
Abstract
INTRODUCTION
The benefits of theatre and arts-based initiatives for enhancing the health and wellbeing of adults, regardless of mental health status, are well-documented. Theatre methodologies offer a platform for co-produced experiential learning, promoting perspective-taking and effective communication among staff and service users. This project aimed to bring together service users and mental health professionals through workshops conducted by an experiential theatre company, focusing on themes such as relationship dynamics, co-production, empowerment and perspective-taking. Notably, the sessions were conducted online due to the COVID-19 pandemic.
METHODS
The study sought to explore the experiences, learning outcomes and work-related wellbeing benefits of participating in this innovative project. Methods involved inviting East London Foundation Trust members to eight weekly online workshops, culminating in a co-created filmed performance. Interviews conducted 9 months to a year later with participants and facilitators were thematically analysed.
RESULTS
Results revealed four key themes: (1) personal and collective growth through storytelling and embodied acting experiences; (2) the importance of workshop structure for experiential learning; (3) challenging traditional role definitions through diminished hierarchy; and (4) sustained impacts on time management at work and in personal lives.
CONCLUSIONS
In conclusion, participants valued their involvement, indicating that theatre-based co-produced learning enhances communication and interpersonal skills in mental healthcare settings. These findings suggest the potential for integrating such approaches into healthcare education and training programs.
Introduction
Healthcare training and education have long been dominated by a traditional approach of knowledge acquisition through didactic classroom teaching. Over the course of the last decade, Kolb's notion of experiential learning has increasingly informed the development of novel training methodologies with a focus on interactive, holistic processes grounded in experience.1,2
It can be argued that creativity and nonverbal communication are key ingredients for the basic components of experiential learning methods (ie, concrete experience, reflective observation, abstract conceptualisation, and active experimentation). There is increasing evidence, both within and outside clinical settings, for the positive impact of engagement with the arts on an individual's wellbeing.3,4 Another important driver for innovations in mental healthcare training is the focus on active service user involvement and co-production, recognised by NICE (2012) and internationally.5,6
Within the wider spectrum of the arts, theatre work is regarded as a particularly suitable method for experiential learning, given its methodological focus on role play and socio-drama. Role play is also the core element of simulation training in healthcare, allowing participants to be immersed in interactive multidisciplinary learning with subsequent systematic exploration of issues encountered while enacting specific roles and clinical scenarios. 7
Prior to being utilised for training purposes, theatre work was featured in mental health services differently, with services users as passive audience members 8 or within a therapeutic context as specific drama/arts therapy practice with staff delivering the intervention. There is evidence that, for medical students, active involvement in theatre projects can cultivate both emotional honesty 9 and improve wellbeing, 10 and in nurses, it can improve morale and retention. 11 One previously conducted project explored the impact of collaboratively devised theatre methods on perspective-taking among healthcare professionals and women prisoners in a mental health context. 12 The results indicated that both staff and service users were able to share personal narratives safely; all participants described immediate enjoyment and facilitated a deeper understanding of each other's perspectives from taking part. The consistency and containment of the process being led by professional theatre makers, as well as the sense of achievement from the final performance in a professional venue, were highlighted as the main affective factors. 13 Facilitated co-production between theatre/university professionals and women in the criminal justice system led not only to improved self-esteem and confidence in the women prisoners but also positive changes in the professional institution involved in the project. 12
This project was conducted at and sponsored by ELFT and aimed to integrate the staff and service user facing strands by creating an innovative theatre project where healthcare staff and service users engaged in a process of facilitated co-production for experiential learning. The short-term aim was to develop confidence and trust among participants taking part in the project as a prerequisite to deeper sharing of personal experience. Conceptualising professional and personal development as a process of reconnecting with compassion and positive motivation related to roles and responsibilities at work, the project was seen as part of the wider learning culture for staff (with protected time during work hours). For service users, while the project was deliberately not designed as a therapeutic intervention, participation had some resemblance to community arts projects with a view to fostering social inclusion (feeling connected to others) and challenging stereotypes (ie, ‘us and them’, ‘staff and patients’).
The research questions that guided the thematic analysis used for our study were as follows: (1) What were the experiences of the participants who took part in the Playing On (POn) experiential learning project? And (2) What was the enduring impact of the Playing On (POn) project on the professional work (roles and responsibilities) and wider wellbeing/lives of the participants?
Methods
Playing On workshops – facilitated experiential learning
POn is an innovative theatre company that works with experts by experience and experts by profession with the aim of exploring relationships and improving the wellbeing of all. The POn project was a collaboration between POn Theatre Company and ELFT that took place between November 2020 and March 2021. The project recruited ELFT staff from a variety of professional roles, including occupational therapists, psychiatric and paediatric doctors, psychologists and drama therapists, along with service users, to take part in a series of workshops leading to the creation of short films. Eight weekly workshops (3 hours each) were held online and were facilitated by four staff members from the POn theatre company. Members of the POn team are a combination of experienced theatre makers and those who have lived experience of the target group, in this case mental health service users who are trained in-house at using process drama techniques with an emphasis on emotional safety. The POn delivery team comprised a professional director, a professional writer, a pastoral support worker and a theatre maker with lived experience as a service user.
Following the workshops, an intensive fortnight training period was provided, during which POn facilitators were continuously present and participants would visit to rehearse and film their parts. These were edited by a professional film maker to create two short training films and a longer film exploring the perspectives and challenges of all those who make up a hospital community. The restrictions on movement due to the COVID-19 pandemic resulted in participants filming in smaller groups, or individually, and over a longer period than POn would usually use for this type of project.
