
Abstract
INTRODUCTION
Residency programs face increasing expectations to grow competency in system-based practice and quality improvement (QI) among trainees. Organizations like the American Board of Internal Medicine and the Accreditation Council for Graduate Medical Education have included QI knowledge in their recertification and accreditation requirements. We describe our experiences over a decade of sustaining a longitudinal experiential QI curriculum at a large Internal Medicine residency program.
METHODS
Each resident participated in interactive seminars as well as a faculty-mentored, team-based QI project. Each project was formally evaluated at an end-of-year poster presentation.
RESULTS
One hundred thirty-six projects were completed between 2007 and 2016. A presurvey of 51 PGY-1 residents (59%) and a postsurvey of 50 PGY-2 and PGY-3 residents (46%) demonstrated increased comfort leading a QI project and improved knowledge of QI principles. We continue a modified version of the curriculum to accommodate the residency program's restructured ambulatory teaching experiences and the impacts of the COVID-19 pandemic.
CONCLUSION
Implementing a performance improvement curriculum based in a resident continuity clinic is feasible and affords several advantages. In applying QI methodologies, residents learn how to measure adherence with current evidence-based medicine guidelines and develop interventions to maintain positive momentum within the reality of busy clinical practice.
Keywords
Introduction
Organizations like the American Board of Internal Medicine 1 and the Accreditation Council for Graduate Medical Education (ACGME) 2 have included quality improvement (QI) expertise in their recertification and accreditation requirements. As part of the ACGME competency in practice-based learning and improvement, all residents are required to “demonstrate the ability to systematically analyze their practice using quality improvement methods, and implement changes with the goal of practice improvement.”1,2 Though less is known about the impact of QI residency curriculum on graduates’ future practice behaviors and patient safety outcomes, prior work has suggested that resident-run projects may lead to improved outcome measures, such as rates of cancer screening 3 or diabetes care.4–6 Implementing such a requirement requires significant resources, including resident and faculty time and quality improvement expertise.7–9
Some programs report resident participation in QI activities as part of elective or research time10,11 and are generally focused on the inpatient setting. Others integrate their performance improvement curricula into resident ambulatory block months and may limit resident involvement to a particular PGY level.12,13
Though most published QI curricula show improvements in knowledge and learner attitudes,14–16 very few studies set in large internal medicine residency programs incorporate both didactic and experiential learning modalities, despite the latter having been identified as a driving success when delivering curricula in QI and performance improvement. 16 One possible explanation for this discrepancy is that longitudinal QI project involvement can contribute to existing time pressures and increase reliance on supporting infrastructure such as administrative personnel, financial resources, and accessible information systems. Though some studies attempt to address this gap, these programs were either limited in scope12,17 or had less emphasis on direct patient care or outcomes. 18
Furthermore, a less explored area of focus is the utility of current residency QI curricula on fulfilling the Quintuple Aim of healthcare improvement, which has evolved in recent years to incorporate health equity as a critical driver of healthcare outcomes. 19 Such gaps may be addressed by heightened attention to the specific settings and patient population contexts in which QI curricular initiatives are implemented.
We describe our experiences over a decade of designing and implementing experiential core curriculum in quality improvement at Emory University's J. Willis Hurst Internal Medicine Residency Program. In this curriculum, residents demonstrated a working knowledge of the Institute of Healthcare Improvement (IHI) Model for Improvement through conducting a year-long outpatient QI project, which was evaluated for adherence to key elements of the Model for Improvement in an annual departmental poster presentation. In this article, we delineate the ways in which our program continually evolved to address common barriers to sustainable integration of QI curriculum, such as poor learner engagement, lack of expert faculty, or competing institutional/educational priorities. In so doing, we hope to inform health professions educators facing similar barriers in promoting the sustainable integration of education and training in quality improvement.
Method and Curriculum Design
We describe our QI program using Kern's 6-step design framework, a well-established model for critical curriculum development that has been shown to improve implementation and long-term sustainability. 20
Problem identification
The investigators closely reviewed the existing residency program curriculum and found no elements of formal or informal instruction in quality improvement. As stated in the introduction, there exists a growing imperative among experts and accrediting bodies to improve QI expertise through large-scale implementation of core curriculum.
