
Abstract
OBJECTIVES
One of the major contributing factors to the opioid crisis, marked by a surge in opioid prescriptions, includes inadequate adherence to guideline-based pain management practices, highlighting the need for a comprehensive curriculum during residency training. In this study, we aim to assess opioid exposure prevalence among hospitalized patients and examine potential associations between disease conditions, patient demographics, and opioid prescriptions during their hospital stay.
METHODS
In this retrospective cohort study at a southern California county teaching hospital, we analyzed the medical records of 2272 patients admitted to the IM resident inpatient teaching service for 1 year, from September 2017 through September 2018.
RESULTS
The study found that 44% of patients received opioid prescriptions during their hospital admission, with 23% receiving prescriptions at discharge and 45% having prior opioid exposure. Patients with prehospital opioid exposure had a 2-fold increased risk at discharge (Relative Risk: 2.51; P < .0001). The hypothesis that factors such as gender, certain medical conditions, and previous opioid use influenced opioid prescriptions during hospitalization is disproved. Instead, hospital admission itself was the significant contributing factor to receiving opioids during acute care and at discharge, irrespective of the source of pain.
CONCLUSION
In conclusion, our study revealed that the primary determinant for opioid exposure during hospitalization is the inpatient admission itself rather than specific patient-related factors. The lack of a structured curriculum in residency training contributes to the default use of opioids for all pain types, highlighting the need for curricular reforms to focus on multimodal pain management principles.
Keywords
Introduction
The prevalence of opioid use in the United States, both therapeutic and recreational, has dramatically increased over the past decade, with drug overdose deaths nearly tripling from 1999 to 2014. 1 Prescription and recreational use of opioids are responsible for the highest drug overdose mortality rates ever recorded. 2 Despite policy and health system changes to curb the epidemic and legislative changes increasing access to naloxone, age-adjusted opioid-involved death rates continue to climb. 3 According to the Centers for Disease Control (CDC), in 2016, around 28% of the U.S. adult population sought medication for chronic pain. 4
The opioid crisis continues unabated for many reasons. One of the main contributing factors is the opioid prescribing practice by physicians without consideration of a more comprehensive, multimodal approach to pain management (including nonpharmacologic therapy and nonopioid pharmacologic options) and not having shared decision-making with their patients when they need to prescribe opioids. There is now ample evidence to suggest that a majority of chronic opioid-dependent patients had their initial exposure to opioids through a prescription (Figure 1) by a healthcare provider. 5 In October 2017, the Federal Response to the Opioid Crisis focused on 2 key factors that contributed to the crisis: increasing opioid analgesic prescriptions and inadequate training for healthcare providers to prescribe opioids safely. 6 A study by Phinn et al found that, of the opioid-naive patients who were prescribed opioids on admission and discharge, approximately one-third of them did not have indications for opioids and were at risk for long-term opioid use. 7

Demonstrates the role of acute pain prescribing as a contributor to the opioid use disorder cycle in vulnerable populations. It is reprinted with permission from Am J Drug Alcohol Abuse. 2015 Nov; 41(6): 508-518. doi:10.3109/00952990.2015.1043435. PMID: 25982491 Dynamic Model of Nonmedical Opioid Use Trajectories and Potential Policy Interventions; Wayne Wakeland, Alexandra Nielsen, and Peter Geissert.
Objective
Most residency training programs in Internal Medicine (IM) and other primary care specialties do not include a structured (not hidden) curriculum to teach a multimodal approach to pain management. The residency program (Categorical IM) studied here and other specialty Graduate Medical Education (GME) programs in this sponsoring institution had neither any orientation training before starting residency nor a structured curriculum in pain management during the training. Our objective was to measure the prevalence of opioid exposure in hospitalized patients and identify any patterns of disease-based association or patient-specific demographic attributes that resulted in opioid prescriptions during their hospitalization. Risk factors for opioid misuse or addiction include past or current substance abuse, untreated psychiatric disorders, younger age, and social or family environments that encourage misuse. 8
Our initial hypothesis was that specific patient attributes and risk factors could predict opioid usage during hospitalization, as could their primary admitting diagnosis. We aimed to investigate whether factors like prior opioid use (prescription or recreational) and comorbid conditions such as mood disorders (specifically anxiety and depression) 9 or chronic pain was associated with an increased likelihood of receiving opioids in the hospital, even when some admission diagnoses (eg, heart failure, altered mental status, acute kidney injury) didn't warrant opioids per current guidelines.10–12
Methods
Ethical approval and consent
The Kern Medical IRB approved the study (#17086) in September 2017. Due to its retrospective nature, the IRB waived the need for informed consent. The study followed the Declaration of Helsinki and the Federal Law of Human Research.
