presents a detailed summary of the findings, including the absolute frequencies, proportional percentages, and associated P values for each category.
Distribution of Anesthesiology Competencies Across All Medical Residency Programs in Brazil, Spain, and the United Kingdom.

Analysis of General Competencies
These competencies were prevalent in the majority of the medical residency programs investigated. The competencies “Apply fundamental concepts of medical ethics,” “Produce a scientific article,” and “Collaborate in a multidisciplinary teamwork” were present in between 87% and 100% of the residency programs of Brazil, Spain, and the UK (Figure 2A-C). The competency “Mastering and applying knowledge of anatomy, physiology, and pharmacology of various organs and systems” was also present in more than 82% of the residency programs, except for Spain, in which it was present in 67.8% of the programs (Figure 2D).

General Competencies Included in Residency Programs Across Brazil (n=101), Spain (n=59), and the United Kingdom (n=96), Totaling 256 Programs. The Y-Axis Represents the Percentage of Programs in Each Country That Include the Given Competency. The Competencies Analyzed Were: (A) Application of Fundamental Concepts of Medical Ethics (Brazil: 95 Programs, 94.1%; Spain: 58 Programs, 98.3%; UK: 96 Programs, 100.0%; P=0.03); (B) Production of a Scientific Article (Brazil: 93 Programs, 92.1%; Spain: 58 Programs, 98.3%; The United Kingdom: 96 Programs, 100.0%; P=.007); (C) Collaboration in Multidisciplinary Teams (Brazil: 88 Programs, 87.1%; Spain: 56 Programs, 94.9%; The United Kingdom: 96 Programs, 100.0%; P < .001); and (D) Mastery and Application of Knowledge in Anatomy, Physiology, and Pharmacology of Various Organs and Systems (Brazil: 83 Programs, 82.2%; Spain: 40 Programs, 67.8%; The United Kingdom: 80 Programs, 83.3%; P =.045). All Data Were Analyzed Using the Chi-Square Test. “Included” and “Not Included” Responses Were Compared.
Analysis of Basic Competencies
The competencies examined in this section are integral to the core skills of an anesthesiologist. However, the findings revealed a lower representation of certain competencies, with statistically significant differences observed across the three countries analyzed. The competency “Stratify anesthetic-surgical risk” was present in only between 32.2% and 51.4% of the residency programs of Brazil, Spain, and the UK, whereas the competency “Recognize and analyze palliative care appropriately” varied between 18.6% and 39.6% of the evaluated curricula, as shown in Figures 3A and B.

Basic Competencies Included in Residency Programs Across Brazil (n=101), Spain (n=59), and the United Kingdom (n=96), Totaling 256 Programs. The Y-Axis Represents the Percentage of Programs in Each Country That Include the Given Competency. The Competencies Analyzed Were: (A) Stratify Anesthetic-Surgical Risk (Brazil: 52 Programs, 51.5%; Spain: 19 Programs, 32.2%; The United Kingdom: 35 Programs, 36.5%; P =.027); (B) Recognize and Analyze Palliative Care Appropriately (Brazil: 40 Programs, 39.6%; Spain: 11 Programs, 18.6%; The United Kingdom: 30 Programs, 31.2%; P=.023); (C) Administer Intramuscular (IM), Subcutaneous (SC), and Intravenous (IV) Injections (Brazil: 44 Programs, 43.6%; Spain: 17 Programs, 28.8%; The United Kingdom: 22 Programs, 22.9%; P =.007); (D) Mastering the Technique of Local Anesthesia (Brazil: 36 Programs, 35.6%; Spain: 6 Programs, 10.2%; The United Kingdom: 10 Programs, 10.4%; P < .001); (E) Mastering the Treatment of the Most Prevalent Cardiac Arrhythmias in Intraoperative and Immediate Postoperative Periods (Brazil: 20 Programs, 19.8%; Spain: 5 Programs, 8.5%; The United Kingdom: 9 Programs, 9.4%; P =.045); and (F) Mastering the Basics of Conscious Sedation (Brazil: 19 Programs, 18.8%; Spain: 2 Programs, 3.4%; The United Kingdom: 9 Programs, 9.4%; P=.009). All Data Were Analyzed Using the Chi-Square Test. “Included” and “Not Included” Responses Were Compared.