Needs assessment of targeted learners
In the early years of the program's implementation (2012-2013), we conducted pre- and postcourse surveys to understand current resident experience and assess basic knowledge of QI skills (Supplemental Materials). The Likert scale-based survey consisted of both objective knowledge assessments on taught QI principles and questions on resident perceptions of the curriculum.
Goals and objectives
Learning objectives of the program dictated that learners should be able to (1) understand core concepts of quality improvement and patient safety, and (2) lead, coordinate, or participate in the design and implementation of QI initiatives at practice and/or system levels using a collaborative, multidisciplinary team approach as demonstrated by fulfillment of a year-long project.
Educational strategies
The program was led by a curriculum director, trained by the Emory Quality Academy in a 6-month faculty development program that was designed to give leaders core knowledge and skills to build a constructive workplace environment supportive of QI activities. Alongside the curriculum director were faculty facilitators, who were attending faculty in primary care who had expressed an interest in learning and teaching the QI curriculum. These faculty members received ongoing mentorship and guidance from Emory's chief quality officers, who led monthly faculty development sessions prior to residents’ small group sessions (totaling to 8 development sessions per academic year, prior to year-end poster evaluations). In addition to giving feedback, providing topic expertise, and monitoring team progress through monthly assignments, faculty facilitators also completed their own QI projects in parallel to the residents in order to attain hands-on experience and assess curriculum structure for iterative improvements.
The curriculum adhered to a team-based structure, wherein each team was composed of a PGY-2 “team leader” who scheduled regular team meetings between small group sessions and oversaw the project creation process, a PGY-1 “team helper” who assisted the team leader, and a PGY-3 “team coordinator” who facilitated interdisciplinary involvement with technicians, nurses, pharmacists, or other nonclinical personnel. The team leader also was charged with reporting team progress to the faculty facilitator at the end of each month and ensuring timely posting of completed assignments to the designated virtual workspace.
To familiarize residents with the Institute of Healthcare Improvement (IHI) model, 5 the PGY-1 residents participated in a workshop on applying QI tools during their orientation.
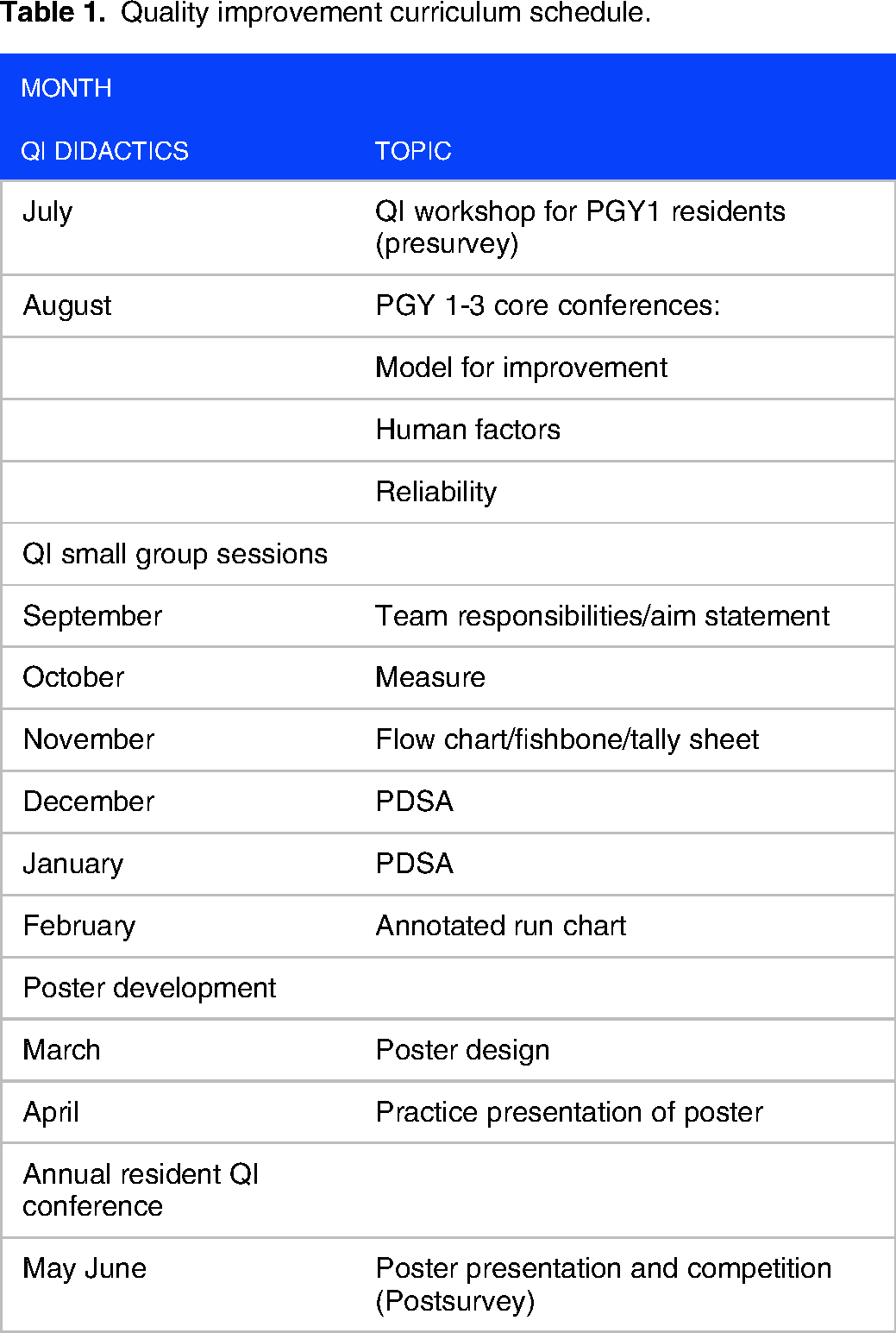
