
Abstract
INTRODUCTION
The Joint United Nations Program on HIV/AIDS (UNAIDS) has set a goal to eliminate AIDS as a public health threat by 2030 and the World Health Organization emphasized pre-exposure prophylaxis (PrEP) as a crucial element. Despite the lack of a specific role for general practitioners (GPs) in PrEP care, GPs could play a crucial role in the follow-up but this is still uncommon. Above, GPs estimate their knowledge about PrEP as low.
OBJECTIVES
This study seeks to understand the knowledge of GPs regarding PrEP care. Through online e-learning, we aimed to enhance our knowledge of PrEP care.
METHODS
Firstly, we assessed general knowledge about the PrEP of GPs. Secondly, we investigated the impact of e-learning on knowledge of PrEP care among GPs. We developed a multiple-choice questionnaire to evaluate self-assessed knowledge and knowledge about PrEP. One group of participants completed an e-learning module and took a pre- and post-test to assess changes in knowledge. Another group completed the questionnaire without e-learning.
RESULTS
Seventy-two participants completed the survey. Finally, 18 participants successfully completed the e-learning module. Nineteen percent (n = 14) of all GPs considered their general knowledge of PrEP to be “good,” while 68% (n = 49) of the GPs felt confident in identifying patients at risk, rating their ability as “good.” Participants achieved an average score of 4.7 (test group) and 4.6 (e-learning group) out of 10 on the knowledge test. After completion of the e-learning, the overall average score of the e-learning group significantly increased by 33% (p-value < .03).
CONCLUSIONS
GP generally scored low on knowledge covering different aspects of PrEP. However, after completing an e-learning module, there was a significant increase in the average test scores. These findings highlight the potential efficacy of targeted educational interventions in enhancing the understanding of PrEP among GPs.
Introduction
The Joint United Nations Program on HIV/AIDS (UNAIDS) has set a goal to eliminate AIDS as a public health threat by 2030, aligning with the Sustainable Development Goals. In 2021, UNAIDS developed a new global strategy to reinforce efforts toward the 2030 goal. 1 Both strategies emphasize the use of pre-exposure prophylaxis (PrEP) as a preventive tool to reduce HIV infections.1,2 The World Health Organization (WHO) initially recommended the use of antiretroviral medication for HIV prevention in 2012. 3 Subsequent recommendations from the European Centre for Disease Prevention and Control in 2015 and WHO in 2016 emphasized PrEP as a crucial element in broad prevention policies, specifically targeting men who have sex with men (MSM) and all individuals at substantial risk of HIV infection.4,5 In Belgium, there were 781 new HIV cases diagnosed in 2021, resulting in an infection rate of 6.7 per 100,000—an increase of 4.3% in comparison with the previous year. 6 Despite this increase, the number of new diagnoses is significantly lower than in previous years (−17% compared to 2019). Belgium still maintains relatively high infection rates compared to the European average of 4.3 new infections per 100,000. 7 Primary prevention remains a persistent focus in efforts to meet the Sustainable Development Goals (SDG) deadline. 8