Data source
A comprehensive analysis was conducted in this retrospective cohort study at a county teaching hospital in southern California. Data was extracted from the electronic medical record (EMR) of 2272 patients admitted to the IM resident teaching hospitalist teams from September 2017 through September 2018 (Figure 2). To reduce selection bias, we included all hospitalized patients in the internal medicine teaching service with broad inclusion criteria. We exclusively utilized EMR notes without relying on subjective or survey data to account for potential recall or observer bias. The dataset was meticulously curated to include patient demographics, past medical history of comorbid conditions, information regarding prior prescription and recreational opioid use, opioids prescribed during the hospitalization, documented admission diagnosis, other medical conditions necessitating opioid prescriptions, and details of opioids prescribed at discharge. Based on the documentation in EMR orders and assessment plan notes, indications for opioids ordered during hospitalization and discharge prescriptions were grouped under the 5 pain categories: inflammatory (includes postoperative), neuropathic, somatic, headache, and musculoskeletal injuries (includes bone fractures). When there was no apparent indication for the opioids prescribed, they were labeled as “Uncategorized.” We utilized the STROBE cohort checklist when writing our report.13,14
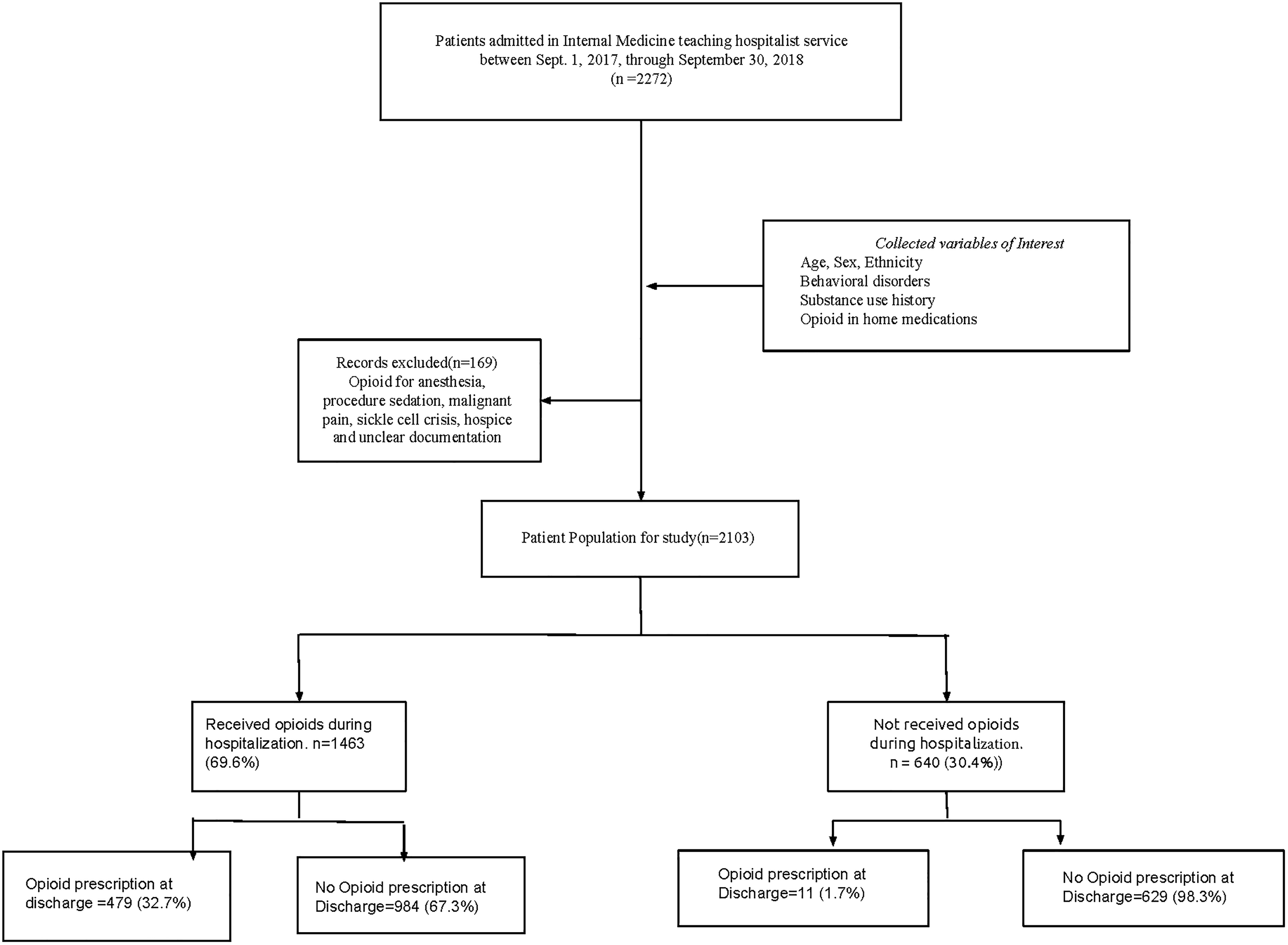
Methods flow chart.