The workshop sessions were designed to be resident-run with the faculty facilitator present, focusing mainly on team-based participation and experiential engagement toward project development. Over the course of the following academic year, all residents were also exposed to 3 QI didactic “core conferences,” each focusing on one of 3 foundational QI principles: improvement, human error and cognition, and high reliability. These sessions were led by the Chief Quality Officer at the Emory Midtown Hospital location. The teams also met on a monthly basis in hour-long small group sessions as part of their ambulatory clinic schedule and were collectively involved in: (1) identifying a QI project focused on improving system based practice; (2) developing an aim statement; (3) determining measures to plot on a run chart; (4) applying QI tools (flow chart, fishbone diagram, or tally sheet) to determine tests of change; (5) running at least one test of change; and (6) plotting their data on an annotated run chart and creating a poster for the end-of-year conference (Table 1).
Quality improvement curriculum schedule.
Over the course of the academic year, residents participated in a team-based project and developed a poster utilizing a standard template (Figure 1) which was evaluated by experts in process improvement at a year-end conference. Project ideas were resident-driven and evaluated for including components of the Model for Improvement as defined on the Institute for Healthcare Improvement website. 5

Basic template for end of year resident poster presentations for their QI project.
Implementation
To ensure maximum resident participation, we implemented our curriculum at the 2 resident primary care continuity clinics: the Grady Health System (GHS) and The Emory Clinic. We also selected general medicine faculty preceptors in each of the clinics with a designated curriculum leader at each site.
The GHS Primary Care Center is an academic safety-net and hospital-based clinic that serves a historically marginalized patient population who face barriers to healthcare related to social determinants of health. The payor mix for majority of the patients at GHS are Medicare, Medicaid, or uninsured. Many patients seen in the clinic have comorbid conditions including type 2 diabetes, hypertension, high BMI, hyperlipidemia, and a history of tobacco use. In addition, several projects were performed in the International Clinic at GHS, which serves a primarily Hispanic and Latino/a/x population. The Emory Clinic practice is located on the Emory University campus and serve fewer patients on Medicaid or Medicare than those at Grady.
The Internal Medicine Residency program at Emory University School of Medicine is a 3-year training program with approximately 166 residents per year (58 PGY-1, 57 PGY-2, and 51 PGY-3) covering American and international medical schools. It is one of the largest programs in the nation. The QI projects are conducted by teams of 8 to 10 residents (mix of PGY-1 to PGY-3) in a weekly continuity clinic under the guidance of faculty advisors, each with a PGY-2 team leader.