PrEP involves a combination of 2 antiretroviral drugs, tenofovir disoproxil fumarate and emtricitabine, which can be taken either on a daily basis or in an event-driven manner, to reduce the risk of HIV infection.9–12 Studies have shown a reduction in HIV incidence of up to 86%, highlighting its feasibility within the European healthcare system.12,13 PrEP demonstrated its feasibility in Belgium through the Be-PrEP-ared study, leading to its integration into the healthcare system in June 2017. 14 From then until the end of 2019, 4071 individuals initiated PrEP treatment. 15 In 2021, 1866 people started treatment, accounting for 35% of the total number of users. 6 The vast majority, 99%, were men (96% MSM in 2020), and usage was most prevalent among individuals aged 30 to 39 (35%).6,16
Belgium offers PrEP through 12 HIV Reference Centers (HRC). The current criteria for MSM include engaging in condomless anal intercourse with at least 2 partners in the last 6 months, multiple instances of post-exposure prophylaxis use, multiple episodes of sexually transmitted infections (STIs) in the past 12 months, or the use of drugs during intercourse. Yearly reimbursement requires at least one annual PrEP-related visit to a certified HRC. 17
Despite the lack of a specific role for general practitioners (GP) in PrEP care (GPs cannot initiate or prescribe the treatment), there exists significant potential in the GP–patient relationship. This relationship could help identify more eligible MSM with a high-risk profile, give accurate information, and make PrEP easily accessible. GPs could play a crucial role in addressing individuals with poor self-assessment of HIV risk, which leads to lower awareness, acceptability, and uptake of PrEP. 18 Recent studies by Buffel et al 18 revealed that 1 out of 3 MSM in Belgium is eligible for PrEP use. Of those eligible, 62.6% were willing to take PrEP, but only 30.7% were actually using it at the time of the survey. This gap between willingness and actual usage emphasizes the need to reduce healthcare-related and structural barriers to PrEP use. 18 GP offices, being more accessible than predominantly urban HIV resource centers and offering potentially lower costs, could enhance PrEP uptake in this stage of PrEP care. 19 With current reimbursement requirements, follow-up visits, and prescription refills can theoretically be provided by GPs, but in the current situation, this is still uncommon. 7 It is important to note that GPs rated themselves low regarding their knowledge of following PrEP users. 20 This study seeks to delve deeper into the knowledge of GPs regarding PrEP. Through online e-learning methods, we aim to explore the potential for an enhancement in knowledge related to HIV prevention and PrEP.
Methods
Study objectives
Firstly, assess the self-assessed and general knowledge of PrEP of GPs. The primary outcome measure focused on the participants’ scores in a test evaluating knowledge of PrEP. Secondly, we investigated whether e-learning serves as an effective method to enhance the knowledge of PrEP among GPs. For the first group, the knowledge test score was evaluated without the engagement of an e-learning module. For the second group of participants, we assessed test scores and the impact of completing an online e-learning module.