The content concerning skills related to drug administration was also below expectations in the evaluated curricula. The contents “Administer intramuscular, subcutaneous, and intravenous injections” and “Mastering the technique of local anesthesia” were present in between 10.2% and 43.6% of the residency programs, as demonstrated in Figure 3C and D. As shown in Figure 3E and F, the competencies of “Mastering the treatment of the most prevalent cardiac arrhythmias in intraoperative and immediate postoperative periods” and “Mastering the basics of conscious sedation” seem to be the most underrepresented, since they were offered in only 3.4% and 19.8% of the curricula.
Analysis of Competencies Related to Sedation and Analgesia
The analysis of competencies related to sedation and analgesia revealed that they were consistently underrepresented across all three countries. As shown in Figure 4, <50.0% of all the competencies were taught in all the curricula: selecting the most appropriate intraoperative and postoperative analgesia (between 27.1% and 40.6%, Figure 4A); performing lumbar punctures and cerebrospinal fluid injections (between 10.4% and 16.9%, Figure 4B); conducting joint punctures and injections (between 8.3% and 13.6%, Figure 4C); mastering the technique of anesthetic blocks for fingers and toes, as well as other peripheral anesthetic blocks (between 5.9% and 10.2%, Figure 4D); mastering anesthetic techniques and their specific variants (between 1.1% and 2.9%, Figure 4E); and evaluating and administering anesthesia with a focus on the neuroaxis (between 0.9% and 3.4%, Figure 4F).

Sedation and Analgesia-Related Competencies Were Assessed in Residency Programs Across Brazil (n=101), Spain (n=59), and the United Kingdom (n=96), Totaling 256 Programs. The Y-Axis Represents the Percentage of Programs in Each Country That Include the Given Competency. The Competencies Analyzed Were: (A) Select the Best Intra- and Postoperative Analgesia (Brazil: 41 Programs, 40.6%; Spain: 16 Programs, 27.1%; The United Kingdom: 29 Programs, 30.2%; P =.148); (B) Perform Lumbar Puncture for Diagnostic or Therapeutic Purposes (Brazil: 15 Programs, 14.9%; Spain: 10 Programs, 16.9%; The United Kingdom: 10 Programs, 10.4%; P =.468); (C) Perform Joint Puncture and Injection (Brazil: 10 Programs, 9.9%; Spain: 8 Programs, 13.6%; The United Kingdom: 8 Programs, 8.3%; P = .575); (D) Mastering the Technique of Anesthetic Blocks for Fingers and Toes, as Well as Peripheral Anesthetic Blocks (Brazil: 6 Programs, 5.9%; Spain: 6 Programs, 10.2%; The United Kingdom: 6 Programs, 6.3%; P=.559); (E) Mastering Anesthetic Techniques and Their Specific Variants (Brazil: 3 Programs, 2.9%; Spain: 1 Program, 1.7%; The United Kingdom: 1 Program, 1.1%; P =.612); and (F) Evaluate and Perform Neuraxial Approaches to the Subarachnoid or Epidural Space for Diagnosis, Treatment, or Anesthesia (Brazil: 1 Program, 0.9%; Spain: 2 Programs, 3.4%; The United Kingdom: 2 Programs, 2.1%; P=.567). All Data Were Analyzed Using the Chi-Square Test. “Included” and “Not Included” Responses Were Compared.
Analysis of Competencies Related to Intensive Care
Regarding intensive care skills, we observed that these competencies were poorly represented in the curricular frameworks of residency programs across the three evaluated countries. Among these competencies are the installation and interpretation of basic monitoring systems performing necessary interventions to maintain the patient's clinical stability (between 40.7% and 55.5%, Figure 5A); analyzing and preventing surgical infections (between 32.2% and 41.6%, Figure 5B); identifying and treating clinical complications during the intraoperative and postoperative periods (between 25.4% and 38.6%, Figure 5C); identifying and managing bleeding and other anesthetic complications in the postanesthesia recovery room (between 22.1% and 34.7%, Figure 5D); interpreting vascular anatomy and performing both peripheral and central venous catheterization (between 23.9% and 38.6%, Figure 5E); diagnosing, evaluating, and treating various types of shock (between 19.8% and 25.4%, Figure 5F); and using external pacemakers and external paddle defibrillation to address unwanted arrhythmias during surgery and performing cardiopulmonary resuscitation (between 5.1% and 15.8%, Figure 5G).
