
Abstract
Objectives
A global shortage of healthcare professionals emphasizes the need for expanded clinical training capacity of medical students worldwide. Patient-centered clinical teaching, the pillar of clinical education, has become the main challenge for medical educators, in all clinical disciplines. The solution will, inevitably come, in three dimensions: elongation of learning hours throughout daytime and during evenings, extending from hospital-based education to community clinics and assimilating a larger volume of simulative training.
Methods
The embodiment of two of three dimensions (extension along the day and to clinics-based teaching) is realized in our NAC—Neurology Academic Clinic: a teaching-centered complex of ambulatory neurology clinics, functioning within a tertiary medical center in the afternoon and evening hours.
Results
Establishment of NAC enabled us to extend our patient-centered clinical teaching, during a 40-week teaching year, to: (A) a larger audience of medical students, with up to 320 students annually, experiencing high-quality, personalized teaching; (B) significantly shortening patients’ waiting lists to highly demanded specialized neurologists with an average shortening of 90 days for the NAC patients; (C) enable our in-house physicians to become “full timers” on an educational basis with financial incentives, potentially increasing their yearly salaries by 14,000$, along with extended academic credits and considerable contribution to future generations.
Conclusion
The NAC model, described in this article, is considered successful and is currently duplicated to other clinical disciplines including infectious diseases, gastroenterology, and psychiatry.
Introduction
Addressing the Worldwide Crisis of Dwindling Professional Personnel in Healthcare Systems
Worldwide, especially after the COVID-19 pandemic, healthcare professionals are becoming harder to both train and maintain. 1 Numerous factors were suggested as explanations for the above, yet effective solutions are still missing. Recently, 2023 world economic forum in Davos, it was stated that by 2030, there will be an estimated shortfall of 10 million healthcare workers worldwide, and that urgent and extreme action is needed currently to improve recruitment and retention of the global healthcare workforce. 2 The AAMC, Association of American Medical Colleges, in its March 2024 report declared that physician demand is projected to continue to grow faster than supply, leading to a total projected shortage of between 13,500 and 86,000 physicians by 2036. 3 This problem becomes more pronounced regarding training and retention of physicians. A Lancet study in 2022 estimated that the world has 104 million health workers and 12.8 million physicians giving a global physician density of 16.7 per 10,000 population. 4 The problem is even greater in Israel, in which the number of physicians per capita (2023 data) is lower than in the OECD at 3.1 versus 3.5 per 1000 population, respectively. In their report, Treister-Goltzman and Peleg claim that the problem is likely to worsen as the number of medical students in Israel cannot increase quickly, especially due to shortage of adequate clinical training sites. 5 In their commentary, Angel and Fire relate, in part, the prospect of shortage of physicians in Israel to the “Yatziv” Reform, substantially reducing the list of foreign medical schools considered eligible for Israeli medical students. 6 This reform aims at increasing the young physicians’ quality, yet at the same time, reducing the influx of young Israeli physicians into our healthcare system.
The Challenge of Attaining Adequate Clinical Training Capacity in Israel
Worldwide, the reservoir of clinical teaching opportunities (named as “fields,” “attachments,” “placements,” etc.) is never enough.7,8 The holy grail of medical education, bedside teaching, is a precious resource, not to mention the clinical teachers and their invaluable experience in the art of bedside teaching. As Sir William Osler stated, “Medicine is a difficult art to acquire” and in his article from the year 1903 “put the students in the wards” as part of his statement that “there is need for a radical reform in our methods of teaching senior students.” 9
Currently over half of medical students’ clinical training occurs in inpatient settings. 10 Integration of medical students into outpatient clinics presents challenges for physicians, students, patients, and faculty. For physicians: (i) Limited time to balance patient care with medical teaching,11,12 (ii) Productivity pressures negatively influence the time allotted for educational discussions which results in reduced overall efficiency in ambulatory setting, 11 and (iii) Faculty engagement - reduced motivation to teach while managing patient loads. For students: (i) High students to patient ratio diminish each student potential for intimate clinical experience with patients, 11 (ii) Lack of case diversity diminish their “gestalt” of clinical reasoning, and (iii) Lack of follow up continuity in outpatient settings narrow their understanding of clinical evolution along a timeline. 13 For patients: some patients are reluctant to take part in a teaching environment 11 and should have their own self-driven incentive for collaboration. For the faculty; inadequate feedback and evaluation of overall clinical performance. The need to overcome these challenges have been recognized globally.11–13 This brought the idea of personalized teaching and medical care by the establishment of the NAC (Neurology Academic Clinic).
Extending Medical Teaching Opportunities in Time and Space
There is no doubt that only clinical-based training serves as the beating heart of medical education. Only through direct involvement in the physician-patient encounter can medical students develop essential clinical skills.14–16 Since this essential component is in critical shortage worldwide, surplusage of clinical placements for patient-centered clinical teaching should come in three dimensions: elongation of learning hours throughout day and night, extending from hospital-based education to community clinics and applying simulative learning on a much larger scale. This envelope of placements and teaching opportunities should be at the service of two main types of patient-centered clinical teaching: endowing students with the principles and structure of clinical reasoning and training and assessment of skills and competencies taking place in the settings of an intimate student-patient meeting. Figure 1 depicts this structural model of clinical teaching in our medical center.