Socio-demographic information, including years of experience, the number of HIV-positive patients treated, current experience with PrEP care, and participants’ self-assessed knowledge of PrEP were the independent variables with influence on the knowledge and the effect of the e-learning.
Population
We included Dutch-speaking GPs and GPs in training. The online survey and e-learning were conducted between March and June 2023. A request for participation was distributed by email through GP organizations and networks, both regional and national.
Design
Drawing on prior research, a literature review, and collaboration with HIV and educational experts, we developed a multiple-choice questionnaire to gather information on participants’ socio-demographic characteristics, self-assessed knowledge, and knowledge about PrEP. The participants’ knowledge was assessed through 10 questions covering various aspects of PrEP care, such as pharmacological considerations, usage, side effects, and initiation and cessation of PrEP (Table 1). The online surveys were administered using Qualtrics KU Leuven.
Ten questions addressing the knowledge of pre-exposure prophylaxis (PrEP)-care of the participants.
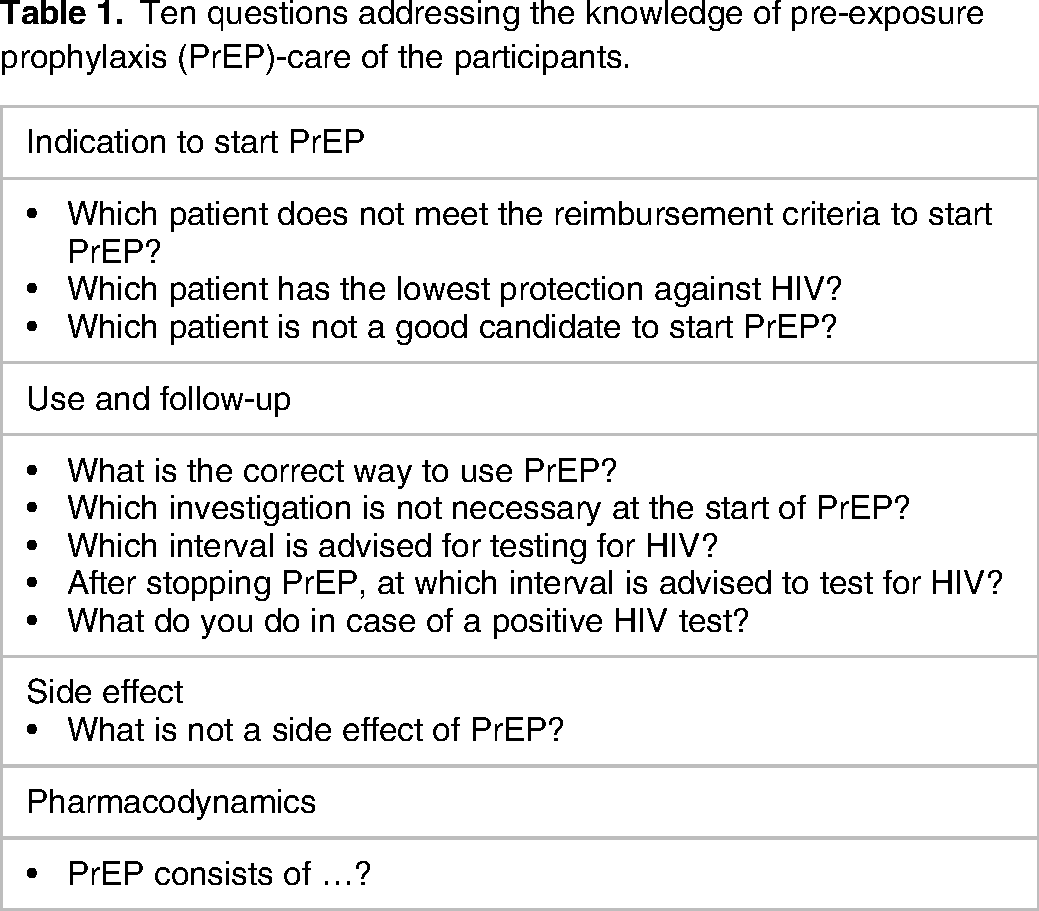
Both groups completed the self-assessed knowledge and knowledge survey, which ended up with an invitation to sign up for the e-learning. One group of participants completed an e-learning module on the latest PrEP guidelines (group A). This e-learning was developed in collaboration with an HIV expert and was based on the most recent WHO, Dutch, and Belgian guidelines of 2023 concerning PrEP. We utilized the online educational platform SOFIA (Published by ACCO) to facilitate the e-learning process. The e-learning is presented as an interactive module with case-based exercises, images, feedback, and a library with background information. After completing the e-learning module, participants were asked to revisit the knowledge test to assess changes in knowledge about PrEP care. A second group did not sign up for the e-learning and therefore only completed the self-assessed knowledge and the knowledge test (group B).
Statistical analysis
We employed a descriptive analysis for the survey data and utilized uni- and bivariate analyses for all collected data. We compared knowledge scores between both groups and changes in knowledge after the e-learning for group A.
Reporting
The reporting of this study conforms to the Consensus Reporting Items for Studies in Primary Care (CRISP) statement. 21
Ethical considerations
Informed consent was obtained at the beginning of both the survey and e-learning by providing information and seeking participants’ consent. Ethical approval for this study was obtained from the Medical Ethical Committee of the University Hospitals of KU Leuven (MP022515).
Results
Seventy-two participants completed the survey (self-assessed knowledge and knowledge test), of which 58% (n = 42) identified as GPs, while 42% (n = 30) were residents in general practice.
Twenty-two participants were assigned to engage in e-learning activities (group A) and 50 respondents (group B) only completed the survey and did not sign up for the e-learning (Table 2).
Professional Experience and Experience With HIV/Pre-Exposure Prophylaxis (PrEP).