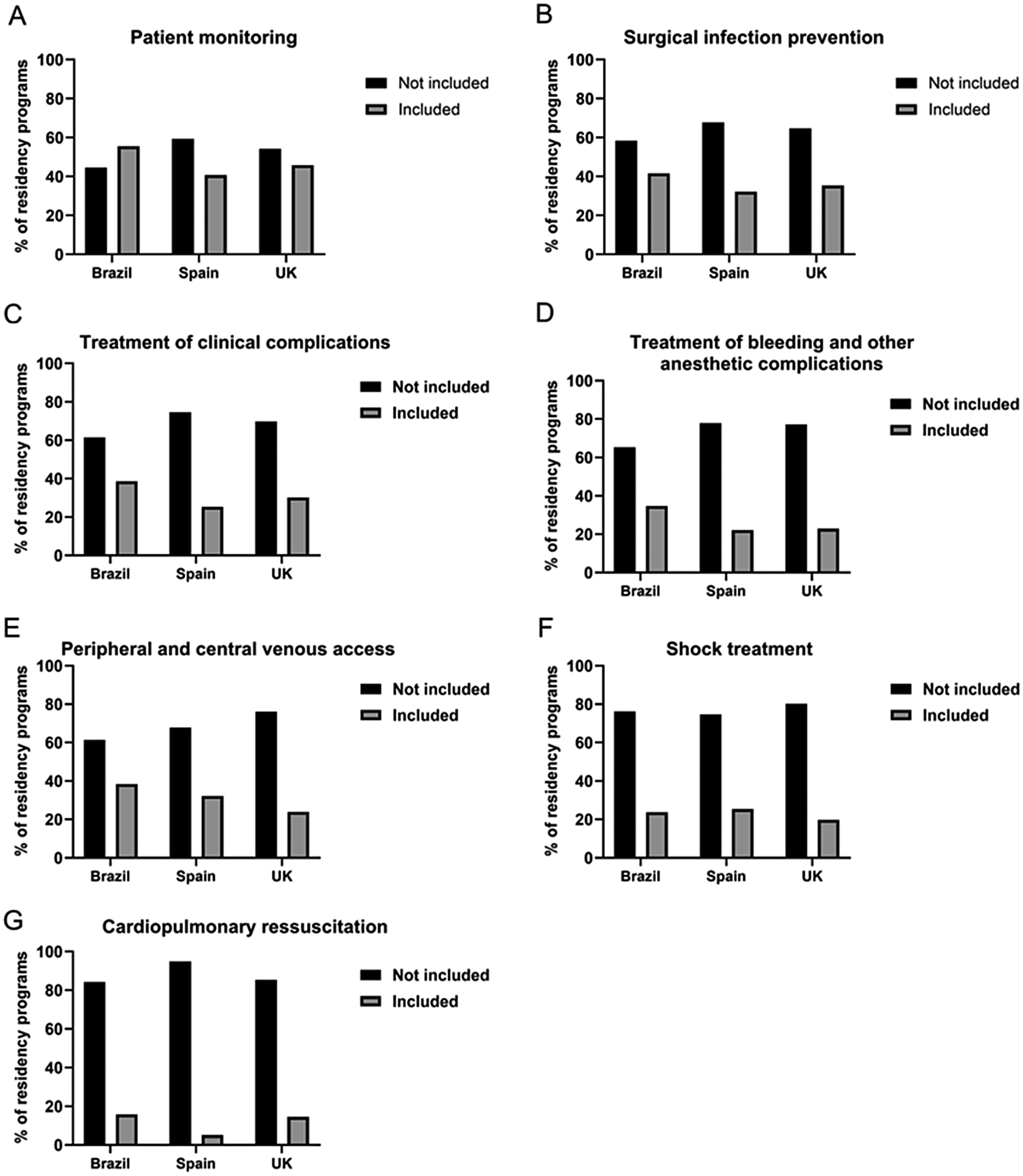
Intensive Care-Related Competencies Were Assessed in Residency Programs Across Brazil (n=101), Spain (n=59), and the United Kingdom (n=96), Totaling 256 Programs. The Y-Axis Represents the Percentage of Programs in Each Country That Include the Given Competency. The Competencies Analyzed Were: (A) Install and Interpret Basic Monitoring as Well as Perform What Is Necessary to Maintain the Patient's Clinical Balance (Brazil: 56 Programs, 55.5%; Spain: 24 Programs, 40.7%; The United Kingdom: 44 Programs, 45.8%; P =.160); (B) Analyze the Causes of Surgical Infection and Prevent Them (Brazil: 42 Programs, 41.6%; Spain: 19 Programs, 32.2%; The United Kingdom: 34 Programs, 35.4%; P=.451); (C) Identify and Treat Clinical Complications During Intra- and Postoperative Periods (Brazil: 39 Programs, 38.6%; Spain: 15 Programs, 25.4%; The United Kingdom: 29 Programs, 30.2%; P=.192); (D) Identify and Treat the Causes of Bleeding and Other Intra- and Postoperative Anesthetic Complications (Postanesthesia Recovery Room) (Brazil: 35 Programs, 34.7%; Spain: 13 Programs, 22.1%; The United Kingdom: 22 Programs, 22.9%; P=.105); (E) Interpret Vascular Anatomy and Perform Peripheral and Central Venous Catheterization (Peripheral and Central) (Brazil: 39 Programs, 38.6%; Spain: 19 Programs, 32.2%; The United Kingdom: 23 Programs, 23.9%; P =.086); (F) Diagnose, Assess, and Treat Several Types of Shock (Brazil: 24 Programs, 23.8%; Spain: 15 Programs, 25.4%; The United Kingdom: 19 Programs, 19.8%; P =.678); and (G) Use an External Pacemaker and Paddle Defibrillation to Treat Unwanted Arrhythmias During Surgery and Perform Cardiopulmonary Resuscitation (Brazil: 16 Programs, 15.8%; Spain: 3 Programs, 5.1%; The United Kingdom: 14 Programs, 14.6%; P =.121). All Data Were Analyzed Using the Chi-Square Test. “Included” and “Not Included” Responses Were Compared.
