
Abstract
Background
Neonatal mortality remains a significant public health concern in Tanzania, with birth asphyxia being one of the leading causes. The Helping Babies Breathe program aims to equip providers with essential neonatal resuscitation skills, particularly in resource-limited settings.
Objective
To assess and document the effectiveness of a peer-led training program on knowledge and confidence in neonatal resuscitation.
Methods
Helping Babies Breathe-Kairuki University (HBB-KU) initiative; a student-led program including both theoretical and practical components attended by future and current healthcare professionals (HCPs). Pre- and post-training knowledge tests assessing knowledge and understanding, and self-evaluation tests reporting self-confidence were administered.
Results
Test results of participants from 2016 to 2023 were analyzed using the paired t-test. HBB-KU initiative successfully trained 1389 trainees. A total of 1243 (93.11%) included medical, nursing, and other health-allied science students. Pre (10.63 ± 2.53) and post (14.71 ± 1.60) training knowledge test scores demonstrated statistically significant (P < .01) improvements. Confidence prior to training, 213 (15.97%) participants reported feeling “very confident”; however, following training, an increase was noted, reaching 784 (58.72%) participants feeling “very confident,” demonstrating a difference of 42.75%.
Conclusion
The results indicate HBB-KU peer-led training initiative is effective in mitigating knowledge gaps and developing confidence around neonatal resuscitation among participants. Given the resource-limited setting, this accomplishment provides a context for a replicable model where students can teach and train peers, and practicing HCPs may be an efficient method to expand neonatal care in similar circumstances, globally.
Introduction
According to the United Nations International Children's Emergency Fund (UNICEF) Child Mortality Report in 2022, the first 28 days of life continue to be the most precarious for a child's survival. Approximately 2.3 million neonatal deaths occur during the first month of life annually, with the largest regional contribution from Sub-Saharan Africa (SSA). 1 The average global neonatal mortality rate (NMR) is 18 deaths per 1000 live births. In the SSA region, the NMR is 27 deaths per 1000 live births.1,2 The data translated show that a neonate is 11 times more likely to die in SSA compared to regions with low NMR, such as Australia and New Zealand. 1
A moderate decline is noted on the under-five mortality rate in Tanzania; however, a hovering plateau is noted for the last decade in NMR, from 40 deaths per 1000 live births in 1999 to 26 deaths per 1000 live births in 2010 and 24 deaths per 1000 live births in 2022.2–6 The most common causes of neonatal mortality in Tanzania are largely contributed by birth asphyxia followed by sepsis, respiratory distress, and complications of prematurity. The alarming plateau of the NMR over the past decade compared to the under-five mortality rate in Tanzania demands innovative and targeted initiatives to counter mortality during this vulnerable neonatal period.7–9
Birth asphyxia remains one of the highest contributors to global neonatal mortality and highlights the need to focus foremost on preventing and treating this condition, which is defined as the failure to initiate and sustain breathing at birth.1,10 In 2010, the American Academy of Pediatrics (AAP) created the “Helping Babies Breathe (HBB)” program, a neonatal resuscitation training tailored to cater specifically meet the needs of resource-limited environments, including Tanzania. 11 The HBB program addresses the urgent need to equip healthcare professionals (HCPs) with skills to immediately respond to birth asphyxia.12–14
It has been identified that low-middle income countries (LMICs) require urgent, affordable neonatal resuscitation training to combat early neonatal mortality within seven days post-delivery. 7 Clinical students at Kairuki University (KU) frequently observed and occasionally participated in neonatal resuscitation techniques under the direct supervision of licensed HCPs during their clinical rotations. Numerous students reported insufficient knowledge and practical skills for basic neonatal resuscitation protocols post-delivery and in the neonatal intensive care units (NICUs). Therefore, a need for more focused training methods on responding to emergent situations was identified with the students at KU, eventually leading to the establishment of the Helping Babies Breathe-Kairuki University (HBB-KU) Alliance. Much of the previous work involving the implementation of the HBB program in Tanzania has focused on training practicing HCPs. Considering the limitations of the educator-to-student ratio, opting for a peer-to-peer led program was feasible to conduct scalable, frequent training sessions, and the opportunity to reinforce knowledge through peer mentoring.
