
Abstract
Background
The coronavirus disease 2019 (COVID-19) pandemic has led to considerable advances in medical education through technological integration. The crisis generated by the pandemic in medical practice, education, and evolving technology has led to changes in the skills of medical professionals. This study aimed to examine the competencies required of medical students in the post-pandemic era.
Methods
We conducted 2 mixed-methods studies. Study 1 explored medical students’ necessary competencies after the COVID-19 pandemic. We conducted group work with faculty members and students from the Chiba University School of Medicine, captured proposed competencies, discussed them, and qualitatively analyzed the group work data using content analysis to extract the competencies. Study 2 was a secondary data analysis that compared the categories identified in Study 1 with the competencies required prior to the COVID-19 pandemic, which were extracted from the websites of all 82 medical schools and colleges in Japan, to identify the differences in competencies before and after the pandemic.
Results
Study 1 resulted in the identification of 12 categories and 62 subcategories. The results of Study 2 showed that the increased occurrence of competencies was related to the utilization of information and communication technology (ICT) and artificial intelligence (AI), self-management, information gathering and explanation, liberal arts and generic skills, and exploring medicine and medical care/research presentations. The prevalence rates of these factors prior to the COVID-19 outbreak were 17.1%, 28.0%, 39.0%, 41.5%, and 48.8%, respectively.
Conclusions
Competency-based medical education in ICT, self-management, and medical exploration has become increasingly important after the pandemic. Therefore, it is necessary to develop an educational curriculum to enable medical students to acquire these competencies. The study findings contribute to the literature on medical education and offer valuable insight into setting effective academic goals and designing suitable curricula for undergraduate medical students in the post-pandemic era.
Keywords
Introduction
Infectious diseases caused by the coronavirus disease 2019 (COVID-19) in December 2019 spread globally, and the World Health Organization (WHO) declared a pandemic in March 2020. 1 During the pandemic, the number of people infected with COVID-19 rapidly increased worldwide, resulting in substantial changes in medical care and education.2,3 The value of online and virtual education was widely recognized during this period, and there is a conviction that medical education might change permanently even after the WHO declared the end of the pandemic in May 2023. 4 In Japan, the pandemic had a tremendous impact on education; various policies and guidelines were implemented during the national emergency, which accelerated the promotion of the use of information and communication technology (ICT) and distance education in schools and universities. 5
Considerable research on medical education practices during the pandemic has been conducted. One study examined the efficacy of an online simulated clinical practice that relied on a learning management system, illustrating an effective educational method capable of being utilized with minimal preparation and resources. 6 In addition, attempts have been made to implement active learning such as case-based learning, problem-based learning, team-based learning,7,8 and asynchronous online learning tools9–11 that use prerecorded lectures along with simultaneous 2-way communication. The accumulation of previous research on using interactive communication has enabled educational activities that are free from the constraints of time and place. 12
The COVID-19 pandemic affected not only learning strategies but also learning goals. It has been pointed out that the pandemic had a significant impact on medical education and stimulated a rethinking of concepts pertaining to medical competence. 4 Outcome-based education is mainstream in current medical education and has been adopted worldwide. The competencies required of medical professionals are influenced by regional, political, social, and economic conditions.13,14 The “WFME Standards For Basic Medical Education 2015” of the World Federation for Medical Education (WFME) states that “The medical school must define the intended educational outcomes that students should exhibit upon graduation.” 15 Medical schools and medical colleges in Japan are also required to comply with the WFME Global Standards for Quality Improvement. Furthermore, the impact of the COVID-19 pandemic on the learning outcomes of undergraduate medical education has not yet been examined. We considered Japanese medical schools to be suitable for data collection and comparative study because: (1) compared to other countries, the Japanese government required educational institutions to take strict measures regarding COVID-19, which had a major impact on medical education, and (2) many medical schools in Japan have been following WFME Global Standards for Quality Improvement prior to the pandemic. Therefore, the learning outcomes defined by each school were documented. There are 82 medical schools in Japan, undergraduate medical education spans 6 years, and high school graduates are eligible to enter medical school. 16
This study aimed to explore the competencies of medical students after the COVID-19 pandemic as considered by the faculty and students involved in undergraduate medical education by investigating the impact of the pandemic on medical practice, medical education, and developments in technology. The study findings provide valuable insights for establishing academic goals and developing curricula for undergraduate medical students in the post-pandemic era.