Analysis of Competencies Related to Airway Management
With respect to skills related to airway management, which is important for patients with COVID-19, similar to other skills, the teaching of these skills was also a minority of residency programs in the three countries evaluated. The competencies investigated were identifying, assessing, and treating respiratory insufficiency (between 22.9% and 35.6%, Figure 6A); evaluating and performing tracheal intubation and extubation (between 13.5% and 20.7%, Figure 6B); recognizing and interpreting difficult airway assessments and managing them safely according to endorsed protocols (between 8.5% and 11.9%, Figure 6C); and analyzing various forms of ventilation (between 11.4% and 16.9%, Figure 6D).

Airway Management-Related Competencies Were Assessed in Residency Programs Across Brazil (n=101), Spain (n=59), and the United Kingdom (n=96), Totaling 256 Programs. The Y-Axis Represents the Percentage of Programs in Each Country That Include the Given Competency. The Competencies Analyzed Were: (A) Identify, Assess, and Treat Respiratory Insufficiency (Brazil: 36 Programs, 35.7%; Spain: 19 Programs, 32.2%; The United Kingdom: 22 Programs, 22.9%; P =.138); (B) Evaluate and Perform Tracheal Intubation and Extubation (Brazil: 21 Programs, 20.8%; Spain: 12 Programs, 20.3%; The United Kingdom: 13 Programs, 13.5%; P=.359); (C) Recognize and Interpret the Assessment of a Difficult Airway and Handle It Safely, Following Endorsed Protocols (Brazil: 12 Programs, 11.9%; Spain: 5 Programs, 8.5%; The United Kingdom: 10 Programs, 10.4%; P =.794); and (D) Analyze Various Forms of Ventilation (Brazil: 13 Programs, 12.9%; Spain: 10 Programs, 16.9%; The United Kingdom: 11 Programs, 11.4%; P =.612). All Data Were Analyzed Using the Chi-Square Test. “Included” and “Not Included” Responses Were Compared.