Evaluation and feedback
For year-end poster evaluation, expert QI leaders at Emory collectively developed a scoring rubric that evaluated projects on the presence of 4 QI elements: aim statements, data measures plotted on run charts, performance improvement tools, and system-level tests of change (Supplemental Materials). Though the launching of our curriculum preceded the publication of any validated survey instruments assessing resident QI knowledge (to the authors’ knowledge), the QI elements on our rubric reflect those described in the revised Quality Improvement Knowledge Application Tool (QIKAT-R), a validated and user-friendly instrument that relies on 3 subsections titled Aim, Measure, and Change. 21 Each of these elements are graded and averaged across the 4 categories, with 2 to 3 expert graders assigned to each poster.
The posters help to solidify resident knowledge of process improvement, provide feedback for longitudinal continuation of projects, and present their efforts to the larger university and hospital community. An example of a completed poster project receiving a high score is shown in Figure 2. To assess curriculum-generated improvements in processes of clinical care, we also tracked scholarly output of all QI projects for academic years 2007 to 2019.

Example of a completed resident project.
Results
Resident survey
Fifty-one PGY-1 residents (59%) and 50 PGY-2 and PGY-3 residents (46%) completed the pre- and postintervention survey, respectively. Prior to taking the course, the majority of residents (90.2%) either “agreed” or “strongly agreed” that core QI principles will likely be incorporated into their future practice. However, although the majority (82.3%) also initially indicated they either did not feel comfortable or felt neutral leading a QI project, our findings showed a trend of increasing comfort level after the course. The proportion of correct answers to the questions on objective QI knowledge also substantially improved, with differences in knowledge-based scores before and after the course ranging from 30% to 50%.
Resident projects
Average scores for projects in the first 5 years of the curriculum can be found under Supplemental Materials, showing an improvement in overall scores from 79.3% in 2007 to 87.5% in 2012. Though we lacked a robust system for tracking specific projects from 2007 to 2011, Table 2 depicts a list of project titles from 2011 to 2016. Projects commonly focused on specific themes, including screening, vaccination, and management of chronic diseases such as hypertension and diabetes. The number of projects per year dwindled after the first few years of the curriculum due to efforts to align projects with hospital priorities. As shown, there is a great diversity in the types of measures and outcomes to drive improvement, and all residents worked alongside nurses, medical assistants, and clinic schedulers in an interdisciplinary format for their tests of change.
Description of resident projects by year from 2011 to 2016.

Resulted in abstract and/or manuscript publication.
Resulted in system changes through protocol implementation.
Since 2007, the curriculum has involved more than 166 (100%) residents yearly, over 20 general medicine faculty and 136 year long team projects. All projects are presented as part of a conference at the end of the year, and selected projects are additionally presented at the School of Medicine research day and departmental grand rounds. Many projects achieved sustainment, especially around management of diabetes, hypertension, and advanced care documentation. Several involved cross-departmental specialty collaborations and/or resulted in system protocol changes (Supplemental Materials). Over 30 projects have also been presented as poster or oral presentations at regional and national conference meetings, and several have led to abstract and/or manuscript publications.22–27
Organizational outcomes
There were several measures of organizational change as an outcome of our course, including learner engagement in QI work, initiation of institutional QI roles, and implementation of faculty training (Figure 3). Given the longitudinal nature of our program, these changes evolved to reflect the dynamic organizational, environmental, and contextual influences present over its iterations.