To our knowledge, no previous research demonstrates that HBB skills can be effectively peer-taught at the university level by students themselves, creating future cohorts of HCPs effectively trained in neonatal resuscitation. This retrospective study aimed to determine the effectiveness of a peer-led HBB training program in improving knowledge and self-reported confidence in neonatal resuscitation among medical and nursing students at KU, with sessions delivered by senior clinical students trained as peer facilitators. The study aims to further explore the potential of peer-led programs, particularly in aspects of neonatal care within resource-limited settings such as Tanzania.
Methodology
Study Design
This study utilized a retrospective pre-post design to evaluate the effectiveness of the HBB-KU training program from November 2016 to November 2023. Data were collected prospectively during each training session and compiled into a database for retrospective analysis. The reporting of this study conforms to the STROBE-Sim guideline for simulation-based healthcare research 11 (Supplemental Material 1).
HBB-KU Initiative
Established in 2016, the creation of the HBB-KU Alliance was driven by the commitment of the HCPs students at KU. A pivotal phase in this initiative was the training of the first cohort of master trainers. Over the course of three days, the first master trainer cohort participated in an extensive training course, which placed equal emphasis on theoretical understanding and practical application of the HBB program.
Master trainers were selected from among senior medical and nursing students who had previously completed the HBB training with distinction and demonstrated strong communication and leadership skills. They were supervised and mentored by faculty members from the Department of Pediatrics and Child Health. In addition to their technical proficiency, master trainers serve as mentors, guiding their peers through simulation scenarios and role-playing exercises to strengthen practical comprehension.
Master training classes were typically composed of 10 to 15 participants to allow sufficient instructor-to-trainee interaction. Sessions included both group discussions and hands-on simulation, using hardcopy training materials from the HBB Second Edition Training Guide. The full course was delivered over two days, with ∼6 to 8 h of instruction and practice per day.
Their participation also includes logistical preparation, where they actively participate in resource management and ensure effective use of training materials and equipment. The escalation of the training sessions within the HBB-KU initiative was coordinated by the master trainers. The subsequent training of upcoming master trainers guaranteed the sustainability of the initiative. Beyond the training room, the master trainers closely worked with the Paediatric and Child Health Department at KU, which generously supported the HBB-KU initiative to its success.
Setting
KU is a healthcare university located in Dar-es-Salaam, Tanzania, enrolling ∼1500 students annually in an array of programs, including postgraduate and undergraduate degrees such as Doctor of Medicine, Bachelor of Science in Nursing, and Bachelor of Social Work. Undergraduate medical students across 5 years of training represent ∼70% of the student population, with an average of 120 medical graduates annually.
Participants
Trainees included students and professionals in the healthcare sector. The students were enrolled in medical, nursing, social work, and other health and allied science training programs at KU, Muhimbili University of Health and Allied Sciences, and other regional medical schools. At KU, before beginning the pediatric clinical rotations in year three for nursing students and in year four for medical students, each student is recommended to complete the HBB training. Additionally, the trainings have extended the reach to collaborate with healthcare facilities, including Kairuki Hospital and Shree Hindu Mandal Hospital, training the current HCPs: doctors, nurses, midwives, and specialists, including obstetrics and gynecologists, pediatricians, surgeons, and anesthesiologists.
Training and Data Collection
The HBB-KU initiative adopts the HBB Second Edition Training Guide from AAP available on the official website for free use. 12 The same standardized training materials and assessment tools were used for all student cadres, including medical, nursing, and allied health students, to ensure uniformity and comparability across groups. It is a dual approach to training that includes both theoretical and practical elements. Training modules include getting prepared for delivery, essential equipment for assisting newborn breathing, routine care, the essence of the “golden minute” following birth, ventilation techniques, and monitoring. The theoretical element of the training is designed to provide trainees with a thorough knowledge of the physiology and the imperative need for neonatal resuscitation. The practical element of the training is a comprehensive and thorough experience designed to convert theoretical knowledge into practical abilities. It includes practical demonstrations, simulations, and role-playing exercises of routine care, neonatal stimulation methods, suction techniques, and the correct use of a bag and mask during resuscitation. The focus of incorporating a practical element in the training is to build skills and provide an opportunity for the trainees to gain the confidence to react appropriately in high-pressure situations.