Analysis of the Distribution of Anesthesiology Competencies in Medical Residency Programs in Brazil, Spain, and the UK
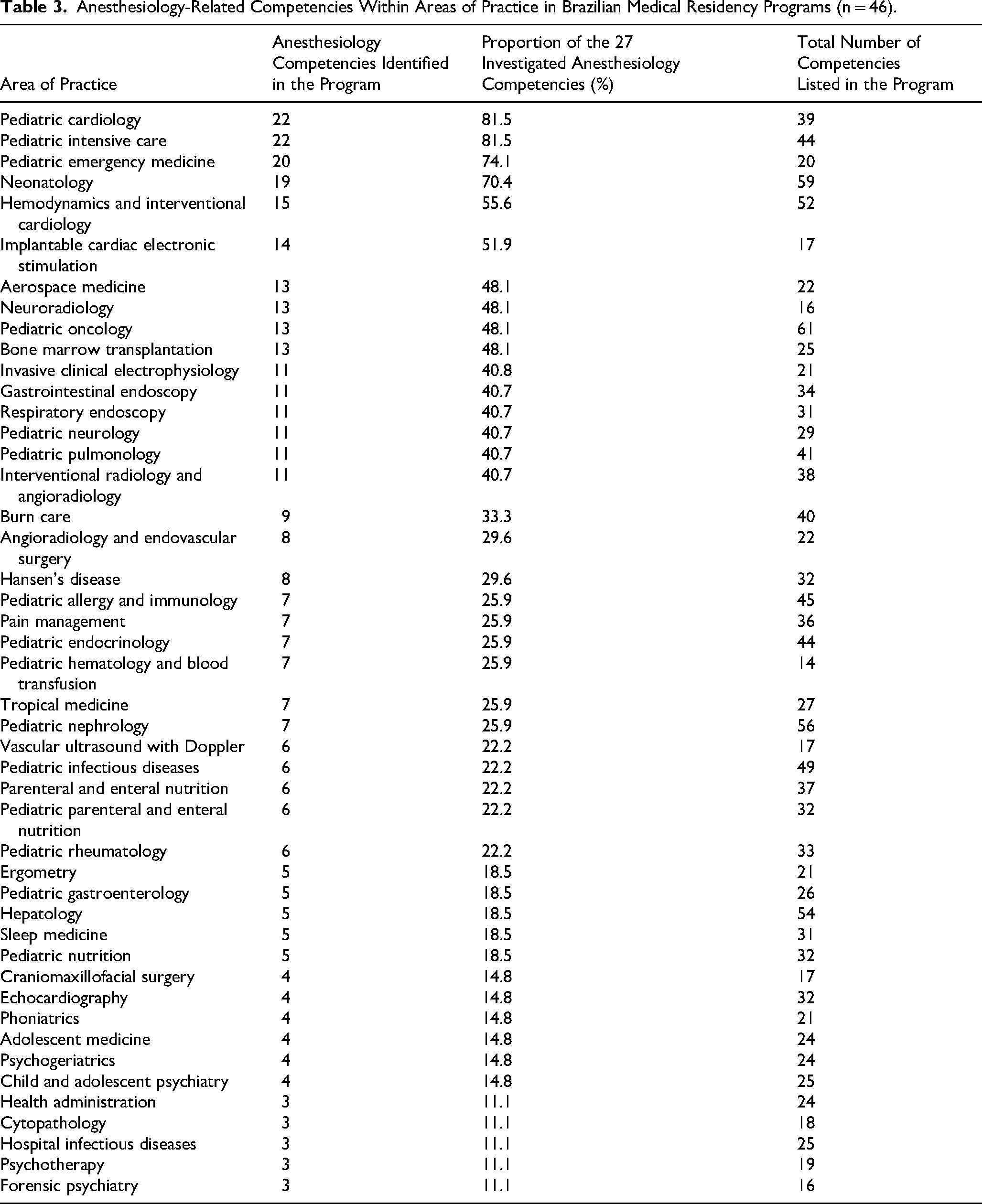
Finally, we investigated the extent to which these 27 assessed competencies were specific to the anesthesia residency or included in other residency programs. In Brazil, curricular matrices are currently available for 46 areas of medical practice, each encompassing between 11 and 244 learned competencies, as well as 55 specialty programs, which include between 7 and 332 learned competencies. Overall, only 6 medical practice programs and 16 specialty programs teach more than 14 anesthesiology competencies, which is half (50%) of the competencies investigated in this study (Tables 3 and 4). Spain presented 7 specialization programs (total of 59 programs) presenting more than 14 skills in anesthesiology, despite being the country with the highest number of skills taught (minimum of 17 and maximum of 736 skills) (Table 5). The UK also had a low number of programs teaching more than 14 anesthesiology competencies. In terms of practice, only 5 out of 31 programs included this amount of knowledge (Table 6). Among the specialties, only 7 out of 65 programs had these competencies (Table 7). The number of skills learned in the UK ranged from 11 to 44, depending on the program. Notably, the programs that shared the most anesthesiology competencies were those in Emergency Medicine, Intensive Care, Surgery, and Pediatrics.