Inclusion and exclusion criteria
For this study, an “admission” was defined as a medical assessment and management decision conducted by an IM resident under the supervision of the hospitalist attending (Figure 2). Patients who received care exclusively within the IM in-patient wards were considered eligible for inclusion, while those transferred to other specialty services were excluded. Additionally, patients who received opioids for sickle cell crisis, procedural sedation, anesthesia, hospice care, and cancer-related pain were also excluded from the study. In the interest of reviewing the findings against the current guidelines10–12 for pain management, we included patients with postoperative pain, musculoskeletal injuries (including bone fractures), and patients with a history of opioid use disorder (OUD). Some patient charts with difficulty collecting the data on the covariates of interest due to documentation inaccuracies were excluded.
Outcome assessment
Covariates of interest
Demographic variables—age, gender, ethnicity
Comorbid conditions—Back pain, anxiety, depression
History of opioid use before this hospital admission (includes prescription and recreational drug use, prior exposure defined as use mentioned in the past, and social history sections of the admission notes; the duration of use before this admission is unclear from the documented notes). These covariates were crucial in understanding how patient-related factors influenced opioid administration during hospitalization.
Tables with details are attached in Appendix 1 in the supplement material to the article.
Statistical analysis
To evaluate disparities in patient demographics associated with opioid prescriptions, we employed the Pearson Chi-square test as our statistical analysis tool. This rigorous analysis was conducted using SPSS version 22, a software platform developed by IBM Corp. in Armonk, New York, known for its robust capabilities in statistical analysis. Qualitative variables were summarized using frequency and percentages, while quantitative variables were summarized using mean and standard deviation. Associations and relationships between the variables were analyzed using an unpaired t-test, Chi-square test, and Fisher's exact test, depending on the data distribution. The prevalence of each outcome variable was reported using percent and 95% confidence intervals. Univariate and multivariable relative risk (RR) regression was conducted to review the outcome variables of interest (“Prescribed opioids during this admission” and “Opioids prescribed at discharge”). RR, 95% confidence interval, and P-values were used to describe the relationship. A univariate multinomial logistic regression was conducted to analyze “Number of days in the hospital,” “Number of pills,” and “Number of days on opioids.” Multivariable analysis was conducted using a backward stepwise selection process considering variables with a significance of 15% for entry and 5% (statistically significant) to stay in the final model. All analyses were conducted using Stata V.15.
Results from the statistical analysis are provided in tables in Appendix 2.
Results
Among 2272 patients treated on the IM resident teaching hospitalist service, 2103 met the inclusion criteria. One thousand four hundred sixty-three (69.6%) patients received opioids during their hospitalization, of which 479 (32.7%) patients also received a discharge opioid prescription, and 984 (67.3%) patients were discharged without an opioid prescription. Of the 640 (30.4%) patients who did not receive opioids while they were admitted, 11 (1.7%) received an opioid prescription on discharge, and 629 (98.3%) patients were discharged without an opioid prescription. Our study variables were collected without missing data for each patient in the final analysis. Per the statistician consult, while the Forest plot depiction is traditionally used in a meta-analysis comparing studies, it can be adapted as a valuable tool for studying multivariable analysis, summarizing the observed effect size, and having a graphical depiction of the effect. 15 The results are also depicted as bar and pie charts in Appendix 3.