This study focused on data collected during the review of the pre-COVID-19 learning outcomes of the Chiba University School of Medicine, a national university corporation, which had been formulated in 2008 and revised in 2013. The learning outcomes before COVID-19 consisted of 36 competencies divided into the following 6 categories: (1) Ethics and professionalism, (2) Communication, (3) Medical and related field knowledge, (4) Clinical practice, (5) Disease prevention and health promotion, and (6) Scientific inquiry. 17
We gathered the opinions of the faculty and students who experienced medicine and medical education during the pandemic to understand the post-pandemic competencies. We evaluated the competencies that undergraduate medical students should acquire post pandemic to improve the learning outcomes that have already been established at Chiba University School of Medicine. In addition, we examined how these competencies differed from those required prior to the COVID-19 pandemic.
Methods
We conducted 2 mixed-methods studies. In Study 1, we performed group work and coded the data using content analysis, a qualitative research method, to extract the competencies. In Study 1, data were collected through group work by faculty, staff, and students at Chiba University School of Medicine. In the group work, the first step was for each group member to write down a competency idea on a card, and the second step was to brainstorm based on the content of the cards. The researchers in this study divided the collected cards into categories and counted the number of each category. The reporting of Study 1 follows the guidelines of the Consolidated Criteria for Reporting Qualitative Studies 12 (see Supplemental 1). 18
Study 2 was a secondary data analysis that compared the results in Study 1 with those of other universities in Japan before the COVID-19 pandemic and identified the changes in learning outcomes after the pandemic. Data were collected from each university's web page and reviewed based on the data. The number of schools was counted for each category. A series of data collection and analysis was conducted in the Japanese, and the results have been translated into English for paper.
Setting
Study 1: Identification of the Proposed Competencies After the COVID-19 Pandemic: Participants and Contexts
This study was conducted and based on data collected at an annual workshop held at the Chiba University School of Medicine. The workshop required the participation of at least one faculty member from each of the basic and clinical medicine faculties. Twelve students who wished to participate were added to the group. The participants of this workshop were selected as appropriate for conducting a study of the medical school curriculum because the diverse specialties of the participants allowed for the collection of opinions from multiple perspectives. A total of 78 participants participated in the study, including 66 faculty members (16 professors, 11 associate professors, 18 lecturers, 20 assistant professors, and 1 researcher) who belonged to the basic medicine or clinical medicine departments of Chiba University School of Medicine, were engaged in medical education, and wished to participate in the workshop. A total of 12 students (2 first-year, 2 second-year, 2 third-year, 2 fourth-year, 2 fifth-year, and 2 sixth-year students) from Chiba University School of Medicine also participated. Participants were divided into 9 groups of 8 to 10 members each. We tried to ensure that all groups included 1 or 2 students and that the faculty members were not biased toward their specialties. Informed oral consent was obtained from all the participants prior to the group work.
1-1. Group Work
In August 2020, a group work session was held to discuss the topic, “What is the essential competencies for students of Chiba University School of Medicine to acquire upon graduation?”
The workshop sought to initiate a discussion on the proposed competencies among the participants. Participants were informed that this work was not limited to the learning outcomes currently defined by Chiba University School of Medicine and existing theories and research. We encouraged them to provide their opinions based on future social predictions. To ensure that they were given equal opportunities to express their ideas, participants were instructed at the beginning of the workshop to fill out one card for each proposed competency. Only the proposed competencies and no other information, such as the name of the person who completed it, were furnished on the cards.
Facilitators were selected from the faculty of Department of Medical Education, 6 medical education researcher and physician, and 3 medical social science researchers. Facilitators in each group instructed group members how to write the cards, and each participant repeatedly filled out about 5 to 6 cards until the saturation point of opinions was achieved. After filling out the cards, facilitators encouraged the participants to brainstorm the group's suggestions. The time allocated for the entire workshop was 60 min. Depending on the progress of each group, about 20 min were allocated for completing the cards, and the remaining time was used for brainstorming.
1-2. Data Collection and Content Analysis
We collected the cards after the group work was completed. Each card was listed as a unit of analysis.19–21 One medical education researcher and physician (HY) and 2 medical social science researchers (ZT and MO) performed coding for the units of analysis. These 3 researchers were experienced in qualitative research with content analysis.
First, the subcategories were coded. The 3 researchers independently conducted the investigations, and opinions were not exchanged during coding. Second, they repeatedly exchanged opinions based on the coding results until they reached an agreement. When consensus could not be reached, a supervisor who was a researcher in medical education and a physician (SI) advised them on how to determine the final subcategories. They then grouped the subcategories into categories using the same method used for coding the subcategories. Figure 1 presents examples of the coding process.