Demographic data of the trainees were collected during registration for the HBB training program. Preceding the formal training, trainees complete a knowledge test to obtain a baseline understanding of neonatal resuscitation concepts. The knowledge test consists of 18 carefully constructed questions covering a wide range of topics included in the HBB program curriculum and is timed with 30 s allotted for each question. Following the training, the participants complete the post-training knowledge survey. The same 18-item questionnaire was used for pre-intervention and post-intervention and was sourced from the HBB Second Edition knowledge check questionnaire released by the Helping Babies Survive Program. Satisfactory results of above 70% in the post-training knowledge survey certify the trainee as HBB-trained. Students completed the pre- and post-training surveys using a multiple-choice answer sheet.
To obtain trainees' self-perceived confidence in neonatal resuscitation, self-evaluation forms were administered prior to and post-completion of the HBB training program. Questions included self-rate prompts in their confidence in neonatal resuscitation pre- and post-intervention.
Sample Size
We used the Kish-Lisle formula below to calculate the minimum sample size needed for our study:

Ten percent of the calculated value was added to account for non-respondence or withdrawal from the study after enrollment.
A minimum of 384 study respondents are required for the study, including a 10% non-response, for a total of 422 respondents. The 50% probability of the HBB-KU training respondents was selected as a conservative measure to account for potential variability from participants. This likelihood takes into account a thorough representation of the target population.
Data Analysis
Data were managed through Microsoft Excel, and analysis was performed using STATA software version 20. All data collected were de-identified and given a serial number before entry in Microsoft Excel, and later transferred to STATA for analysis. Paired t-tests were conducted to compare pre- and post-knowledge survey scores. Since both pre- and post-training knowledge test scores were collected from the same participants, a paired t-test was applied to compare within-subject improvements. Group means reported in Table 2 represent the average of individual paired scores. A P-value of less than or equal to P < .01 was considered statistically significant. Self-confidence shifts before and after training were also analyzed, and additional chi-square tests were performed to assess the statistical significance of categorical shifts.
Ethical Approval and Informed Consent
The HBB-KU Alliance is fundamentally an educational initiative spearheaded by the Department of Pediatrics and Child Health at KU. Given the educational nature of the program and its classification as a low-risk activity, formal ethical approval was deemed not required. However, to uphold ethical standards, verbal consent was obtained from all participants, ensuring their informed cooperation in the evaluation processes used for research purposes.
The confidentiality of the trainee's test scores was ensured using codes instead of the trainee's names. All participants received comprehensive details regarding the training sessions’ objectives, methodology, and potential benefits of the training sessions. Participants were assured that their participation was voluntary and that they could withdraw from the training at any time without any repercussions.
Results
The HBB-KU trained a total of 1389 participants from November 2016 to November 2023, of which 1335 (96.11%) participants’ data were completed. The majority of the participants were students, with 1243 (93.11%), which included medical students, nursing students (bachelor's degree and diploma), and other health and allied science students. The remaining 92 (6.89%) were HCPs, which included medical doctors, registered nurses, midwives, and specialists such as critical care nurses, pediatricians, obstetricians, gynecologists, and surgeons.
As shown in Table 1, 964 participants (72.21%) reported never having participated in a neonatal resuscitation prior to the HBB training without having previously completed an HBB course. Similarly, 936 participants (70.11%) had not previously attended any formal HBB training. Prior to HBB training, a total of 721 (54.00%) of the study participants reported they had no confidence in their ability to perform neonatal resuscitation, while 213 (15.97%) were very confident in their skills. A Chi-square test revealed a statistically significant shift in confidence levels pre- and post-training (χ² = 890.36, df = 2, P < .00001), confirming that the HBB-KU program was associated with a substantial increase in self-reported confidence in assisting neonatal resuscitation (Figure 1 and Table 1).

Change in self-reported confidence in neonatal resuscitation before and after Helping Babies Breathe (HBB) training among participants (N = 1335).