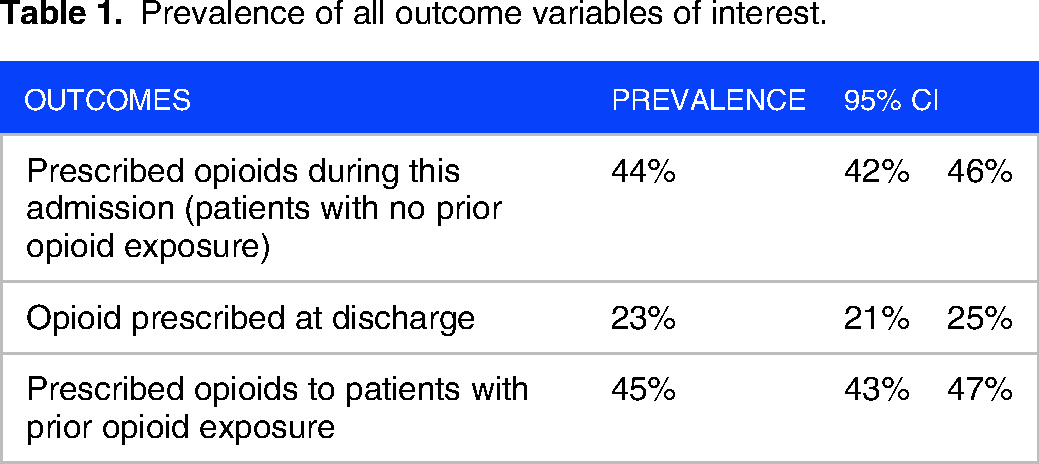
As shown in Table 1, overall, patients prescribed opioids during their current admission had a prevalence of 44% (95% CI [42%-46%]), opioids prescribed at discharge had a prevalence of 23% (95% CI [21%-25%]), and those who had been exposed to opioids before admission had a prevalence of 45% (95% CI [43%-47%]).
Prevalence of all outcome variables of interest.
The findings from Forest Plot 1 (Figure 3) analyze factors influencing opioid prescriptions during admission. Patients admitted for medical conditions comprising inflammatory pain, somatic pain, headache disorder, and musculoskeletal injuries (including bone fractures) showed a statistically significant increase in the risk of being prescribed opioids. This points to a notable pattern in which patients are routinely given opioids at the time of admission, regardless of the specific type of pain they are experiencing. The uniformity in the prescription of opioids points to a possible area for more research into the variables impacting the prescribing practices during the admission process across a range of pain presentations.

Forest plot 1.
Table 2 examines the RR of opioid prescriptions at discharge. It revealed that patients were at a higher risk of being prescribed opioids regardless of the etiology of pain. Patients who had prior exposure to opioids before their hospital admission, including both prescribed opioids and recreational drug use, exhibited a significant 2-fold increase in the risk of receiving opioid prescriptions at discharge, as indicated by an RR of 2.51 (P < .0001). Similarly, those who were prescribed opioids at the time of admission had a 2-fold increase in absolute risk for subsequent opioid prescription at discharge, with an RR of 2.48 (P < .0001). These findings underline the significant impact of prehospital opioid exposure and admission opioid prescriptions on the OUD cycle (Figure 1), multiplying the risk for long-term opioid usage by patients. 5
Multivariable relative risk regression of opioids prescribed at discharge.

The Forest Plot 2 (Figure 4) analysis provides findings on factors influencing opioid prescription at discharge. The patient's demographic attributes, such as age, gender, or ethnicity, did not seem to affect the physician's choice of opioids versus other medications for managing pain in the in-patient setting. The duration of opioid medication during hospitalization may have influenced discharge opioid prescriptions as patients on opioids for 4 to 6 days show a statistically significant increased risk of opioid prescription at discharge (RR: 2.49, 95% CI [2.04-3.04]), while those on opioids for ≥7 days exhibit a similar increased risk (RR: 2.48, 95% CI [1.95-3.17]). It is also seen that patients prescribed opioids during their hospital admission are notably more likely to receive opioid prescriptions at discharge, with an RR of 2.1 (95% CI [1.75-2.52]). Additionally, individuals with prehospital opioid exposure had a higher risk for opioid prescription at discharge, with an RR of 1.61 (95% CI [1.34-1.92]). According to the guidelines,10,12,16 patients under the pain categories studied here should have received (multi-modal-analgesia [MMA] using a combination of other nonpharmacologic therapies or nonopioid pharmacologic therapies. Still, the majority of the discharged patients were prescribed opioids without any documentation of a decision pathway to differentiate based on the etiology/type of pain categories. Hence, the group “Uncategorized” received about one-fourth of all opioid prescriptions given at discharge (Figure 5).