The workshops were structured in two ways. First, as a series of spaces where participants would use a metaphor to talk about their feelings, a gathering space where people would share and discuss the themes of the work, and a closing space where people could reflect on the process and reconnect with themselves to leave the work in the room. Concurrently, the workshops also used process drama-derived activities such as improvisation and collaborative character development; participants and facilitators co-produced characters and scenes before a writer and the artistic director shaped the story, which was then filmed in parts and collated as a final performance. More detailed information about the workshops is provided in Appendix 1 (Supplemental Material).
Participants
All staff within ELFT received an invitation to partake in the POn project through a trust-wide email, while service users were recruited through the People Participation team of the trust and their community mental health teams. A total of 15 individuals, consisting of both employees and patients of ELFT, expressed interest in participating after seeing the advertisement. All 15 ELFT staff or service users who indicated their interest were included in the study. No specific exclusion criteria were applied in for participants to begin the project.
Throughout the project, eleven participants remained consistently engaged by attending the majority of workshop sessions, contributing to the final script, and actively participating in the filmed production. This group comprised four doctors, three service users, two occupational therapists, one drama therapist, and one psychologist, with nine female and four male participants. All 11 individuals who successfully completed the study were invited to participate in the interviews via email. There were four participants who were invited to join the project who were unable to attend consistently and didn’t contribute towards the script or final performance. These participants were not invited to take part in the interviews. For the qualitative evaluation component of the project, all participants, along with two POn facilitators, were invited for interviews. This included the eleven individuals who took part in the final performance, as well as the two primary facilitators. Given the limited number of possible interviewees all participants who finished the project were invited to interview and the researchers conducting the thematic analysis did not pursue a data saturation methodology (see Figure 1).
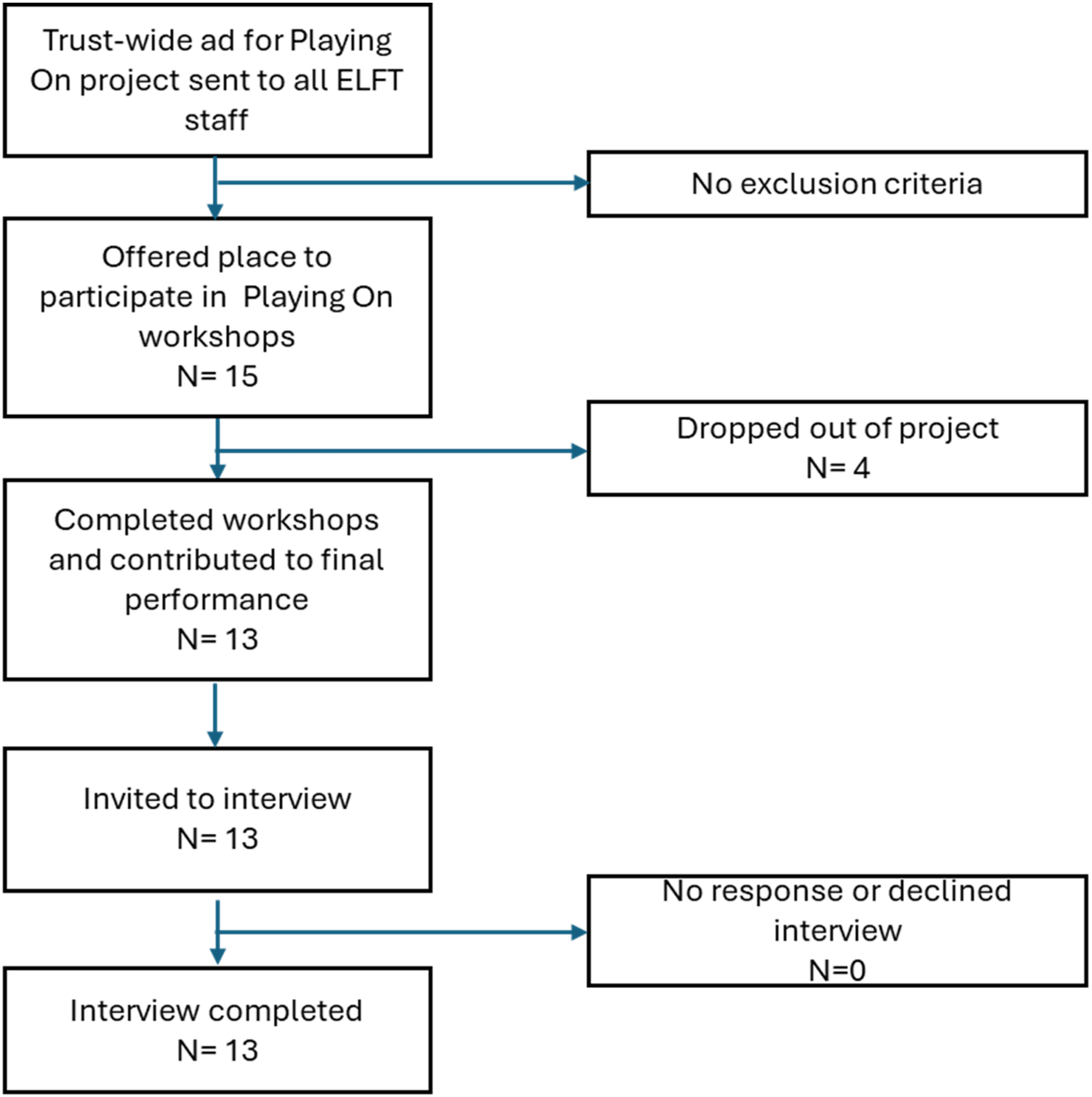
A COREQ (consolidated criteria for reporting qualitative research) flow diagram showing the recruitment and interviewing of participants to the Playing ON project.