Examples of Coding Process.
Study 2: Comparison of the Required Competencies Before and After COVID-19
2-1. Data Collection
We gathered data on the learning outcomes prior to the COVID-19 pandemic from the websites of all 82 medical schools and colleges in Japan between April 2021 and March 2022. These universities posted lists of the competencies to be acquired by the time of graduation at the end of the curriculum on their respective web pages “Outcomes at Graduation,” “Competencies at Graduation,” or “Diploma Policies.”
2-2. Data Analysis
The learning outcomes developed before the pandemic were compared with the categories in Study 1. For each university, we made a judgment on whether a category was mentioned. If we found an identical term in a document, we considered it even if the wording was partially different. In this survey, the full texts of these documents were reviewed and tabulated according to each school to determine whether they were listed or not. The schools’ names were anonymized.
Three researchers (HK, ZT, and MO) independently conducted the study; if they did not agree on the results, they discussed it with the supervisor. The comparison criteria were repeatedly reviewed until a consensus was reached among the researchers. The relevant criteria are listed in Table 1.
Criteria for How Often the Competencies Identified in Study 1 were Mentioned Before the Pandemic.

Abbreviations: AI, artificial intelligence; ICT, information and communication technology.
Results
Study 1: Group Work and Content Analysis to Identify the Required Competencies After COVID-19
The 351 cards from the group work were collected. The 3 coders and supervisor discussed and classified them into 12 categories and 62 subcategories. The category names and number of cards in each category were as follows: (1) Medical practice/Patient safety (n = 49), (2) Professionalism/Ethics (n = 45), (3) Teamwork and communication (n = 44), (4) Exploring medicine and medical care/Research presentations (n = 43), (5) Knowledge of medicine and medical care (n = 41), (6) Information inputs and outputs (n = 31), (7) Respect and building trusting relationships among patients (n = 27), (8) Use of ICT and AI (n = 19), (9) International perspectives and language skills (n = 19), (10) Lifelong learning (n = 14), (11) Self-management (n = 12), and (12) Liberal arts and generic skills (n = 7) (Table 2). As shown in Figure 2, the categories of competencies can be divided into “Medical competencies” and “Scientific competencies.”

The Essential Competencies for Medical Education.
Themes and codes identified in the content analysis

Abbreviations: AI, artificial intelligence; ICT, information and communication technology. *( ) = numbers of codes.
Study 2: Results of the Comparison of the Competencies Extracted in Study 1 With Those Required Before COVID-19