Forest plot 2.

Association of variables with opioids prescribed at discharge versus etiologic category of pain.
Discussion
Summary of the findings
The primary objective of this study was to rigorously examine whether the hospitalized patients’ specific demographic attributes, preexisting comorbidities, or previous opioid exposure made them more likely to receive opioids during acute care and at discharge. To our surprise, the single most significant determinant for opioid exposure during acute care is the event of hospitalization itself, rather than any specific patient attribute, demographic, or diagnosis. Given the diverse nature of our population across multiple demographics and comorbidities, the fact that hospitalization alone served as the dominant risk factor for opioid prescription highlights the generalizability of our study. As illustrated in Table 2, Figures 4 and 5 results, the neuropathic and headache categories had lower percentages of discharge opiates. They had no significant association or increased risk for discharge opiates since the P-values were .07 and .4, respectively. However, the majority of patients admitted to the inpatient team received opioids as a part of their treatment plan, irrespective of their principal diagnoses and other medical comorbidities. EMR data showed that opiates were prescribed in bundled admission order sets for patients with primary diagnoses (eg, heart failure, diabetic ketoacidosis) when pain was not even a symptom of the clinical syndrome. There was no documentation of shared decision-making with the patients who were prescribed opioids. The indications noted in the discharge opioid prescriptions and the discharge summary documentation showed a universal choice of opioids for all pain categories, leading to the assumption that MMA was not discussed or prescribed. Even for pain categories such as postoperative and bone fractures, guidelines note the high level of evidence recommending MMA for managing acute, high-intensity pain. 10 The guidelines recommend the routine use of a combination of NSAIDs, regional nerve blocks, topical analgesia, and cryotherapy as part of a comprehensive analgesic plan for both operative and nonoperative care of bone fractures. In the situation of the inevitable need to use opioids, like contraindications to the use of NSAIDs, and when pain severity limits a patient's recovery and progressive mobility, patient comfort and safety must be carefully balanced while prescribing opioids. The literature is scarce in evidence for the safety and efficacy of opiates in treating patients with postoperative pain and acute musculoskeletal injuries. 16 Hence, the appropriate type (immediate release vs extended release), route (oral vs intravenous), and dose of opiates for specific injuries or conditions are not well defined. Standard prescribing habits seem to provide an excess amount of medication routinely and prolong the use of intravenous opioids in the acute care setting. Because of the potential for misuse of all opioids, the Orthopaedic Trauma Association (OTA) Musculoskeletal Pain Task Force recommends that the prescriber should use the lowest effective dose for the shortest period possible (strong recommendation, high-quality evidence). 16 The OTA panel recommends the use of MMA as opposed to opioid monotherapy for pain control (strong recommendation, moderate-quality evidence). In the retrospective review of the assessment and plan notes for these charts, there was no documentation of any decision pathways or the use of MMA, and quite often, the default orders of intravenous and oral opioids from the admission order sets were continued through the day of discharge.
Limitations
We acknowledge several limitations of our study. First, due to being a single county hospital system, one specialty (IM) residency program, and data collected over 1 year, our sample size was a relatively small patient group after exclusions. Due to the retrospective nature of the study, we could not accurately assess if any resources (at the time of data collection, relatively few clinical practice guidelines were available for the use of opioids in the acute inpatient setting outside of postoperative pain management and palliative care) 12 were used by the residency program at the time of opioid prescribing. As a retrospective study, the subjective nature of documentation in assessment and plan notes also led to difficulties deciphering the rationale behind medical decision-making. Opioid prescribing patterns were challenging to track in terms of the duration and the total number of opioids received by patients while inpatient and upon discharge (given that the study was based on retrospective data gathered from EMR orders and assessment-plan notes rather than medications actually received by the patients). We acknowledge that the above-stated limitations impact the study's validity and the measured outcomes’ reliability. It warrants the need for a multicenter prospective study to measure the impact of the current guidelines and legal mandates that came into effect after this study. Within these limitations, the findings and discussions satisfactorily demonstrate our study's overall goal to emphasize the need for a structured longitudinal GME curriculum.