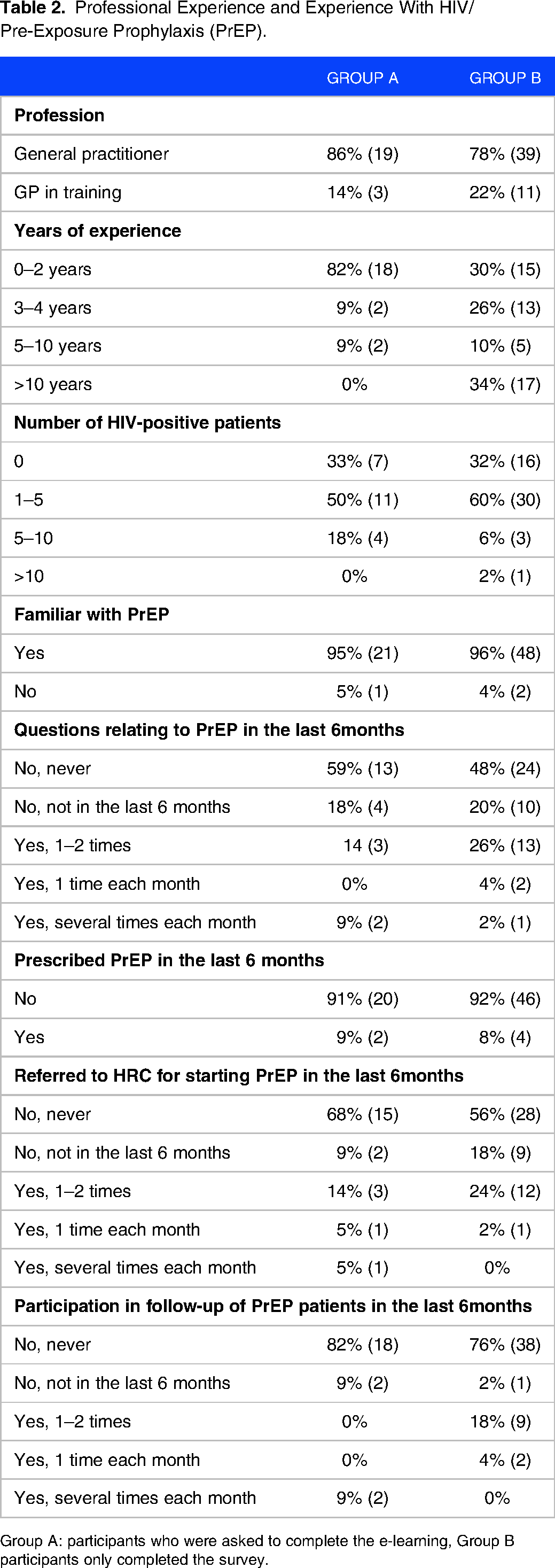
Group A: participants who were asked to complete the e-learning, Group B participants only completed the survey.
Forty-one (57%) of all participants reported that 1 to 5 of their patients were HIV positive, while 96% (n = 69) were acquainted with PrEP. Half of the participants (51%, n = 37) indicated never encountering any inquiries related to PrEP, whereas 29% (n = 21) reported having patients inquire about PrEP within the last 6 months. Over the same period, 6 (8%) physicians prescribed PrEP, 18% (n = 13) engaged in the follow-up care of PrEP patients, and 18% (n = 13) referred patients to an HRC for initiating PrEP.