Anesthesiology-Related Competencies Within Areas of Practice in Brazilian Medical Residency Programs (n = 46).
Anesthesiology-Related Competencies Within Medical Specialties in Brazilian Residency Programs (n = 55).

Anesthesiology-Related Competencies Within Medical Specialties in Spanish Residency Programs (n = 59).

Anesthesiology-Related Competencies Within Areas of Practice in the UK Residency Programs (n = 31).

Anesthesiology-Related Competencies within Medical Specialties in the Uk Residency Programs (n = 65).

Discussion
According to Prideaux's educational perspective (2003), a curriculum can be conceptualized as a set of activities that encompass a study program or course plan, including essential elements such as content, teaching and learning strategies, and assessment processes. 18 It can be classified as descriptive or prescriptive. The prescriptive curriculum is defined by specific objectives or outcomes for students, while in the descriptive curriculum, there is a comprehensive and systematic analysis of the educational context to understand its impact on curriculum development. 18 In this context, the analysis of the curriculum frameworks of medical residency programs in Brazil, Spain, and the UK evaluated in this work considered the textual identification of anesthesiology competencies regardless of the classification of these frameworks as descriptive or prescriptive.
Through this perspective, we examined the curriculum frameworks of medical residency programs provided by the respective regulatory bodies of 49 medical specialty programs and 46 areas of practice in Brazil, 65 specialty programs and 31 areas of practice in the UK, and 59 specialties in Spain. At the time of this research, Spanish programs and specialties did not include descriptions of areas of practice or subspecialties. We observed that the curricula feature both specific and general competencies, with the latter being common to all specialties.
Competencies considered general to all specialties— such as medical ethics, scientific article production, multidisciplinary teamwork, and knowledge of the anatomy, physiology, and pharmacology of various organs and systems—are present in most medical residency programs in Brazil, Spain, and all programs across the UK, with statistically significant differences. The omissions found in some programs in Brazil and Spain likely reflect gaps in the development or documentation process rather than intentional exclusions. Despite these gaps in the curricular framework, professionals by the end of their training are expected to demonstrate the ability to complete their final project, collaborate effectively in multiprofessional teams, and possess an understanding of human anatomy and physiology. The curriculum structure in the UK, however, may account for the stronger alignment of its programs with these competencies.
With respect to specific competencies, we observed a significant underrepresentation across all the evaluated curricula. Some of these competencies include anesthetic-surgical risk stratification (P < .027); recognizing and adequately analyzing palliative care (P < .023); administering intramuscular, subcutaneous, and intravenous injections (P < .007); mastering the technique of local anesthesia (P < .001); managing the most prevalent cardiac arrhythmias in the intraoperative and immediate postoperative periods (P < .045); and mastering the fundamentals of conscious sedation (P < .009). The UK curricula presented a lower number of all these competencies. A reduced number of competencies across all countries’ residency programs are also observed in areas such as sedation, pain management, intensive care, cardiopulmonary resuscitation, and airway management, with no statistically significant differences among the countries.