Figure 3 shows the total number of schools and percentage of mentions in domestic universities for the 12 categories. The categories that were not given much importance before the COVID-19 pandemic but emerged as crucial during the COVID-19 pandemic were: 8. Use of ICT and AI (17.1%), 11. Self-management (28.0%), 6. Information inputs and outputs (39.0%), 12. Liberal arts and generic skills (41.5%), and 4. Exploring medicine and medical care/research presentations (48.8%). Many universities had considered other categories as vital prior to the COVID-19 pandemic.
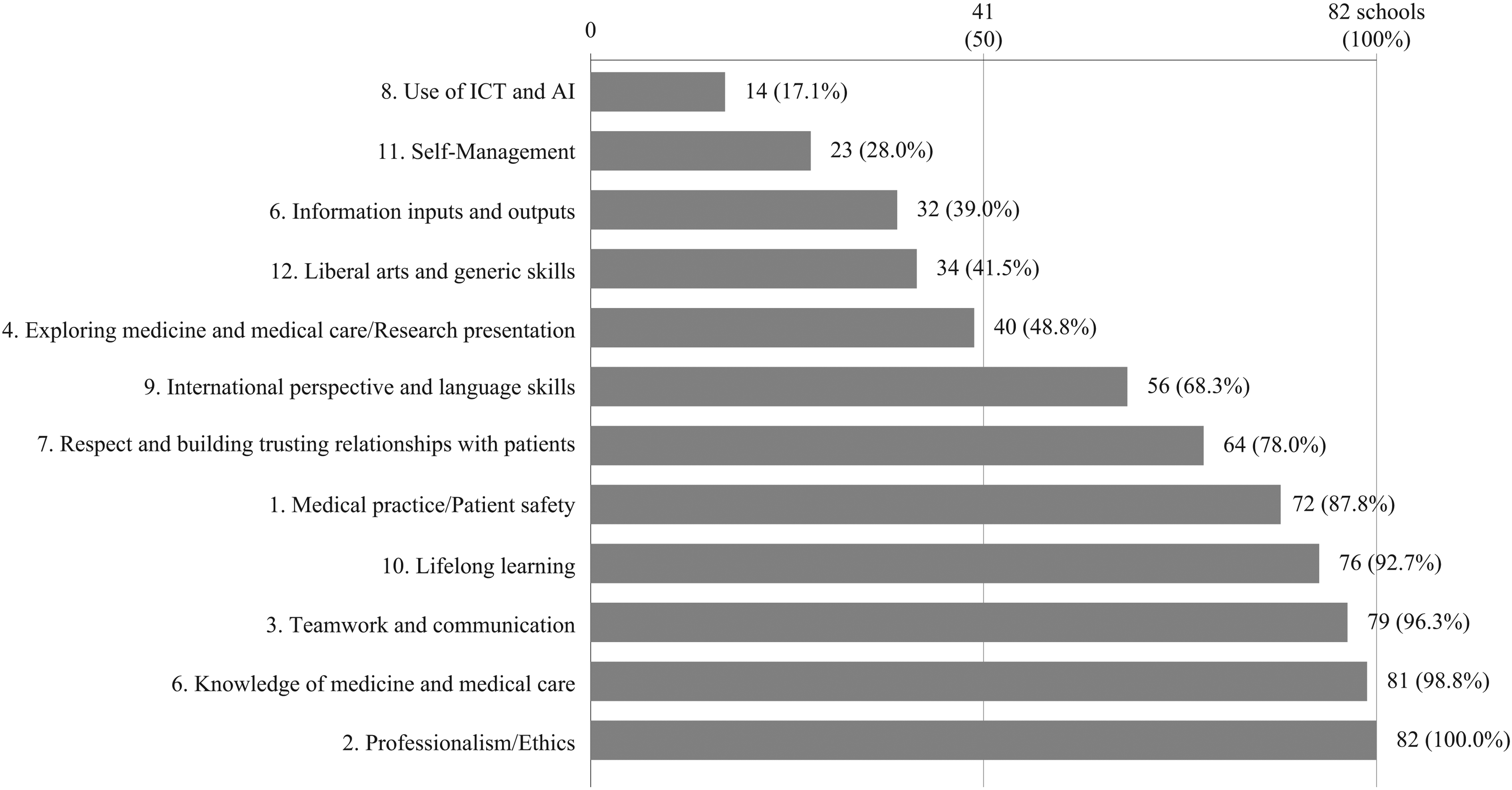
The Number of Universities that have the Same Learning Outcomes Extracted in Study 1.
Discussion
This pioneering study examines the competencies of medical students after the COVID-19 pandemic in mixed groups of faculty members and students and explores the changes caused by the pandemic. We identified the following competencies as necessary after the pandemic: Use of ICT and AI, self-management, information inputs and outputs, medical exploration and presentations, and liberal arts and generic skills. The findings revealed that professionalism/ethics, knowledge of medicine and medical care, teamwork and communication, and lifelong learning had been defined as competencies by more than 90% of universities in Japan before the COVID-19 pandemic.
The use of ICT and AI has been the focus of research because the development of telemedicine in actual clinical settings was promoted at a rapid pace along with the introduction of ICT and AI in medical education. ICT and AI are increasingly used in the field of medicine. In addition, the application of AI and programming raises expectations for increased work efficiency. These technologies will continue to advance in the future, and medical students are expected to be proficient in using such cutting-edge technologies. It is suggested that medical educators should gain expertise in ICT and AI too.22,23 The use of ICT and AI in healthcare has been focused on before the pandemic and would have developed even if the pandemic had not occurred. This result suggests that participants believed that the pandemic played a role in driving the development of ICT.
Self-management is associated with burnout among healthcare professionals. Burnout among healthcare workers was consistently high. 24 It became a cause of great concern for healthcare staff working during the COVID-19 pandemic, and its impact was more burdensome for front-line physicians. 25 In addition, the shortage of doctors remained a major challenge. 26 This proved to be an opportunity for physicians to become more aware of their own physical and mental health needs. Improving awareness about effective mental healthcare practices and resilience to prevent burnout among physicians is crucial.