Ethical approval
Ethical approval for this study was approved on the 8th of July 2021 (reference number G2106e) from the East London NHS Foundation Trust ethics committee, specifically for service evaluation projects. All Participants were approached and informed already at the beginning of the project about the evaluation intentions, and all agreed to take part, providing written informed consent, after being provided with detailed information about the study purpose, data collection and study method (Participant Information Sheet [PIS]). The PIS explained the process of the interview, no particular risks were identified; it was clearly stated that in the unlikely event that a participant might become distressed while taking part, the interview would be stopped, and that participant could withdraw from the study at any moment in time. Interviews were conducted by health care professionals, trained in research methodologies.
Data collection
All participants were informed that they would be invited to take part in a post-course evaluation prior to the start of the project. The timeline for interviewing participants was impacted by the COVID-19 pandemic. While there may have been some effect on the recall of participants to be interviewed up to a year after the project, most participants were able to recount their experiences in considerable detail. Participants were contacted via email between nine and twelve months after the end of the project with a reminder of the details of the post-project research study.
Interviews were semi-structured and led by a topic guide that was created specifically for this project (see Supplementary File 1). Researchers introduced themselves, their role and interest in the study and study objectives at the beginning of the interview. All participants were asked all questions on the topic guide with further questions guided by their specific experiences of the project that came to light within the interview. The topic guide was developed by the researchers to explore and capture participants’ experiences of taking part in the POn project. All of the interviews took place one-on-one individually with no one else present; twelve were conducted via the Zoom platform, and one was held in person. Interviews were conducted over a six-month period between July and December 2021 and were conducted by three researchers (HGP, RD and TW), all of whom are medical doctors, independently evaluating outcomes. RD, TW, TJ had no relationship with any participants prior to the study, HGP had a prior relationship with one participant (doctor) who was interviewed for the study, but TW conducted that interview. FR was not involved in obtaining data or conducting interviews. The interviews were between 21 and 74 minutes in duration. All interviews were recorded by Dictaphone and transcribed manually by the researchers.
Data analysis
The data were analysed using a thematic analysis. Thematic analysis, as described by Braun and Clarke, 14 allows for theoretical flexibility. Several decisions about how the qualitative data should be analysed are set out prior to the start of the analysis. The three researchers completing the analysis (RD, TJ and TW) met to discuss how their individual knowledge of related research and professional backgrounds could impact the findings of the thematic analysis to ensure that a theoretical standpoint was established accordingly. None of the three researchers conducting the thematic analysis had significant knowledge of the topic prior to the data collection and analysis.
An essentialist/realist epistemological framework was applied whereby a direct relationship is assumed between the language used by participants and the meaning implied. 14 Themes within the data were generated from the transcripts and recordings in an inductive or ‘bottom-up’ way. 15 Themes were identified primarily from the explicit meanings of the interviewees at a semantic level. As the data were organised and interpretated during the coding and theming process in some instances, the three researchers looked beyond the surface meanings to a degree and described underlying latent ideas. Final themes were the result of a combination of the frequency of coded data and a sense of the relative importance of recurring instances that, with time and over many iterations, amalgamated into categories.
The thematic analysis followed the six stages outlined in Braun and Clarke. 14 The researchers familiarised themselves with the whole dataset through multiple readings and listening to the transcripts and audio recordings of the interviews. Each researcher developed bespoke codes inductively for all data items. After developing initial codes independently for each transcript, researchers met to discuss their respective codes. The differences in interpretations between researchers were then discussed to reach agreement. The codes were analysed further to generate initial themes. The original data were revisited several times; through several iterations, themes were derived and amalgamated into overarching themes. This process was collaborative, and opinions were sought within the wider research team where there was ambiguity. Throughout the thematic analysis, researchers discussed how their own personal experiences, opinions and professional identities may influence the themes derived from the data. After completing the thematic analysis the researchers (TW, TJ and RD) collectively reflected on their experiences in analysing the data.
Results
Theme 1: personal development, group development and group cohesion
Subtheme 1.1: individual development and wellbeing
Participants arrived at the project with varied experience of involvement in the performing arts and appeared to hold their personal experience as an important factor that drew them to the study. The vast majority highlighted a pre-existing interest in creative endeavours that were mainly held in their personal rather than professional lives and went on to explain that they saw the project as an opportunity to bridge their personal interest in the arts with their professional lives. Participant #3 (P.3 Psychiatrist): ‘I always found things to improve – understanding my patients, improving communication skills, and learning through drama or any kind of resource other than medical books – very interesting’.
Alongside this, the novelty of the project and the potential for its application within their respective roles and wider lives appeared to be a motivating factor for several participants’ involvement within the group. Participant #12 (P.12 Service user): ‘I come from a teaching background and we used to do a lot of these things, like role plays, even in teaching and learning. So it all sounded very innovative, and an interesting project, and very creative’.