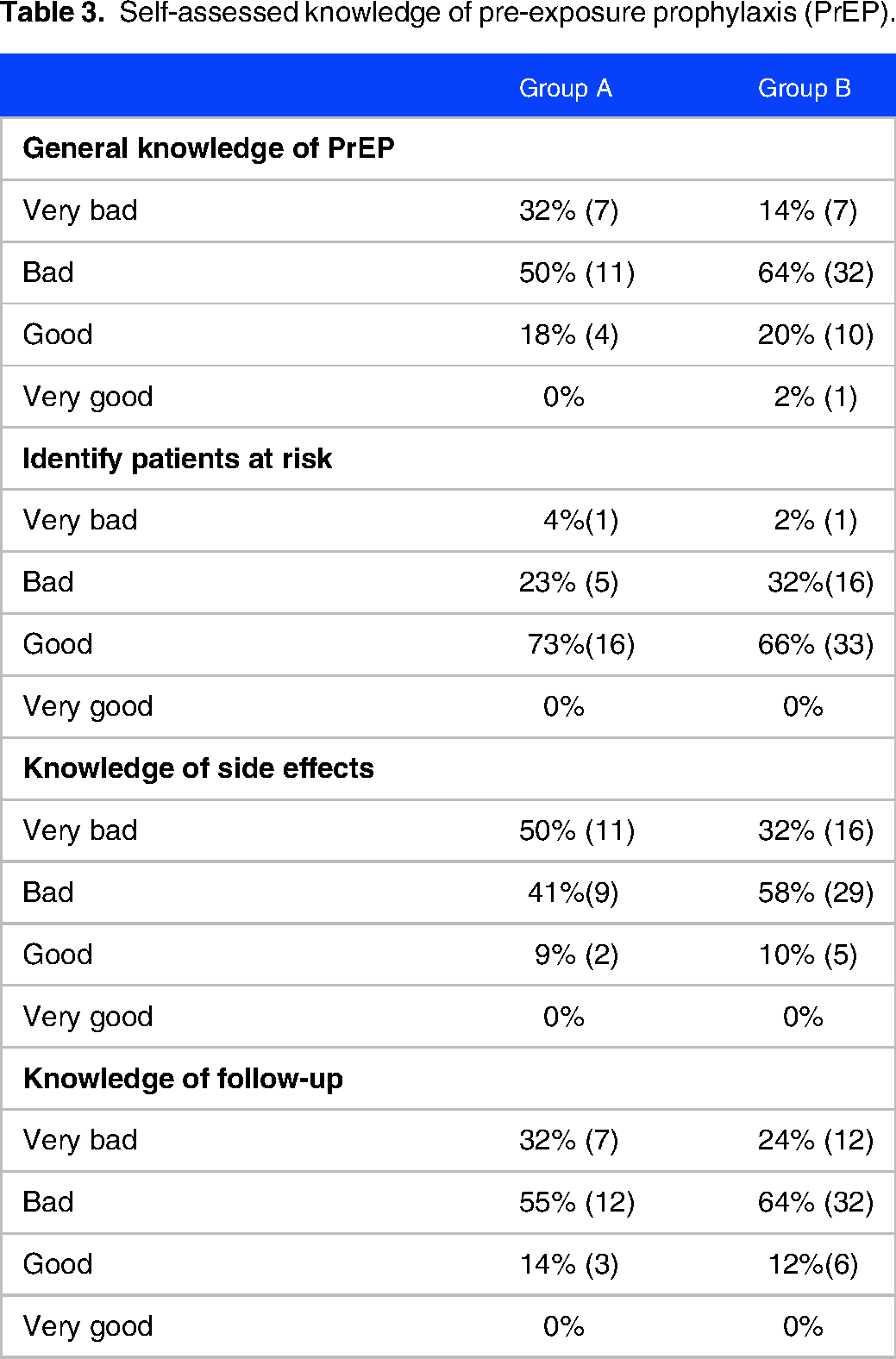
Nineteen percent of the participants (n = 14) considered their general knowledge (self-assessed knowledge) of PrEP to be “good,” while 68% (n = 49) of the GPs felt confident in identifying patients at risk, rating their ability as “good” (Table 3). In group A, 50% (n = 11) indicated that their knowledge about side effects was “very bad,” whereas in group B, 58% (n = 29) expressed their knowledge as “bad.” Sixty-one percent (n = 44) of the participants assessed their knowledge of follow-up procedures as “bad”.
Self-assessed knowledge of pre-exposure prophylaxis (PrEP).