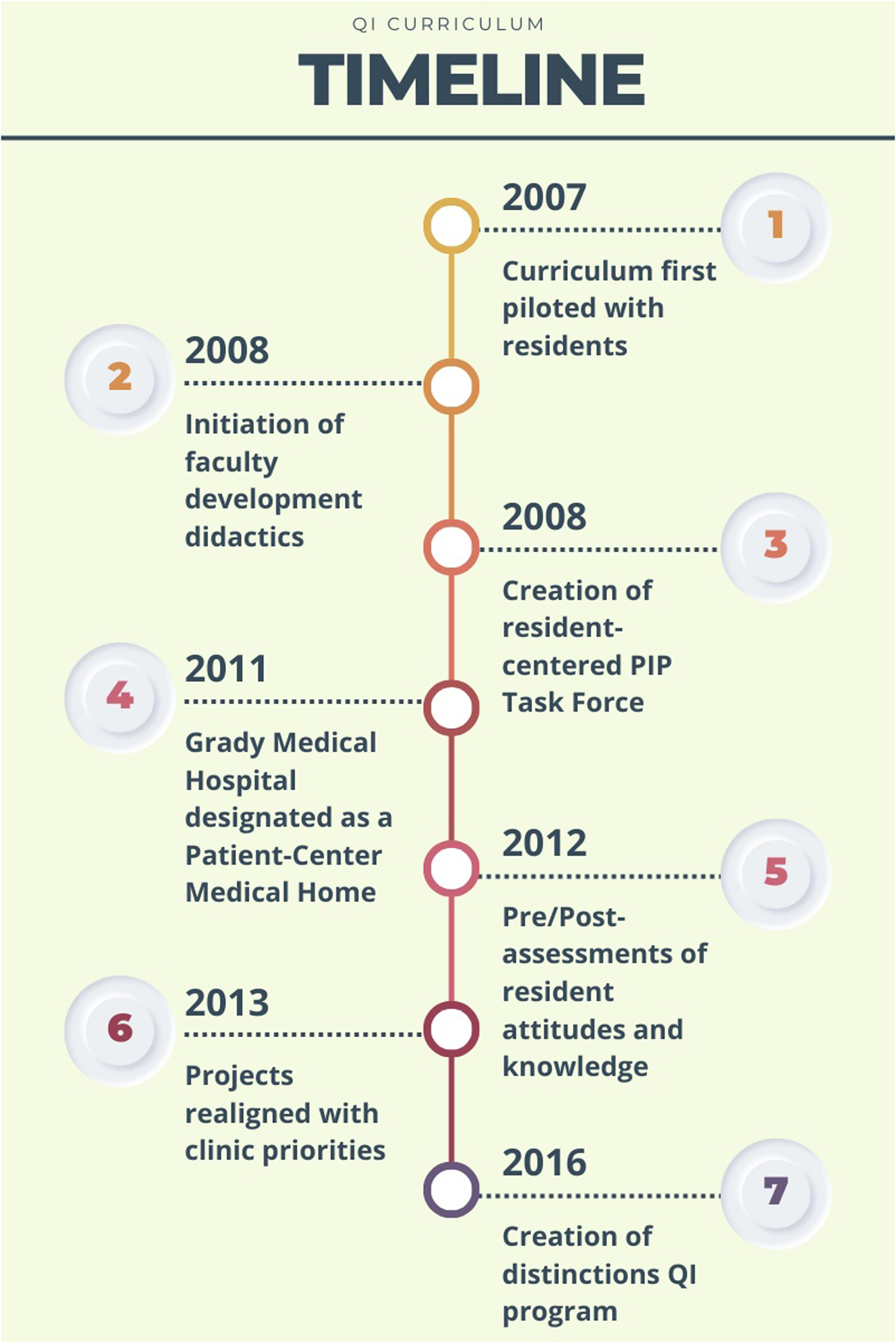
Timeline of program changes and stages in curriculum development.
In 2011, Primarcy Care Center of the GHS received designation as a Patient Center Medical Home (PCMH), drawing more concerted efforts to align resident projects with quality organization goals with Emory and Grady. This led to a redirection and consolidation of project focus that necessarily decreased their overall quantity, though we feel that attempting too many projects within a cohort also damaged the ability to bring projects to completion due to the substantial time and energy demands of real-life quality and safety interventions.
Furthermore, faculty mentors who precept in the clinic (mostly general medicine) received didactics in QI skills as part of faculty development to help guide residents. Upon initial curriculum implementation, faculty development was held as skills-focused weekly conferences, later transitioning to monthly meetings as needed. Mentors with expertise in knowledge and application of QI principles were available for additional guidance.
In addition, we initiated a resident Performance Improvement Project (PIP) Faculty Task Force. The PIP Task Force has historically consisted of one of the Chief Quality officers from Emory Healthcare, a PIP Curriculum Director from each clinic site, and the general medical faculty preceptors based in the clinics who agreed to serve as QI project facilitators. Our curriculum spurred the creation of a resident-centered task force, consisting of approximately 12 resident volunteers with an interest in QI, which made ongoing improvements to the curriculum based on resident feedback, faculty facilitator feedback, and clinic needs assessments. They provided longitudinal mentorship and QI expertise, including guidance regarding selection of projects and feasibility of scope, creation of QI project distinctions criteria, and achievement of project milestones.