Others saw the project as an opportunity to mitigate the isolation experienced during the COVID-19 pandemic. Participant #10 (P.10 Service user): ‘She [facilitator] was trying to make sure that other service users don't get lonely or isolated at home and have that impact their mental health. So, something to keep them busy, and that's why I did it’.
Although there was curiosity and enthusiasm, participants across all backgrounds often started the project with a degree of apprehension, having had limited experience within the theatre or acting. They described that as the project progressed, their confidence improved, and the healthcare professionals in particular reported a wellbeing benefit often linked to enjoyment of the work environment. With time, many appeared to become more assured in the value of creativity within healthcare settings. Participant #11 (P.11 Psychiatrist): ‘There were points last year when I felt very drained. I wasn't always enjoying my job, and I think this current project has just given me something in my week that is quite fresh and new’. Participant #1 (P.1 Service user): ‘It made me braver when I worked with a QI team. Realising life isn't all about… numerical output of what you do, that there is space for me to create in other ways. And to actually be appreciated for that is kind of life-transforming. That there are ways I can work and people can accept me and get it’.
Subtheme 1.2: collective development and benefits of the group environment
The environment established by the POn team and the experience of interacting within the group were positively reported. Those taking part often reported feeling valued, valuing the contributions of other participants, and drawing reward from observing others develop throughout the project. Participants felt safe and able to express vulnerability, which seemed to foster a sense of connectedness and belonging that was derived as a significant benefit from the process. Participant #4 (P.4 Clinical psychologist): ‘It was nice to see some participants, for example, didn't feel comfortable having their videos on at the beginning, but for the second half of the project, their cameras were on, and people were able to take more risks’. Participant #9 (P.9 Occupational Therapist): ‘Human beings have these struggles, you know, and it was good to be able to hear those and get a lot of support from each other’.
The process facilitated by POn appeared to allow for an authentic reflective space. Breakout rooms for further exploration were highlighted as an important factor for participants who appeared to value the act of being able to reflect on a collaborative footing rather than being a solitary pursuit. Participant #2 (P.2 Arts therapist): ‘Quite early on, when going to a breakout room we were given something to work on… it affected both of us – there was a time to talk about it as well… he was talking about his own confidence… and I was thinking about sort of familiarity I am with working in that way, but actually the confidence. I’m in a different place.. so yeah, it was having enough confidence to be able to enter into something which we were sharing together’.
Service users tended to report positively about being heard and having greater agency within the space. Doctors and therapists often spoke about the benefits of being held in, rather than holding, a therapeutic space. They described transactional aspects that were compared to usual working practices – being afforded the opportunity to receive, rather than give. Some participants experienced this on a more profound level than others. P1: ‘I think it showed me that one of the phrases I tried to share with the group was about ‘imagination is magic-ing something new into the world’ and actually, I could say if I hadn't been there that that part of it wouldn't have happened. So I think, feeling that I could work somewhere where they trust my imagination’. P4: ‘It made me think something perhaps I hadn't mentioned was that actually part of my participating I guess it was for me to be a participant, rather than the facilitator and have that freedom of being able to just receive and be cared for, and thought about, rather than always being on the other end’.
An aspect of the group that was viewed less favourably was that several members taking part in the project were from the same community mental health team. This imbalance was noticed by other members in the group and appeared to impact their sense of belonging. Participant #6 (P.6 Consultant Paediatrician): ‘I felt like a bit of an outsider sometimes because there was a group of clinicians that knew each other’.
Subtheme 1.3: storytelling, play and embodiment
The POn workshops were structured to include using the shared experiences of participants to develop characters and a script. Several participants spoke of how they experienced developing their capacity to play, improvise and create stories. There was a sense that participants were able to grow into working creatively as the project developed. P1: ‘I think the project… made me braver, made me trust my creativity. It made me realise that there was enough space to choose a role. I think, in the past, I thought “I can't fit into the work system – it's too limiting, the roles are too limiting”. What I realised is that I can do something like this and my creativity can be encouraged. That is massively healing’.
The development of storylines through the input of people from a wide range of backgrounds was frequently spoken about by all groups and individuals and described as having extended the participants’ understanding of others’ experiences. Many participants reflected on how they felt the variety of professional roles within the workshops enhanced the breadth of the storylines and enabled them to see things from a different perspective and expand their thinking. P6: ‘I think this type of storytelling… helps to create compassionate experiences, because you begin to understand from all the different people's perspectives and you start to have a very holistic understanding of the system – of, you know, the patient, the clinician, the hospital environment, the clinic that you know’.
Participants described how the theatrical workshop activities demanded embodying the act of playing the role of another and how for some participants this was an enduring impact of the project. P4: ‘The character development… could be something like, “Right, think of a colour” or “Think of what this person sees outside the window”, and, all of a sudden you're into your character's mindset and then you're acting it, and I think it's something very different, because in that way you're embodying and expressing the thought or the hypothesis you have in your head… you're living the relationships that you're considering’.
Furthermore, participants reflected on how the experience of sharing stories and creating together in this way had brought them insight into each other's lives. There was a recognition of the vulnerability of doctors as a professional group by the other participants. Participants reflected that, prior to the project, doctors were perceived as unable or unwilling to share their personal experience. By doing so during the project, stigma was reduced. P12: ‘I think with service users and carers working together – they were able to see that even professionals can have mental illness…, it was very… nice to be able to share your experiences openly… It has definitely helped people to talk about their own struggles and mental health, and it has helped to reduce that stigma around mental health, regardless of whether they are a service user, carer or professional’.