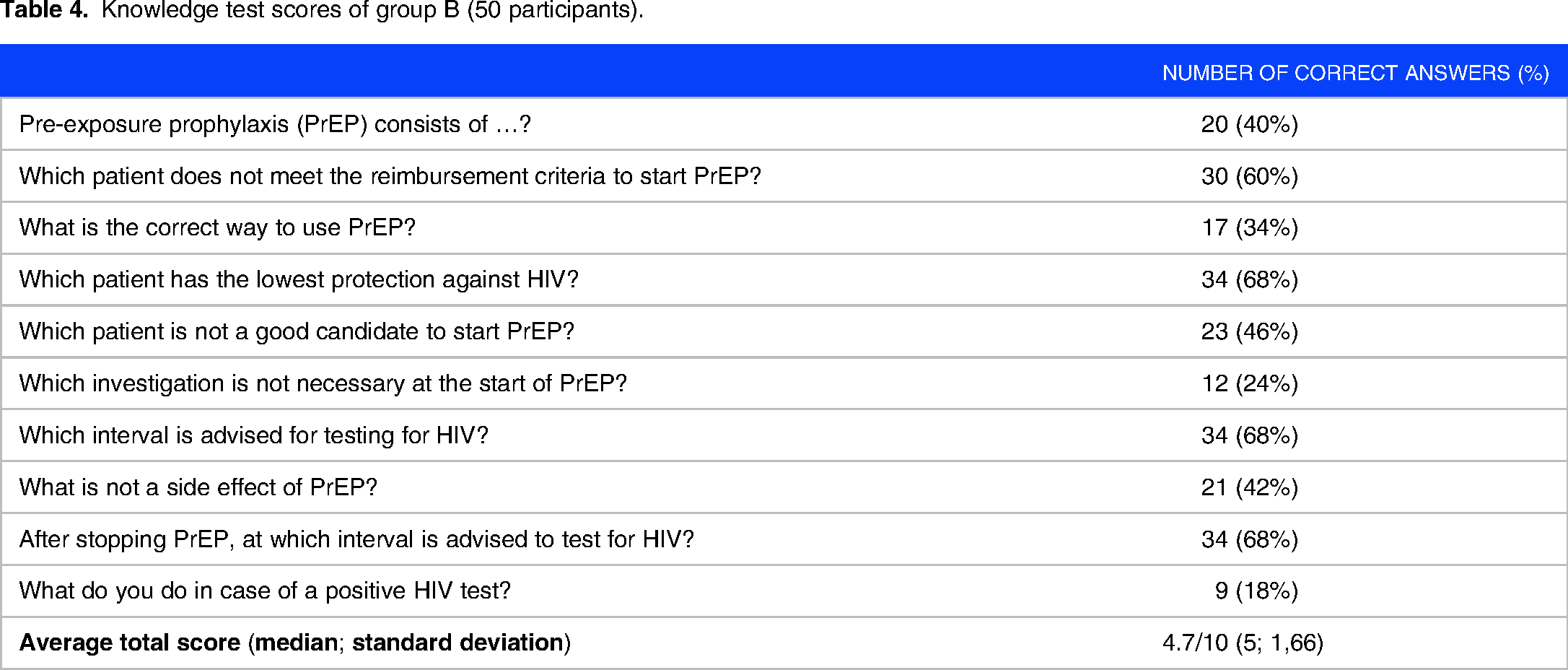
Participants in Group B achieved an average score of 4.7 out of 10 on the (pre-) knowledge test, with a median of 5 (Table 4). Questions pertaining to the identification of patients at risk received the highest relative score of 58%, while questions concerning pharmacodynamics relatively scored lowest at 40% (Table 5).
Knowledge test scores of group B (50 participants).
Results per topic of group B.

In Group A, 18 participants completed the e-learning and also finished the post-test. On the pre-test, group A achieved an average score of 4.6 out of 10 with a median of 4 (Table 6). The relative scores for questions related to the indications of PrEP reached 52%, while those concerning the use and follow-up reached 44% (Table 7).
Knowledge test scores of group A (22 participants).

Results per topic of group A.

After completion of the e-learning by group B, the overall average test score showed a significant increase of 33% (p-value < .03). Specifically, there was a 20% increase in the score related to indications (p-value < .05), a 30% increase in the score for use and follow-up (p-value < .03), a 37% increase in the score for side effects (p-value < .03), and a 38% increase in the score for pharmacodynamics (p-value < .03).
Discussion
In this study, we aimed to assess the (self-assessed) knowledge of GPs and GP residents about PrEP, as well as the impact of an e-learning intervention. Participants were given a series of questions covering different aspects of PrEP, and the average score among participants appeared to be low. However, after completing an e-learning module, participants showed a substantial increase in the average test scores. These findings highlight the potential efficacy of targeted educational interventions in enhancing the understanding of PrEP among GPs.