Finally, given the sustainability of the curriculum, a formal distinctions program was developed in 2016 for residents interested in QI and Patient Safety. To receive this distinction, residents were required to have demonstrated excellent practical application of quality improvement skills in their year-end project, complete online modules in the IHI Open School's Basic Certificate in Quality and Safety, contribute meaningfully to QI scholarship and/or local initiatives, and participate in Resident Quality Committee activities. Approximately 3 to 5 residents per year have received this distinction since implementation.
Discussion
We describe a longitudinal quality improvement training curriculum embedded within the outpatient learning environment of a large American academic health system and associated Internal Medicine residency program. Our curriculum is distinct from similar published curricula at other institutions in its depiction of a large-scale, longitudinal innovation focusing on project-oriented outcomes and scholarly output, apart from simply self-reported or test-based postcourse knowledge assessments. In detailing the implementation, evolution, and sustainment of more than a decade of our curriculum, we demonstrate the several intentional changes made to further optimize from its initial incarnation with the hopes of aiding future attempts at replication in other institutions.
Selecting the resident continuity clinics as the site of our curriculum's implementation was crucial to its success and allowed the residents to focus on chronic care issues and participate in healthcare system redesign. The projects selected by residents ranged from evidence-based management of high-prevalence chronic illnesses like diabetes to preventive care like age-appropriate cancer screening. Although the 2 sites for the resident continuity clinics, Grady Memorial Hospital and Emory University Hospital, differ substantially in patient population, clinic resources, and access to information technology, our curriculum has been successfully sustained in both practices. The continuity of patient care and education within the resident clinics allows for a QI experience that is both longitudinal and team-based.
One advantage of our curriculum is the intense focus on patients who face social determinants of health. Prior studies have demonstrated that a lack of alignment between institutional priorities and resident-led projects can lead to fragmented QI efforts and learner disengagement. 28 Since the start of the curriculum, the residency program aligned projects with goals for the health system in the hope that projects would be sustainable, improve patient outcomes, and possibly drive health equity. As a result of the change in focus, projects were fewer but larger in scope, involving interdisciplinary teams of PCMH from 2013 to 2016.
Another advantage was the focus on appreciating interprofessional competencies and their relevance to implementing QI initiatives. Interdisciplinary team experience was embedded into the didactic curriculum by design, with all residents made aware that collaboration with Certified Nursing Assistants, front desk personnel, and other team members was not only encouraged but also constituted an essential part of the Model for Improvement.
Key lessons learned through developing this curriculum include the importance of quality leadership involvement and the creation of the PIP task force. This has generated useful feedback on the curriculum and helped facilitate didactic sessions. Additional lessons learned include the importance of setting clear goals, objectives, and deadlines for each educational session. Creating a forum for communicating about projects was also important, for which the IHI website 29 was particularly helpful. Lastly, to alleviate time pressures, we separated the didactic component of the curriculum into the core conference schedule, allowing for monthly 1-hr team meetings.
To our knowledge, we are one of the few large IM residency programs to implement a longitudinal continuity clinic-based QI curriculum, directly involving all residents in all levels of project design and implementation and driving toward improved patient outcomes in different settings.
Limitations/challenges
Our study is most limited by the fact that much of our data was originally collected for administrative purposes and retrospectively reviewed for analysis, and therefore suffers various discontinuities and heterogeneity that render it underpowered for statistical analysis. As stated, we present our descriptive data with the aim of informing future educators wishing to incorporate QI principles in their residency curriculum. As such, we frame this section as a set of recommended “best practices” in addressing various barriers to implementing QI educational programs at curricular and environmental levels.