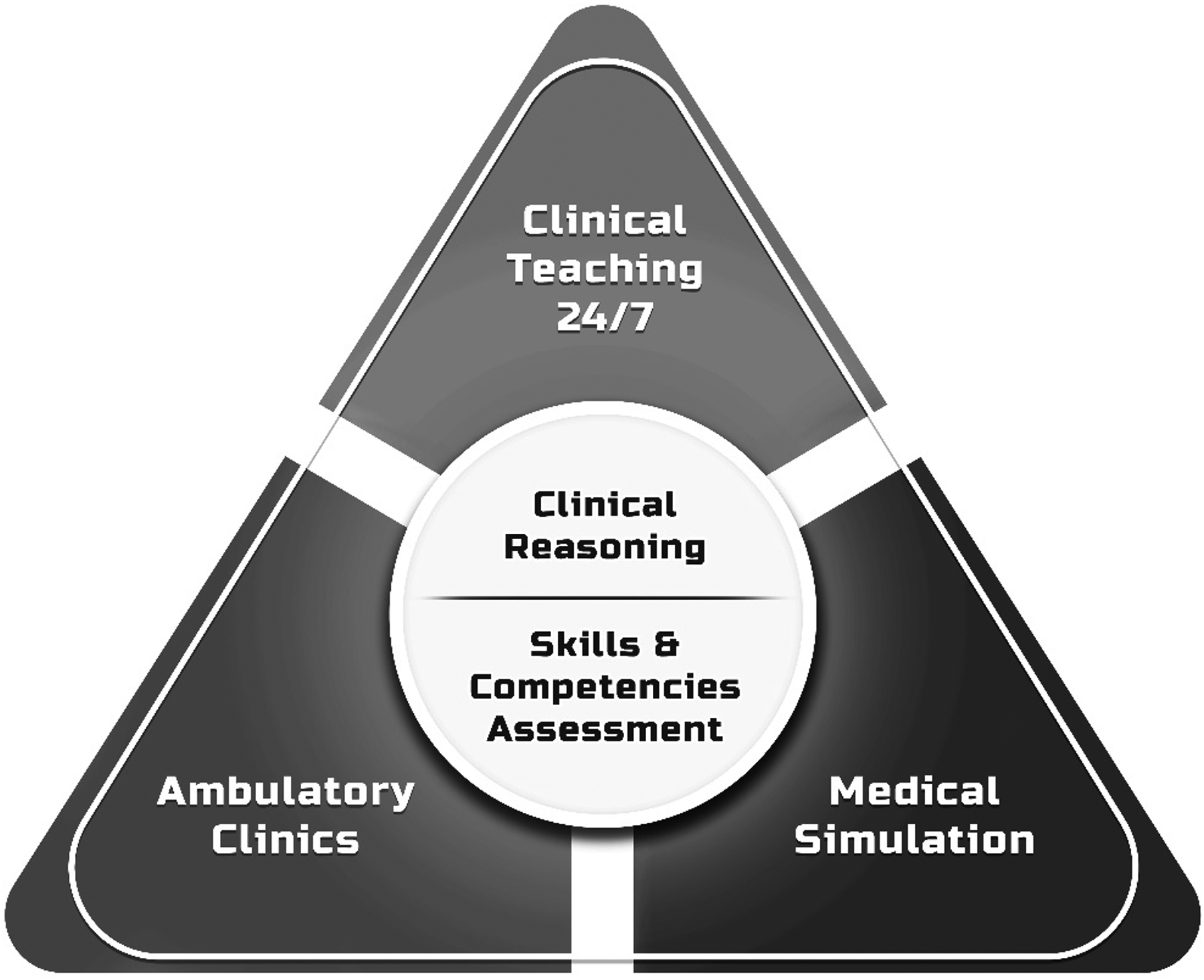
Structural Model of Clinical Teaching Expansion in the Chaim Sheba Medical Center.
Methods
The Case of NAC (Neurology Academic Clinic)
The Neurology Academic Clinic (NAC) represents an innovative initiative that prioritizes delivering medical education within a personalized environment. This distinctive model empowers students to extract insights directly from patient interactions, creating an environment conducive to the enhancement of their medical knowledge. Moreover, this platform exposes the student into the thought processes of expert neurologists during patients’ decision-making processes, offering valuable perspectives on the complexities of diagnostic and therapeutic decision-making. By directly engaging with patients, students gain insights that foster a deeper understanding of medical complexities through an exploration of considerations, benefits, and risks. Beyond the professional aspect, in this platform the student learns from the patient-physician interaction how to provide compassionate care, build trust and offer explanations regarding diagnosis and therapy, thereby fostering patient engagement in the treatment process.