Information inputs and outputs are essential for better medical practice and development. Publishing research, presentations at conferences, and medical statistics are also important. Ten Cate et al found that competent physicians are not always aware of what is best for their patients and are overwhelmed by uncertainty. 4 Sackett et al pointed out the need to develop skills to continue to select the best care based on evidence-based medicine. 27 Recently, the rapid increase in the amount of available medical information has become a challenge in medical education. 28 Therefore, it is necessary to identify credible information from numerous resources. In their experience with the COVID-19 pandemic, Lungeanu et al noted that knowledge of data science and the ability to understand the results of research papers can be critical complements to clinical practice. 29 Thus, it is essential for medical professionals to stay updated on the latest research trends and continue to explore new findings. Maintaining up-to-date knowledge is a competency related to lifelong learning.
With the development of medicine, presenting individual and collective experiences is crucial. In recent years, publication methods have extended beyond conventional oral presentations and written papers to include social media. Acquiring skills to deliver information through new media platforms is gaining attention. The subcategories of information transmission, considerate presentation, and appropriate use of social media are essential competencies, suggesting that they are not only input but also output methods of information.
The term liberal arts and generic skills are used to describe a broad range of knowledge and skills that are not limited to the field of medicine. Zouaoui et al emphasized that skills such as knowledge, communication, and planning are essential for facing complex challenges. 30 It is believed that these skills are necessary to cope with the increasing amount of medical information and to improve problem-solving abilities.
Japan's national curriculum, the Model Core Curriculum for Medical Education, was revised in 2022. A section on “Information Technology” that reflects the increased use of information science and technology in medicine and healthcare was added. 31 The use of information science and technology in medicine is expected to increase in the future.
Additionally, a new system for reforming the way doctors work was introduced by Japan's Ministry of Health, Labour and Welfare in April 2024. This law regulates doctors’ long working hours and promotes task-shifting and task-sharing of some duties among medical professionals. 32 This system is expected to make it easier for doctors to manage their own health.
Limitations
There are several limitations to this study. First, there is a limitation regarding the research sampling. The participants were limited to teachers and students at a single institution in Japan. Most of the participants were faculty members, so it may have been complicated for 1 or 2 students in each group, or even for physicians in the early stages of their careers, to candidly express their opinions. It was also challenging to gather opinions from the public at large.
Second, a secondary data analysis was made only at the category level and not at the subcategory level. Third, only the presence or absence of each category mentioned on the website of the colleges was aggregated without considering the number of mentions within the same university's learning outcomes, whether at the headline or main text level or the importance of the category in the context. Future research should address these limitations. Fourth, although the impact of COVID-19 was significant, the changes in attitudes toward ICT and AI in medical education and self-management cannot be attributed solely to the impact of COVID-19. Research on technological advances, health worker burnout, and self-management had been accumulating prior to the onset of the novel coronavirus infection pandemic. It is necessary to consider the impact of factors other than COVID-19.
Conclusions
Competency-based medical education through ICT, self-management, information inputs and outputs, and medical exploration has become increasingly important since the COVID-19 pandemic. The study results indicate that it is necessary to design an appropriate educational curriculum to enable medical students to acquire these skills. The findings of this study have valuable implications for policymakers to promote competency-based medical education in the post-pandemic era.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251333502 - Supplemental material for Exploring the Essential Competencies for Medical Education in the Post-COVID-19 Pandemic Era: A Mixed-Methods Investigation at a Japanese Medical School
Supplemental material, sj-docx-1-mde-10.1177_23821205251333502 for Exploring the Essential Competencies for Medical Education in the Post-COVID-19 Pandemic Era: A Mixed-Methods Investigation at a Japanese Medical School by Misaki Onodera, Zaiya Takahashi, Hajime Kasai, Hidetaka Yokoh, Kiyoshi Shikino, Yasuhiko Kimura, Ikuo Shimizu, Kazuyo Yamauchi, Mayumi Asahina and Shoichi Ito in Journal of Medical Education and Curricular Development
Footnotes
List of Abbreviations
Acknowledgments
ORCID iDs
Ethical Considerations
This study was approved by the Ethics Committee of Chiba University (approval no. 3425). Informed consent was obtained from all subjects prior to commencement of the study. The study database was anonymized.
Consent to Participate and Publication
Informed consent for participation and publication was verbally obtained from the participants before the study commenced.
Author Contributions
MO, ZT, HY, and SI planned, designed, and conceived the study. MO, ZT, HY, KS, HK, and MA facilitated the group work and collected data on the proposed competencies in Study 1. MO, ZT, HY, and HK performed the coding in Studies 1 and 2. SI reviewed the findings of Studies 1 and 2. MO drafted the manuscript. ZT, HK, KS, IS, KY, and SI performed the manuscript review and editing. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Preprints
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.