Subtheme 1.4: therapeutic experience of the group
Although the POn project was distinct from, and not intended to be, a clinical mental health space, there was a strong sense that this separation was less clear in the experience of participants. The language they used often directly or indirectly implied a blurring of boundaries between the workshop and the clinic. Many of the participants spoke about how the project positively impacted their own mental health and how taking part in the sessions felt ‘therapeutic’. P4: ‘I think it has helped me develop in some way … It was almost like a therapeutic group… I think having consistency and doing it weekly… the structure was the same every week and something about that was quite containing’.
Participants described feeling able to talk ‘openly’, ‘honestly’, being treated ‘equally’ and feeling able to be ‘vulnerable’ as important to the experience of the group. These attributes of the group were experienced by some participants as healing or therapeutic. P1: ‘So there was a kind of bond within the group that we were vulnerable together. We had a safe space. But we all reaffirmed each other in our vulnerability and actually gave each other a lot of affirmation, so that's very healing’.
An experience of the group as explicitly therapeutic or as having improved their mental health, wasn't was not universal among participants. One participant with a background in arts therapy commented that although the workshops were not intended as therapy, the project may have benefitted from acknowledging the parallels and incorporating some of the aspects of therapy to enhance the experience. P2: ‘I was very aware that it wasn't a therapy session and I was trying to hold the boundaries of working using theatre in a place where this is not run by therapists. And I suppose my argument would be… let's have a therapist in there and input in there, actually, because then you've covered everything and just have that clinical expertise…’
The freedom participants described in being able to explore roles not otherwise afforded during their day-to-day lives led to a collective experience of expanded perspectives that may not have been achievable through solitary reflective processes. In collectively building a script, thought was given to some work colleagues in a way that perhaps had not been before, such as maintenance staff and cleaners. As one senior medical doctor explained: P3: ‘I found that when we were really being in that role and were playing it, I always felt strongly about each character, like a homeless person that one of our colleagues played, or a young adult that one of our service users played… so I really felt compassion towards those characters, as I said the cleaner, which was a really strong and powerful connection that I have felt’.
Furthermore, the outcome of the type of reflection experienced during the POn project not only appeared to help participants develop greater compassion but also prompted them to view individuals and systems more completely. With time, the layers of reflection and improvisation synergised, and participants explored together the roles they and others held and enacted. Participants spoke about their reflection on their place within the system as a whole and how individual actions have the potential to elicit far-reaching consequences. P12: ‘Service users, carers and professionals might have their own perspectives, and to be able to understand when everyone comes together … it was really insightful and something I’ve learned a lot from. I have a better understanding now of people's personal and professional experiences and how they can play different roles in different situations’. Participant #5 (P.5 Consultant psychiatrist): ‘Personal relationships with people you’ve had over the years… You explored how you communicate with other people or how other people affected other people within systems and institutions as well’.
In opposition to this, one participant felt their perspective of other participants was relatively unchanged and that the project had little discernible personal impact. P4: ‘Has it changed my perception of relationships with service users? Huh… not really. I’d say, I used my perception and relationships of past experience of service users, to inform the project rather than the other way around’.
Theme 2: project process and logistical aspects
This theme speaks of the direct experience of the environment created by the team, how the facilitation of the sessions provided the foundation for participants to support each other and collaborate, and the logistics of the sessions. Participants provided diverse feedback on positive and negative practical aspects that were, at least in part, influenced by their roles outside the space.
Subtheme 2.1 facilitators and the project environment
Participants regularly described the environment created by the POn team in a positive light. Many spoke, or alluded less directly, to a culture of respect and equality where people were free to contribute as much as they were comfortable with. P12: ‘Trusting, safe and supportive… that enabled people to… open up and… have the courage to share their experiences and be honest about them’.
At the outset, the facilitators and the group created a set of ground rules together. This shared experience was broadly remembered by participants as the starting point for the development of what became a strong bond that provided safety to share material that they had not shared within comparable NHS team group work or staff reflective spaces. Participant #8 (P.8 Occupational therapist): ‘I believe that when you create an effective community then… individual difficulties can be held in it… Playing On creates community that enables people to share what they need to share. And so even in the characters I played, I mean, I think there was a high degree of vulnerability in the degree of my participation’.
Facilitators provided an ‘equal’ space and appeared adept at allowing participants to bring ideas to this space and at points actively modelled this approach in front of the whole group. P5: ‘They listened, and they were empathetic and they reflected, and they came back to things. A good example is, I remember talking about something and then later when someone brought it up, and I thought, “Gosh, they remembered that”’.
Participants reported feeling comfortable in exploring topics in what was a ‘creative’, ‘playful’ environment. The idea that the environment was safe to make mistakes, experiment and, ultimately, learn was a perceived benefit to individuals. P8: ‘We can't play… children can't play unless there's a sense of, like, safety. It is creating that space to kind of learn as well, isn't it, to learn from your mistakes. Essentially children are learning from… what sometimes doesn't work’.