Recommendations for structured curriculum on pain management in GME
To regulate inappropriate opioid prescribing, multiple strategies need to be implemented simultaneously, such as policies and guidelines targeted at prescribers, curricular improvement in physicians’ and allied health professionals’ education, implementation of state-level prescription drug monitoring programs, and lowering the default opioid dose in EMR. 17 Physician overprescription is one factor that can be partially mitigated by medical education and training.
Despite the apparent importance of effective pain management, physician comfort and knowledge in this area are surprisingly low.18–21 Since the completion of our study and data collection, there has been significant national interest in medical education and healthcare providers’ training in pain management with a focus on MMA. Since June 2023, there has been a federal requirement for any Drug Enforcement Administration (DEA) registered physician to undergo 8 hr of training in the treatment and management of opioid and other substance use disorders as part of the Medication Access and Training Expansion (MATE) Act. 22 However, it is unfortunate but noteworthy that the DEA registrant training is not required for GME trainees as they operate under the DEA registration of a hospital/clinic pursuant to United States Bill 21 CFR 1301.22(c). 23 As a new mandate, further scrutiny is needed to determine whether completing the training modules led to changes in prescribing patterns or improved physicians’ competence in this area. Despite the legal requirements, as well as the removal of barriers to medication-assisted therapy (MAT) for OUD, it remains unclear if acute care physicians not board-certified in addiction medicine are prescribing MAT to patients in need.
The results of this study reveal the need for a structured (not hidden) GME curriculum on the principles and practice of pain management and to consider MMA as an opioid stewardship 24 effort to manage acute pain. Among medical schools and residency programs, the incorporation of an opioid stewardship curriculum that provides education and training related to opioid overdose prevention, education, and naloxone prescribing has ultimately increased naloxone prescribing practice by physicians. 24 While few medical schools and residency programs deliver such curricula, its inclusion has improved knowledge and confidence in managing pain. 18
As one of the fundamental competencies of hospital medicine, attending physicians and resident house staff should be proficient in acute pain management. 11 Residents and fellows often prescribe opioids without receiving proper education on safe prescribing practices. Residents in GME programs frequently feel a lack of confidence in managing pain due to inadequate training.25–27 One reason could be that palliative care and pain management are not adequately represented in core curricula at both the undergraduate and postgraduate levels. Despite the implementation of many opioid-related federal policies, as well as mandated opioid prescribing education for healthcare professionals in several states, residents and fellows in GME are overlooked as opioid prescribers and miss out on such training.23,27 In a previous survey designed by Chaitowitz to analyze residents’ prescribing attitudes, results suggested that practical competence was low, even with fundamental opioid prescription concepts. Knowledge of dosage, duration of action, and drug equivalence in opioid prescription was lacking, consistent with previous studies.27–29 Inadequate education resulted in using opioids exclusively for initial pain management instead of MMA. Education can empower residents to make appropriate decisions about the initiation, continuation, modification, or discontinuation of opioid treatment for each patient at each clinical encounter. 21
The Flexner model of medical education and residency training aspires for the resident trainee to emerge as a competent professional capable of independent, unsupervised practice through training methods that fundamentally exist in a craft/trade/guild construct. While there has been some refinement of the training standards in GME over the past century, a comprehensive curriculum and standardized pathway to assuring competency does not exist, and trainee assessments do not correlate to patient care outcomes. 30 There is current consensus and momentum to develop and evolve Competency-Based Medical Education.31,32 The knowledge and skills in the pain management domain are not assessed or evaluated as a required core competency expected from the trainee. In contrast, it should be considered an equally important competency akin to glycemic control or antibiotic stewardship. The adequate management of pain and judicious use of opioid medication are vital concepts to be introduced as early as the initial few months of the internship, with progressive advancement of skill level in this competency over the entire residency training as a longitudinal curriculum. In an observational study by Raheemullah et al, a 16-week educational curriculum was incorporated into existing residency didactics and a protocol based on CDC guidelines, demonstrating that increasing resident competence in managing chronic pain and opioid use disorder is feasible. This educational intervention and guideline-based protocol improved resident confidence in opioid prescribing practices along with detecting and managing addiction. 18 Although state medical boards have eased regulations to allow inpatient providers to prescribe MAT for managing acute pain in patients with a history of OUD, GME trainees are often not taught or guided to offer these to patients who desperately need them.