Our 2012 to 2013 needs assessment survey was limited in its scope of knowledge and attitudes assessed, as well as the number of surveyed participants. Given the large program, we had lower resident response rates, and doing the survey yearly proved challenging. We also did not use a validated survey tool, which may bias the survey results. Evaluation of learner satisfaction, attitudes, and perceptions could have been supplemented through extraction of qualitative data through focus groups or interviews with participants. Our poster scoring system was also developed internally, and therefore had not been previously validated for accuracy or assessed for interrater reliability, though it does share key components of the validated QIKAT tool. Future iterations of the program may modify this grading rubric to incorporate prior recommended guidelines and evaluate interrater reliability.30,31
In addition, various institutional factors made locally implementing this work challenging in some respects. First, there was difficulty determining the optimal size for project teams. A smaller number of large teams lends itself to oversight by the curriculum leader, but limits individual engagement, whereas a larger number of small teams require greater direct resident involvement but increases the complexity of oversight. In our curriculum, project teams would range from 8 to 10 residents in size after adjusting for shared clinic days and locations. Secondly, though the variety in clinic locations and patient populations with which this curriculum was implemented remains a strength of our program, future research should aim to evaluate for differences in project quality or resident learning between different sites. In addition, although we would have liked to incorporate co-learning between residents and faculty, it was exceedingly difficult to find protected time that could accommodate both resident and faculty availabilities.
Finally, it was difficult to measure downstream effects of the QI curriculum on patient outcomes or clinical care, although projects were planned in accordance with institutional priorities and areas of focus. Measuring changes in clinical outcomes following educational interventions is a well-established challenge due to complexities in establishing true causality. It is notable that several projects evolved into published studies showing sustained positive impacts in the clinic, but we were unable to undertake system-level analyses of QI projects’ impact on clinical outcomes. Future research will look toward conducting qualitative interviews and/or focus groups with past participants to better assess whether the curriculum influenced their future practice behaviors or career path.
The large size of our residency program and continuity clinics located at 2 different hospital campuses pose logistical challenges related to dissemination across sites and tracking individual projects; it also requires salary support for the curriculum leader to ensure communication of timelines, enforcement of deadlines, and general preparation for each of the didactic sessions.
Conclusion
Our experience implementing a quality improvement curriculum based in a resident continuity clinic proved feasible and sustainable, with distinct advantages in allowing residents to participate longitudinally across several years of training with a focus on hands-on, project-driven engagement aligned with institutional priorities. In applying these lessons, residents learn how to measure adherence with current evidence-based medicine guidelines and develop interventions to maintain momentum within the reality of busy clinical practice. Our curriculum adds a new dimension to the existing literature by introducing multiple avenues for dynamic, real-time program development that can serve as a model for other training programs.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251320482 - Supplemental material for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program
Supplemental material, sj-docx-1-mde-10.1177_23821205251320482 for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program by Kain Kim, Bhavin Adhyaru, Joyce Doyle, Jada Bussey-Jones, Danielle Jones, Lorenzo DiFrancesco, Shelly Ann Fluker, Richard Gitomer and Nurcan Ilksoy in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251320482 - Supplemental material for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program
Supplemental material, sj-docx-2-mde-10.1177_23821205251320482 for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program by Kain Kim, Bhavin Adhyaru, Joyce Doyle, Jada Bussey-Jones, Danielle Jones, Lorenzo DiFrancesco, Shelly Ann Fluker, Richard Gitomer and Nurcan Ilksoy in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205251320482 - Supplemental material for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program
Supplemental material, sj-pdf-3-mde-10.1177_23821205251320482 for Developing and Implementing a Quality Improvement Curriculum in a Large Internal Medicine Residency Program by Kain Kim, Bhavin Adhyaru, Joyce Doyle, Jada Bussey-Jones, Danielle Jones, Lorenzo DiFrancesco, Shelly Ann Fluker, Richard Gitomer and Nurcan Ilksoy in Journal of Medical Education and Curricular Development
Footnotes
Authors’ Contribution
All authors contributed to writing the original draft of the manuscript. NI, JD, and RG helped lead the curriculum. LD served as program director of the curriculum. JB and DJ assisted with development of the curriculum. BA assisted with conceptualization of the manuscript and critical revision of the work.
Consent
Informed consent was obtained from participants and residents participated as part of the internal medicine resident curriculum.
Declaration of Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
For this study, Emory Institution Review Board (IRB) exemption was received as a quality improvement initiative. All data used in the study was anonymized.
Funding
This curriculum initially was funded by an internal educational grant through Emory Healthcare (2006-2008). Currently it is supported by Emory University Department of Medicine.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.