Subtheme 2.2: process of the project
Participants recognised what they felt was a clear structure in terms of allowing the group to set boundaries which established trust and respect early on. Participants frequently commented on the provision of opportunities for reflection outside the main group in smaller group settings, such as breakout rooms, and valued these opportunities as contributing to the development of trust. Participants particularly enjoyed how sessions were introduced through warm-up activities that were experienced as entertaining and novel by many. P6: ‘There was always this style of introducing ourselves at the beginning and it could be, these theatre-type techniques, like, ‘Imagine that you are a type of weather’ or ‘What's your favourite food?’, “What would you be?”, or “How are you feeling?”. And all of us introduced ourselves in that way, not in the way when you have a clinic meeting or something else’. P4: ‘You’d start by saying, well, ‘How do you feel today?’, like, pick an object that represents it. Then, you are hearing about people's lives as well. And I think as we grew into each other, it was really nice to say, “D’you know what, you’ve had a really hard day, I’m going to give you x as a gift to make it better’.
While some of the aspects of the workshops, such as the start time and the duration, remained fixed, much of the content of the workshops varied. Participants spoke positively of the variability and flexibility of the session content. The improvisation activities were particularly popular: P11: ‘It was organic, it just came out of improvisations and grew each week’. P6: ‘It's made me more experimental because it was all improvised, and I’m very used to scriptwriting, I still write scripts. But you get obsessed with writing and which word you put here and which word you put there, and so improvisation is just delicious because it's just, you know, “Have a go and see what comes out. What's in your head, let's see how it works”’.
While this freedom to improvise was often seen as positive, particularly with participants who were therapists and doctors, some expressed their frustration with the perceived lack of direction and some disappointment in the perceived unclear overall aim of the project and the final performance. P9: ‘A bit clearer about the intention of how we were going to work, maybe they wanted it to be quite open. Certainly I came into it not really knowing what I was coming into… but yeah, maybe just for me. It could’ve been a bit clearer really because I wasn't really sure what we were doing. P2: ‘My main criticism would be the quality of the editing, I’m afraid’.
Subtheme 2.3: the online setting
The context of the POn project running during the COVID-19 pandemic meant that sessions initially commenced online. Participants came to the project with preconceptions that were generally in support of face-to-face rather than online sessions, feeling that the content generated would be ‘richer’. Largely, this did not change, with many feeling that the online setting negatively impacted the quality of the final piece of work. Others saw the lack of face-to-face group contact as a lost opportunity to interact and connect with others. P8: ‘There are a lot of service users that I work with who don't have this facility’. P5: ‘Because of the pandemic, we couldn't meet up, and that physical contact would have been nice. Because it was all about drama and roleplay, so you lose out on Zoom. It would have been good to have the physical side of things, but also socially being in a room and having a coffee with someone would have been interesting and different, or even a drink afterwards so there's that social element’.
Conversely, several participants put forward alternative perspectives of the online setting, suggesting that it enabled less confident individuals to begin the project and that these participants had slowly built their presence in the sessions over the course of the project. Another suggested that the location of the project had ‘broadened their mind’ to the possibilities of working online. P9: ‘You would think that if you can't see somebody and you’re in a conversation with them, you know, like you’re meant to be in the same room… it didn't seem to hold people back. But for some people it might actually mean they could join in, because actually being in a room with other people might have felt more difficult’.
Theme 3: hierarchy, power and roles
All the participants were associated with ELFT through work or as service users and, as such, arrived at the project with established roles within the trust. Some participants knew each other as colleagues, clinicians, or service users. Many participants commented on the changes they felt in how they experienced themselves and others within the workshops with respect to their pre-existing roles and values. This theme describes the way in which participants discussed their experience and awareness of power, roles and hierarchy prior to, during and after the project.
Subtheme 3.1: hierarchy and Power
The doctors in the group were the most likely to comment on how their experiences of the workshops were different from how they were accustomed to feeling, communicating and interacting with service users and other healthcare professionals. Non-medical healthcare professionals also talked about a diminished experience of hierarchy in the project, describing this change consistently with direct reference to a ‘flattened’ or non-existent hierarchy. P6: ‘It wasn't hierarchical. Generally, if you look at clinician-client relationships, there is a type of hierarchy and a power dynamic which that is a very sad thing in a way, but it has existed historically. Whereas this is a space where we're all on the same level’.
This change was universally seen as positive by both medical and non-medical healthcare professionals. It was often cited as contributing to being more ‘authentic’ when reflecting or improvising with the group. Non-medical participants in general observed and commented on the desire among the doctors to discuss power and hierarchy within clinical spaces as a theme in the workshops. P8: A very significant theme that came from the medics was around hierarchy… they chose to be like the cleaner, or the person shouting at the cleaner, or… they reflected those themes. There weren't other people saying, “Oh, medics are like this”. So for me to see that, you know, we actually do have a lot more shared concerns and values than I might feel like at times when I feel very polarised… It was very helpful’.
Power and hierarchy were common themes of the improvisations and discussions within the group and in part shaped the final performance script. There was a sense that doctors’ interests were given priority within the final script. Not all the participants experienced a change in their perception of pre-existing roles. One service user described how they felt that prior roles endured to a degree over the course of the workshops and how they themselves continued to behave as if this was the case. P10: ‘We all worked together and we were all equal. But I just thought of myself as a service user, and the therapists and the other doctors… I was a bit nervous and I made sure that I was careful what I was saying’.
This was strikingly different from another service user's perception of power and whose description of their experience was in keeping with how healthcare professionals had largely described the workshops. P1: ‘There's a different power dynamic. So, we were all in an unfamiliar space, out of our comfort zone, choosing new roles, and it got rid of the power structure, the hierarchy, and I think… I felt very empowered, that I could choose my role in life or my role in the play’.