There is currently no structured curriculum in residency training to teach the principles and practice of a multimodal approach to pain management. The hidden curriculum 33 is prevalent in GME, assuming that the resident's knowledge and skills for pain management practice are acquired by observing the senior residents and the attending physicians’ discussions during patient rounds. In addition, residents often prescribe opioids by default due to the existing norms, 33 such as avoiding being reprimanded by supervising attendings and hospital administrators who are concerned about patient satisfaction scores. 27 Hence, residents who are untrained and not confident with MMA tend to order opioids as the default drug of choice to treat all types of pain in all hospitalized patients without any discretion, decision pathways, or shared decision-making with patients. The EMR, instead of enabling physicians to improve the quality and safety of patient care, facilitates a perilous path to harm through prechecked order sets that often include intravenous opioids as the standard as-needed option for pain treatment.
Pain management principles and practice skills should be integral to undergraduate and postgraduate training curricula. It should be taught in several sessions with a combination of structured didactic format, asynchronous modules, and case-based problem-solving team approach with reinforcement during bedside teachable moments. The residency training curriculum should include the multimodal approach to pain management with case-based examples. Interns early in their training should practice role-play scenarios to acquire the necessary skills, such as shared decision-making with patients when there is an inevitable need to order opioids, the use of opioid risk assessment tools, counseling patients about medication adverse effects, and offering guidance to taper and wean opioids over time. Resident and fellow evaluations should include an assessment of their competency to manage pain safely and adequately for their patients, especially now that there are standardized asynchronous modules (American Medical Association, New England Journal of Medicine Knowledge Plus, and American College of Physicians, to name a few high-quality resources) available in this area to help physicians comply with the MATE Act.22,34,35
Conclusion
The opioid use epidemic in the United States is an enormous and complex problem with multifactorial causes, some of which include social determinants of health, the business model of healthcare delivery, the lack of effective public health policies, and much more. However, the scope of this study is to highlight the role GME trainees play in contributing to the patient's initial opioid exposure and the potential subsequent long-term dependence as a result of that avoidable exposure. The GME trainees and supervising physician educators can have a notable, positive impact on patients’ outcomes by consistently using pain management guidelines, championing MMA, opioid stewardship, and shared decision-making with patients. The structured GME curriculum should align with the emerging competency-based assessment of the trainee milestones and rotation evaluations for competency levels achieved in this domain (pain management), with timely and periodic feedback based on patient outcomes.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241298353 - Supplemental material for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program
Supplemental material, sj-docx-1-mde-10.1177_23821205241298353 for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program by Sudhagar Thangarasu, Gowri Renganathan, Barney Soskin, Lela Ruck, Vishakh Prakash, Sumedha Unnikrishnan, Jyothsna Goranti and Everardo Cobos in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241298353 - Supplemental material for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program
Supplemental material, sj-docx-2-mde-10.1177_23821205241298353 for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program by Sudhagar Thangarasu, Gowri Renganathan, Barney Soskin, Lela Ruck, Vishakh Prakash, Sumedha Unnikrishnan, Jyothsna Goranti and Everardo Cobos in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241298353 - Supplemental material for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program
Supplemental material, sj-docx-3-mde-10.1177_23821205241298353 for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program by Sudhagar Thangarasu, Gowri Renganathan, Barney Soskin, Lela Ruck, Vishakh Prakash, Sumedha Unnikrishnan, Jyothsna Goranti and Everardo Cobos in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-4-mde-10.1177_23821205241298353 - Supplemental material for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program
Supplemental material, sj-pdf-4-mde-10.1177_23821205241298353 for Need for Structured Pain Management Curriculum and Competency-Based Evaluation in GME: An Observational Study in One Internal Medicine Residency Program by Sudhagar Thangarasu, Gowri Renganathan, Barney Soskin, Lela Ruck, Vishakh Prakash, Sumedha Unnikrishnan, Jyothsna Goranti and Everardo Cobos in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgment
We thank Dr Alok Dwivedi for his contributions through statistical analysis and the results tables.
Authors’ contributions
Study design, data collection, and interpretation: Thangarasu, S., Renganathan, G., and Cobos, E; statistical analysis and results interpretation: Thangarasu, S.; and acknowledgment to statistician—Alok Dwivedi, PhD.
Consent statement
Due to the study's retrospective design, the IRB waived the need for informed consent.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
The study followed the Declaration of Helsinki and the Federal Law of Human Research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.