The NAC offers several advantages for both clinical neurologists and patients. Firstly, it allows neurologists more time to dedicate to each patient, enabling thorough processing of their cases and providing ample opportunity to educate students about various conditions with a personal approach to both students and patients. This high-quality educational tool is especially important in the realm of neurology, as part of the need for abolishing “neurophobia,” a term coined for students’ and young physicians anxiety from the hardship encountered when they try to fill the gap between their basic neurological knowledge and the clinical neurological know-how.17,18 Additionally, the NAC works as an afternoon overtime session, which come with higher salaries. This serves as a source of motivation for the experts involved. At the beginning of NAC we knew that increased salaries would serve as an incentive for neurologists to attend this clinic. The fact that we never had a gap in filling these placements with physicians ascertained our initial assumptions. From the patients’ perspective, the clinic facilitates quicker appointment scheduling compared to the typical six-eight month wait for neurologist visits. This rapid response capability proves invaluable, particularly in cases of progressive exacerbation or emergence of new symptoms, ensuring timely and effective medical attention.
Results
Table 1 detail the advantages endowed with each stakeholder by the NAC and the steps that had to be taken in order to make sure that all stakeholders’ interests are kept.
Detailed Advantages Endowed by NAC to All Relevant Stakeholders.

Discussion
Future and present challenges of the global healthcare systems necessitate innovative solutions. In the current project described, we addressed one of the most difficult, rate-limiting steps of providing healthcare systems with well trained professional personnel: the low capacity of clinical teaching placements for medical students. We describe not only our thoughts and planning but also the results of a preliminary innovative project. It should be emphasized that Israel suffer from a shortage of clinical placements for medical students, with over 60% of our physicians being educated outside Israel. Their medical education, especially at the “clinical years” is undoubtedly less “tuned” to the needs of their future patients and healthcare system.
We addressed core challenges that have concerned medical educators for many years. As these were stratified in a BMJ review back in the year 2003 20 (without significant improvements ever since) include time pressures and the competing demands of balancing student clinical teaching with the clinical evaluation of patients, the NAC aimed to solve these main challenges. Other administrative and research demands were mostly not addressed in our model. Another challenge is that clinical teaching is often opportunistic, which makes tutorial planning more difficult 21 —resolved by the pre-planned teaching capacity of the dedicated clinic, also addressing the challenge of increasing numbers of students - attended by additive clinical fields.
NAC, Neurology Academic Clinic, operated during the afternoon and evening hours, dramatically expanded our clinical teaching potential in this unique clinical discipline. We did not approach all stakeholders with a demand for expansion, rather, we prospectively addressed each and every step of the process and served all stakeholders with solutions for their potential obstacles down the road for execution of the NAC. Moreover, we also made sure that all stakeholders will benefit from the process. This is a “tough mission” since, unfortunately, medical education is not easily prioritized in-hospital managements and governance bodies. 22 The process necessitates an in-hospital unit that would be engaged with medical education as its main business. In the Chaim Sheba Medical Center (SMC), such a unit was established in the year 2021 and ever since, is engaged with promotion of medical education in SMC itself and nationwide all around our country.
Harnessing the clinical unit/discipline is of utmost importance. One of the most promising young specialists in the relevant discipline (in the case of NAC—the neuroscience division) was recruited by the education authority and advocated the NAC as part of her main workplace challenges. Support from her superiors was invaluable. Also, the financial and managerial units within the hospital management were actively engaged in order to supply some of the essential components needed for the stakeholders: financial incentives for both clinical and non-clinical personnel, alongside with reduced workload of the educational clinic were mandatory and necessitated support in the highest levels of our medical center management.
After one year of operation, the NAC results in considerable positive results: A larger audience of medical students was thought in our medical center, with up to 320 students’ “chairs” totally added (for both students who studied abroad, those who were added to existing faculties and those who are enlisted to newly opened faculties in our country). Students feedback was positive, reflecting the high-quality, personalized teaching experience they had. Also, we achieved significant shortening of patients’ waiting durations to highly demanded specialized neurologists with an average shortening of 90 days for the NAC patients including four main disciplines within NAC: headache clinic, neuro-immunology clinic, epilepsy clinic and movement disorders clinic. Our physicians, as key-stakeholders, benefited from the option of becoming “full timers” on an educational basis with financial incentives, potentially increasing their yearly salaries by 14,000$, along extended academic credits and considerable exposure to the next generation of young physicians. Additionally, non-medical stuffing of the NAC was not an obstacle with the medical center management support in terms of financial incentives and lower throughput demands. The project as a whole necessitated subsidizing by the institutional education authority on top of tuition fees paid by Israeli medicine students who study out of Israel. These students highly value this opportunity of clinical teaching in a personalized setting in SMC over the clinical teaching offered in foreign language at their university hospitals, despite the high costs associated with clinical training within the NAC model. We foresee a potential for financial balancing of future clinics once they are approved by existing and new medicine faculties (already affirmative for afternoon teaching in their contracts with our medical center).
Conclusion
Successful activity of NAC serves as a model within our medical center for further expansion of clinical-education placements in other disciplines and should serve also as a model for the construction of similar clinics in other hospitals nationwide. In the current article we detailed the benefits endowed and the expected throughput from each stakeholder. We foresee this effort as an essential step towards ameliorating the future of healthcare systems.
Footnotes
Author Contributions
All authors contributed significantly to the research and to the manuscript drafting and final version submitted to publications.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.