Healthcare professionals commented on their dissatisfaction with current healthcare practice and referred in complimentary terms to aspects of the workshops, such as the diminished hierarchy, that reframed the power dynamic inherent in more traditional medical model practice. One service user described their experience of traditional power dynamics in mental healthcare and the effect they felt their diagnosis had on medical professionals. P1: ‘I think with mental health challenges, you can be defined by different diagnoses, and there's a struggle for a meaning to life… often you meet doctors and they're looking at you through a medical perspective and not seeing all your possibilities – or maybe that's a bit of a stereotype’.
There was concern from participants as to how less hierarchical attitudes to working would be sustainable within current systems. P6: ‘We as a small group shifted culture, perhaps, and so we’re signed up to this way of thinking now, but then I have to go back to my regular system which doesn't think in this way’.
Subtheme 3.2: changing roles and values
Working together as a group of both healthcare professionals and service users precipitated many participants to compare their experience of being in the workshops with aspects of their work within, or use of, mental health services. Aspects of the workshop experience reported as less familiar within their regular mental health service routine, such as ‘flattened’ hierarchy and the authentic collaboration between healthcare professionals and service users, prompted reflections from some mental health professionals on how they feel mental health practice in its current form deviates from their values. P6: ‘I think there was a very old-fashioned model before, that had you distance yourself in your ivory tower from the patient, from the client – you know, you're fixing them so you need to be better, different from them’.
Within the sessions, all participants described both the impact of changing roles brought about through taking part in the project in general and further role changes through scripted acting, improvisation and vicariously through observation. An occupational therapist described how they experienced changing roles within the project and the enduring effect this had for them. P8: “The final thing I'd add that I've kept thinking about over the last few months is with, say, drama… People might have the perception that there's something about putting a mask on, but I think it's so much about dropping the mask… People hold on to their masks to hold on to power, really, I think. When you have the opportunity to be in another role, I think you can share… things with your colleagues that you could not share if you were just in a discussion’.
Some participants experienced the changes in the power dynamics inherited from clinical situations to be so significant as to lead to using their newly assumed autonomy to act in a way that felt novel and empowering. One service user described how they helped clinicians. P1: ‘I think meeting different kinds of staff and people that experience services was really good. Some of them I didn't know, hadn't met before, and I found that I gave a lot of encouragement to them, because I thought, “Someone says there's this perception that they're helping us,” but I was actually like no, I want to encourage you, because I found I’ve done lots of people-participation work with lots of different staff, and some of the doctors were more limited in their role of who they worked with, so actually felt it was liberating to encourage them to have a role beyond their normal role’.
Healthcare professional participants commonly described feeling that participating in the project had enabled them to work with service users in a way that they would like to replicate within their working lives. P9: ‘We're all on that continuum. I don't see my service users as “them” and “us”, and that's what was lovely when I think about what the project is, that people could show their vulnerabilities. And that's the reality of being a human being, you know, we all have vulnerabilities and it's just how we manage to cope with that. And people were seen in the group, which I thought was very powerful’.
Theme 4: the projects enduring influence
The interviews took place up to a year after the end of the project. Many of the participants spoke of how the POn project had influenced other projects they had since taken part in. Several participants new to theatre-based workshops spoke of how they were now involved in similar projects or were actively looking to become involved with similar projects. P12: ‘I'm definitely looking for more creative kinds of opportunities and projects now, and that's why I've started to do more things like this… he [the artistic director] asked me if he could use my video. It is quite nice, that's something that you created, even though it was originally created for the medical education project, but that can be used for the wider community’.
Other participants described collaborative projects created with people from the workshop group. P11: ‘I got connected to other people in the Trust who are like-minded. It's meant I've actually got involved in other projects since…I have so little contact with therapists where I work, and like as a consultant, you would never get to lead a group… So it has really led to some great opportunities for me’.
Some of the participants, most frequently non-medical healthcare professionals, had often been involved in running groups within their daily work lives prior to the workshops. These healthcare professionals were the most likely to report how the POn workshops had inspired new ways of working within pre-existing groups and projects. One clinical psychologist described how word-of-mouth dissemination of the project led to an invitation to use similar methods elsewhere in the Trust. P4: ‘People heard of the work… they've asked us to do an Away Day for them …they want us to look at themes of racial inequalities in their workspace and to use creative arts of ways to sort of explore and express that’.
Not all participants reported having been drawn to seek out further opportunities in theatre or other arts-based projects. Four participants could not complete the workshops. One explanation for leaving the project from a medical doctor in the early stages of psychiatry training was their inability to secure the time on a weekly basis due to clinical work priorities.
Reflections of the analysts of the reported qualitative themes
The strengths of our thematic analysis were in strictly adhering to our methodology of clearly defining theorical underpinnings early on. We reflected that it was important for the thematic analysis to be staggered over a period of 3 months as ideas and patterns fermented over time and allowed more flexible analysis to arise. On reflection we considered our professional roles as potential mediators of the analysis and in future would seek more diversity of professional roles within the analysing team.
Discussion
This study and its findings demonstrate the utility and efficacy of theatre-based experiential learning methods to foster collaborative therapeutic alliances between staff and service users and their impact on subjective wellbeing and work morale.