Characteristics of Study Participants.
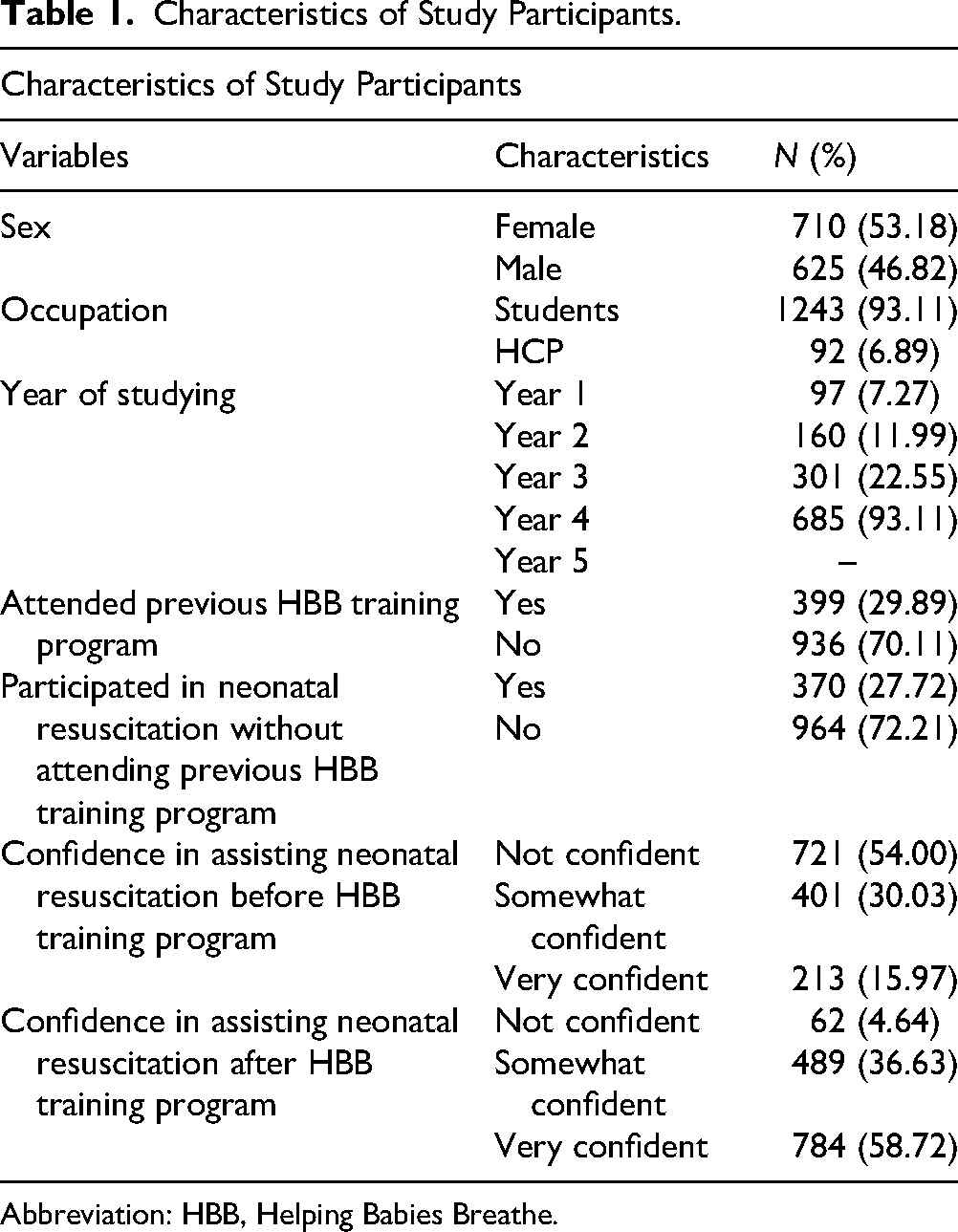
Abbreviation: HBB, Helping Babies Breathe.
Pre- and Post-Training Knowledge Scores Among Study Participants who Completed the HBB Training (Maximum Score = 18).