These curricular gaps may impact both the safety of clinical practice and the quality of research. In clinical practice, they could lead to increased complications and mortality due to the inappropriate use of analgesic, sedative, and muscle relaxant drugs as well as improper handling of medical equipment. 19 Competence in these areas is essential for mastering the skills that form part of safety protocols, which are already the subject of artificial intelligence research aimed at supporting educational contexts. 20 From a scientific perspective, researchers require adequate knowledge to develop ethical, effective, and complication-free anesthetic protocols, particularly in experimental studies involving animal models, as inadequate protocols may introduce bias and compromise the reliability of research outcomes. 21
With respect to residency programs, the research results indicate that anesthesiology curricula across the three studied countries presented similar descriptions of core competencies. However, anesthesiology-related competencies were also prevalent in other programs that deal with potentially critical patients or that serve large population groups, such as family and community medicine. This indispensable curricular coherence can be illustrated by the path of a patient diagnosed with hip osteoarthritis in primary care, who, after undergoing surgery, will recover in an intensive care unit and, after hospital discharge, may return to primary care for the management of comorbidities. This demonstrates the need for integration and continuity of care across the different levels of healthcare.
In addition to the change in disease profile—where degenerative diseases now require high-complexity procedures that cause more deaths than infectious diseases 7 —new health crises have emerged. The COVID-19 pandemic and the opioid crisis, among other, have become severe health issues, continuing to demand significant mobilization of health institutions. The medical emergency caused by the COVID-19 pandemic highlighted the need for specialized knowledge to monitor patients with respiratory failure, providing ventilatory support, venous hydration, the administration of vasoactive drugs, and sedation to allow invasive ventilation.3,5 In this context, the severity of many cases was identified at the primary care level, reinforcing the importance of adequately training professionals who work in these care settings. On the other hand, the opioid dependency crisis, which emerged in the United States with fentanyl and in parts of Africa, Asia, and the Middle East with tramadol, also underscores the urgent need for education in pain management, whether acute or chronic. 22
In Brazil, the specialties with the greatest number of competencies in medical residency programs are Emergency Medicine, Intensive Care, Cardiovascular Surgery, and Family and Community Medicine, whereas Pediatric Cardiology and Neonatology stand out in specific areas of practice. In Spain, the most comprehensive specialties are Intensive Medicine, Neurosurgery, Family and Community Medicine, and Pediatric Nursing. In the UK, the specialties include Emergency Medicine, Cardiovascular Surgery, Intensive Care, and Acute Internal Medicine, with Pediatric Emergency Medicine, Pediatric Intensive Care, and Neonatal Medicine being notable areas of practice.
Although some specialties with a reduced total number of competencies present a high proportion of anesthesiology-related competencies, this proportional representation does not necessarily indicate in-depth training in the field. Programs such as Traffic Medicine or Pediatric Emergency Medicine, for instance, feature compact curricular frameworks and yet include more than 60% of the analyzed anesthesiology-related competencies. However, this high percentage may reflect a more superficial approach or a focus on specific clinical contexts. Therefore, interpreting the presence of anesthesiology competencies requires not only quantitative analysis but also attention to the depth and complexity with which these skills are addressed, since learning outcomes depend on content, motivation, and the educational context. 23
The high number of anesthesiology-related competencies in specialties such as Hand Surgery, Interventional Radiology, or Aerospace Medicine may be explained by the overlap of clinical skills shared with anesthetic practice, particularly those involved in perioperative care—such as clinical evaluation, infection prevention measures, bleeding control, respiratory and hemodynamic stabilization, and pain management. Although these competencies are directly associated with anesthesiology, they are also integral to the routine clinical practice of these specialties. This suggests that the observed emphasis on anesthesiology-related competencies may reflect the cross-cutting nature of these clinical skills, rather than a deliberate or structured anesthesiology training pathway.
In programs with extensive curricular loads and short durations—such as Family and Community Medicine in Brazil—a significant number of anesthesiology-related competencies (77.8%) are included. Nevertheless, these are embedded within a total of 332 competencies over just 2 years, 24 which poses a substantial challenge to the effective acquisition and development of competencies. In contrast, equivalent programs in Spain, such as Family and Community Medicine, include an even larger set of competencies (467), but with a longer training period of 4 years, 25 potentially allowing for more robust consolidation of clinical skills. This contrast underscores the importance of considering both curricular density and program duration when evaluating the effective acquisition of competencies, including those related to anesthesiology.