The results of our survey indicated that the concept of PrEP was widely recognized among GPs. Almost all of the participants indicated that they were familiar with the concept, a significantly higher percentage compared to recent studies in neighboring countries. A study in France found that only a third of the participants were acquainted with PrEP. 22
Notably, almost one-tenth of the GPs in our study reported prescribing PrEP in the last 6 months which is higher than findings from earlier research. In contrast, previous surveys revealed that only 4% of GPs had ever prescribed PrEP. 20 A similar trend is observed in the frequency of questions received about PrEP. Other studies also revealed that a substantial number of GPs never received questions about PrEP, whereas our study revealed a lower percentage, with only half of the respondents reporting having never had inquiries about PrEP in the last 6 months. 23 This suggests a rising prevalence of inquiries about PrEP among GPs, indicating an expanding awareness and interest among patients. Nonetheless, 60% never referred a patient to an HRC for PrEP, and three-quarters never conducted routine follow-ups for a patient.
The self-assessed knowledge within our study group was low, with only one-fifth claiming to possess a good understanding of the subject. Our participants assigned themselves a slightly higher score compared to the group in other studies. 23 Additionally, our participants demonstrated greater confidence in identifying patients at risk, with more than half of them stating they had a “good” understanding of risk behavior. Concerning side effects, participants had the least confidence as most of them rated their own knowledge as not good comparable to other studies.22,23
The scores attained by both groups following the completion of questions related to PrEP, both groups achieved similar total scores as expected. Notably, the subscore for the “indication” section was the highest for both groups. This observation highlights the skilled capacity of GPs in identifying patients at risk and potential PrEP users. Examining the aspects of “use” and “follow-up,” both groups demonstrated relatively low scores. This finding holds significance, as poor adherence to PrEP use has been linked to seroconversion in clinical trials. 24 GPs might play a role in increasing medication compliance.
After participants completed the e-learning module, there was a significant increase in the total average score and the subdomains on the knowledge test. These results indicate a consistent learning curve among the participants. The most substantial improvement was observed in the categories of “side-effects” and “pharmacodynamics,” but these sections comprised only 1 question each. The relatively modest increases in scores for other questions may be attributed to higher initial scores. Nevertheless, it is imperative to recognize that subjects related to indication and use are paramount for GPs, as mentioned earlier. These results suggest that an e-learning module serves as an effective method to enhance the knowledge and skills of GPs in the realm of PrEP care.
The applicability of these findings is constrained due to the limited participant pool. Both cohorts exhibited an uneven distribution, characterized by a substantial representation of GP residents or those with over a decade of experience. Second, the self-assessed knowledge and knowledge about PrEP were developed with a team of HIV and educational experts but not pilot-tested.
Despite the increased risk of sampling bias, the mean scores in both groups were comparable. This suggests that awareness of PrEP is present even when considering the focus on the subject in the training of young GPs, in contrast to the likely absence of such emphasis in past training. This phenomenon may be attributed to the pre-existing interest and higher-than-average knowledge of the subject among participants. Consequently, our findings may be prone to an overestimation of the baseline knowledge of PrEP.
Conclusions
An e-learning intervention demonstrated to be an effective method for enhancing knowledge in PrEP care. Learning interventions should specifically target themes such as indications, use, and follow-up procedures related to PrEP. Further investigation is required to ascertain whether an increase in knowledge also corresponds to an increase in the sense of competence and an improvement in the quality of care. A simultaneous enhancement in both knowledge and a sense of competence could potentially lead to greater involvement of GPs in PrEP care. This, in turn, could serve as a means to reduce costs and amplify the scale of PrEP implementation. Exploring this possibility merits further research and policy measures to involve GPs in PrEP care.
Footnotes
Acknowledgment
Not applicable.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
NV, AV, and BS contributed to the concept and design. NV contributed to data collection and analysis. NV contributed to the drafting of the article. AV and BS contributed to reviewing the article: NV and BS contributed to the revision of the article. NV, AV, and BS approved the article for publication.
Data Availability
Available via a shared link on a simple request
Ethical Approval
Ethical approval for this study was obtained from the Medical Ethical Committee of the University Hospitals of KU Leuven (MP022515).
Informed Consent
Informed consent was obtained at the beginning of both the survey and e-learning by providing information and seeking participants’ consent.