Abbreviation: HBB, Helping Babies Breathe; HCPs: healthcare professionals.
Paired t-tests were used to compare the mean knowledge scores before and after the training.
Current HCPs refer to HCPs already practicing in the field, while future HCPs include students in the field.
Table 2 displays the results of paired t-tests comparing pre- and post-training knowledge scores for each participant subgroup. Although summarized as group means, the analysis was performed on individual-level paired data. These results indicate all participants and the sub-groups within the participants had statistically significant improvement (P < .01) (Table 2).
Discussion
The HBB-KU alliance represents an important first step initiated by future HCPs in tackling Tanzania's pervasive problem of high NM. The primary objective of this study was to evaluate the impact of peer-led methodology on improving and enhancing the neonatal resuscitation knowledge and skills of medical and nursing students. The study undoubtedly demonstrated the remarkable success of the HBB-KU training of 1389 trainees in a span of 7 years from 2016 to 2023.
Numerous studies have demonstrated the effectiveness of HBB training implementation with significant improvements in knowledge gaps and other tested skills.7–9,15 The HBB program's efficacy in filling the knowledge gap in neonatal resuscitation is also evident in this study by the significant increase in the post-training knowledge survey scores compared to pre-training knowledge survey scores across different participant subgroups (Table 2). Additionally, the study participants reported a considerable increase in confidence following the HBB training, which may translate to an increased willingness to appropriately respond to newborn emergencies in clinical settings.16,17 However, it is important to acknowledge that self-reported confidence does not necessarily reflect practical competence. The study did not include an objective assessment of clinical skills, such as through an Objective Structured Clinical Examination (OSCE) or evaluation of bag-mask ventilation technique. These forms of assessment could provide a more accurate and standardized measure of neonatal resuscitation proficiency.
Despite this, previous studies in Tanzania and abroad have revealed that there is a positive correlation between the HBB training and a decrease in neonatal mortality rates due to birth asphyxia.7,9,13,18 It was concluded that using HBB training has significantly improved prompt start of bag-valve-mask ventilation, particularly within the golden minute. 19 This further establishes the importance of conducting HBB training, particularly in LMICs where birth asphyxia contributes a large percentage of early NM. However, it cannot be ascertained that HBB training implementation improved management of asphyxiated newborns. It is important to clarify that HBB is designed to prevent progression to severe asphyxia by enabling immediate intervention in non-breathing infants. The training does not target the comprehensive management of infants who experience prolonged hypoxia or secondary cardiorespiratory failure.
With respect to the HBB-KU initiative, integration of a peer-led methodology has been shown to be vital. Peers foster a conversational and collaborative learning atmosphere, often comfortable to share clinical experience, which allows a platform to harbor shared learning. The communal approach of HBB-KU removes barriers of conventional hierarchy, which may obstruct effective engagement, open dialogue, and effective skills enhancement. The peer-led methodology serves as a means for trainees to witness skills required for effective neonatal resuscitation under the supervision of master trainers who have completed the training successfully themselves. To ensure that high standards were maintained, the peer-facilitated training sessions were conducted under the guidance and periodic supervision of faculty members from the Department of Pediatrics and Child Health, who reviewed session content, provided feedback, and ensured alignment with the HBB curriculum.
In resource-limited settings, peer-led programs could show particular effectiveness in addressing the barrier of disseminating practical healthcare skills. Conventional training approaches frequently encounter issues with scalability, cost, and accessibility. On the contrary, peer-led projects make use of local community connections, disseminating practical skills in a more scalable and financially affordable manner. 20 Peer-led trainings could also ensure that training is customized to the specifics of the local healthcare system, as they are better aware of the unique needs and circumstances of that particular setting.
The rooted peer-led methodology of the HBB-KU initiative has demonstrated significant effectiveness in showing how a collaborative learning environment has enhanced HCP trainees’ confidence and skill acquisition. By using peer-led methodology leverages and facilitates peer-to-peer interaction, which eliminates the traditional hierarchies that can hinder open dialogues and interactions. Dissemination of healthcare skills using peer-led methodology is noteworthy. However, peer-led methodology is not used in the medical fraternity, underscoring the opportunity for broader adoption and implementation in medical training programs globally. 21 Promoting and encouraging peer-led methodologies has the potential to transform training methods, particularly in environments where it is not feasible for specialists to conduct traditional educational paradigms.