Despite the similar prevalence of competencies in program curricula, other nonpedagogical factors must be considered, as they influence both educational outcomes and population health. Socioeconomically, Brazil shows the poorest health indicators among the countries analyzed. The average life expectancy among Organization for Economic Cooperation and Development (OECD) countries is 80.3 years; in Spain, it is 83.3 years; in the UK, it is 80.4 years, whereas in Brazil, it is 74.3 years. In terms of physicians per capita, OECD data indicate that Brazil has an average of 11.75 doctors per 100,000 inhabitants, compared with 13.93 in Spain and 13.12 in the UK. 26 The OECD average is 13.50 doctors per 100,000 inhabitants. 15 In the field of medical education, the UK has 16 medical schools among the top 100 in the world, whereas Brazil and Spain each have only one.27,28 Despite the better performance of medical schools in the UK, Spain has superior health indicators, including in the fight against COVID-19, according to the World Health Organization (WHO) and the Worldometer.29,30
Although the analysis was conducted independently by 2 researchers, who cross-checked and reviewed the data to identify potential inconsistencies after completing their respective analyses, a weakness of this study lies in its methodological approach. Specifically, the curricular matrix sourced from the internet may be outdated or lack essential information. Additionally, the analysis of 256 documents in 3 different languages posed challenges due to the lack of uniformity in terms of formatting and organization. Nevertheless, the identified gap in competencies highlights the need for further reflection on the development of curricula that can be compared across countries and international institutions.
Conclusions
In this study, the anesthesiology medical residency programs in Brazil, Spain, and the UK presented similarities in terms of the number of competencies. The programs in other specialties and areas of practice that have the highest number of anesthesiology competencies are those related to the treatment of critically ill patients. The low prevalence of competencies related to pain management, sedation, airway management, and hemodynamic monitoring, which are essential for high-complexity procedures, suggests a need for curriculum revision in medical residency programs and a potential increase in the number of slots for specialty programs focused on caring for critically ill patients.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251358060 - Supplemental material for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom
Supplemental material, sj-docx-1-mde-10.1177_23821205251358060 for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom by Dayse dos Santos de Almeida Rodrigues, Alexia de Almeida Reis Rodrigues, Natiele Carla da Silva Ferreira and Luiz Anastácio Alves in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251358060 - Supplemental material for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom
Supplemental material, sj-docx-2-mde-10.1177_23821205251358060 for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom by Dayse dos Santos de Almeida Rodrigues, Alexia de Almeida Reis Rodrigues, Natiele Carla da Silva Ferreira and Luiz Anastácio Alves in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251358060 - Supplemental material for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom
Supplemental material, sj-docx-3-mde-10.1177_23821205251358060 for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom by Dayse dos Santos de Almeida Rodrigues, Alexia de Almeida Reis Rodrigues, Natiele Carla da Silva Ferreira and Luiz Anastácio Alves in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251358060 - Supplemental material for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom
Supplemental material, sj-docx-4-mde-10.1177_23821205251358060 for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom by Dayse dos Santos de Almeida Rodrigues, Alexia de Almeida Reis Rodrigues, Natiele Carla da Silva Ferreira and Luiz Anastácio Alves in Journal of Medical Education and Curricular Development
Supplemental Material
sj-xlsx-5-mde-10.1177_23821205251358060 - Supplemental material for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom
Supplemental material, sj-xlsx-5-mde-10.1177_23821205251358060 for Preparing for Practice: A Comparative Analysis of Anesthesiology Residency Competencies in Brazil, Spain, and the United Kingdom by Dayse dos Santos de Almeida Rodrigues, Alexia de Almeida Reis Rodrigues, Natiele Carla da Silva Ferreira and Luiz Anastácio Alves in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We thank the Teaching and Biosciences Program at the Oswaldo Cruz Institute for their support in the development of this work.
ORCID iDs
Author Contributions
DSAR conceived the study, designed the methodology, provided resources, conducted the investigation and formal analysis, managed the data, produced the data presentation, and wrote the original draft. AARR conducted the investigation, managed the data, produced the data presentation, and wrote the original draft. NCSF conducted the formal analysis, prepared the figures, and wrote the original draft. LAA conceived and supervised the study, managed the project, designed the methodology, provided resources, and reviewed and edited the manuscript. All the authors have approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.