While this study aimed to evaluate the effectiveness of the HBB-KU Alliance training, some limitations must be acknowledged. The primary data sources included pre- and post-training knowledge assessments provided by the HBB AAP curriculum and a self-evaluation questionnaire developed by master trainers in collaboration with the Department of Pediatrics and Child Health. Although the knowledge test is a validated tool, the self-confidence evaluation was not formally validated. Furthermore, the study did not assess trainees’ practical skills using an objective structured clinical examination. The absence of OSCEs in the study assessment does not imply a limitation in the training content itself, but rather a gap in the ability to objectively measure skill acquisition. Thus, in cooperation, the clinical assessment would provide a more robust measure of the trainees’ capacity.
As a peer-led program, another study limitation is related to the experience level of master trainers. While they were carefully selected based on previous performance, communication, and leadership skills, many lacked real-world clinical exposure to neonatal resuscitation. This occasionally presented challenges, particularly in teaching technically demanding skills like bag-mask ventilation. Although faculty members provided supervision during sessions, future programs may benefit from a more structured mentorship model to support peer trainers as they build the confidence and skill needed to teach hands-on procedures effectively.
Recommendations
HBB-KU envisions establishing a system of participant tracking and re-evaluation involving continuous monitoring and assessment of trained participants, a one-year HBB training determining the effectiveness of the program. This future vision will provide insightful information on areas where our HBB training needs to be improved and refined, which will maximize the effectiveness of the training. Additionally, HBB-KU has pioneered a successfully implemented peer-led program and anticipates inspiring other training institutes to adopt and execute a similar model, working together in lowering NMR in Tanzania: one breath at a time.
Conclusion
The study findings highlight how effective the peer-led approach employed in the HBB-KU alliance training program is at enhancing the skills of future HCPs, particularly in resource-limited environments. HBB-KU initiative stands as a promising peer-led model for addressing critical challenges of neonatal mortality. Research, innovations, and the implementation of clinical evaluation tools will all be crucial to the initiative's long-term viability and wider implications for medical education and practice for our future HCPs.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251358037 - Supplemental material for Peer-Led Neonatal Resuscitation Training: Experience of Kairuki University
Supplemental material, sj-docx-1-mde-10.1177_23821205251358037 for Peer-Led Neonatal Resuscitation Training: Experience of Kairuki University by Raidah R Gangji, Leonard Malasa, Gambuna D Koya, Aliasgar Khaki, Felician Rutachunzibwa, Maulidi Fataki, Florence Salvatory Kalabamu, Esther M Johnston and Esther Mwaikambo in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors would like to thank the Department of Pediatrics and Child Health at Kairuki University for their continuous support in the implementation of the HBB-KU initiative. The authors would like to appreciate Dr Rahma S. A. Baabde, Dr Sara M. Siwji, Dr Meshack M. Morice, and Dr Albert Kalya for their work, which has significantly contributed to the HBB-HKMU Alliance program. Additionally, the authors would also like to extend their gratitude to all those involved, including the dedicated master trainers, for their hard work and commitment have been instrumental in the positive outcomes of the HBB-HKMU Alliance program.
ORCID iDs
Ethical Considerations
The Kairuki University Research and Ethics Committee was informed of this educational program. In accordance with university guidelines for low-risk educational activities, formal ethical approval was not mandated. The program was identified and acknowledged by Kairuki University.
Consent to Participate
Verbal informed consent was obtained from all participants prior to inclusion. The study posed minimal risk, and participation was voluntary.
Authors’ Contributions
RRG, LM, and GDK: conceptualization; RRG, LM, FSK, and EMJ: methodology; RRG, GDK, and AK: training coordination; RRG, GDK, and AK: data collection; RRG and GDK: data analysis; RRG, LM, GDK, and FSK: manuscript drafting; LM, FR, MK, FSK, EMJ, and EM: project coordination; LM, FR, MK, FSK, EMJ, and EM: supervision. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.