A recurrent theme from all participants was the pleasurable experience of being given a space within which they could feel creative and playful. The importance of play has long been recognised; Winnicott believed that it is ‘only in playing that the individual child or adult is able to be creative and to use the whole personality, and it is only in being creative that the individual discovers the self’ 16 (p73); he also felt that ‘creative apperception … makes the individual feel that life is worth living’ 16 (p86).
More recently, Solms 17 (p.118−119), linking evolution, neurobiology and psychology, stated that playing ‘promotes viable social formations’ and ‘is a major vehicle for developing empathy’. However, in order to be playful, and individual first has to feel safe. Nicholson 18 (p.133) recognises this in describing the need for a space ‘in which people feel safe enough to take risks and to allow themselves and others to experience vulnerability’. The sense of safety that participants spoke of emerged from specific aspects of the creative theatre-play process: the co-creation of ground rules at the start of the project, a check-in to start each session, a space to follow-up if anyone was struggling, and consistency to both structure and staff as well as a strong emphasis on only doing as much as felt comfortable. This playfulness, enabled by safety, straddles both the wellbeing and education/training aspects of the project aims, as play-therapy elements have been promoted from the perspective of experiential learning theory with specific emphasis on the context of reflective practice. Bell et al 19 describe the utility of play-based activities for the creative exploration of themes in counselling practice, such as enhancing self-awareness in supervision. While this theatre project was not designed as reflective practice or supervision the project did deliver insights for the participants and our findings support the idea that active collaborative involvement in arts projects can deliver key aspects of healthcare training/ education. This is not a wholly new area: experiential, immersive learning methods are increasingly considered in healthcare education due to their positive impact on self-efficacy and the acquisition of competency; examples include community-based experiential learning in dementia care, 20 communication/collaboration and problem-solving skills as well as clinical reasoning and critical thinking21–23. Bonsack et al 24 conducted a pilot study on “stand-up comedy inspired experiential learning” and demonstrated a positive effect on connecting emotions and cognitions in healthcare education; this and other related innovations in education seem very relevant for healthcare delivery because of the importance of emotional intelligence for empathy, therapeutic relationships and effective communication. 25
The community and group aspects of the project came out strongly in the findings, this is to be expected as the project was unusual in bringing together staff and services users in a creative forum where their roles were not relevant, insofar as POn facilitators treated all participants in the same way. As such, this project could be seen as a space where traditional assumptions about the role of healthcare professionals and patients and corresponding hierarchies could be broken down. As reflected in their interviews, the reality was somewhat more complex. Healthcare staff participants responded most positively to this less hierarchical space; they expressed a uniformly positive experience of perceived absence of the usual workplace power dynamics. Staff spoke of the experience of feeling freed from the potential constrictions, and perhaps associated responsibility and even guilt, that they usually experience at work when in their defined professional roles. This change in power dynamics was enabled through the specific project method: the three aspects of character work – first, being able to choose to play someone else, second, the actual experience of playing someone else and last, witnessing others playing someone else. At all three of these junctures, there were opportunities to connect to, and empathise with, someone else's role as well as see someone in a new light, thereby potentially diminishing stereotypes both between and within each group. These insights relating to power link to the potentially radical nature of educational experiences whereby those in power come to see themselves anew 26 and the potentially transformative nature of applied theatre projects, which, in bringing together different groups around a shared topic, can lead to changes in the wider social sphere. 27 These reflections and insights around hierarchy and power link back to the educational and training implications of the findings; participants are likely to benefit with regard to their wellbeing and staff for their professional- development and ability to develop empathic therapeutic relationships with patients.
As well as power dynamics other group-specific psychological phenomena also emerged from the interviews. This project drew on the power of group creative processes 28 as participants spoke of a sense of connectedness, understanding and supportiveness towards each other. These feelings link to Foulkes's concept of ‘resonance’ 29 (p269) and Yalom's 30 notion of ‘universality’, both of which describe the positive experience that can arise when individuals share feelings with strangers in a group setting. Both of these phenomena were mobilised in this project and can be seen occurring in other professionally facilitated, time-limited therapeutic theatre projects within which service users worked on difficult personal material to generate a sense of shared meaning.31,32 Some caution is required because groups can have the potential to be destructive via anti-group phenomena such as scapegoating, bullying, and exclusion, 33 but these were not described by participants; potentially in the longer term, less structured or less well-facilitated space such difficulties may have emerged.
An important question for similar projects in the future is how to label such educational work. Some participants (more staff than service users) spoke of a desire for more clarity regarding the purpose of the project. This perception likely resulted from the difficulty in positioning such a project, with a lack of clarity as to how to distinguish the project content from clinical contexts where therapeutic art interventions are meant to support service users. Explicitly clarifying which area the project sat within – education/training initiative, staff wellbeing offering, therapeutic intervention or creative project – may have brought clarity to all concerned. However, it may also have closed off the openness that characterised the project. The only participant who was an art therapist felt the project resembled art therapy processes and therefore ought to have had an arts therapist co-facilitating; hence, another potential benefit of not describing the project as having any one aim was that it was not taken over by a particular professional group. This final point, of allowing for a degree of uncertainty and not knowing, illustrates the complexity of both the project and the research findings – no single theme or finding sits in a distinct practical or theoretical domain: the education/training and experiential leaning aspect relies on a state of playfulness which is enabled by a sense of safety within a shared community all of which leads to an experience of wellbeing and fulfilment.
Limitations
There are limitations to the project and to the research undertaken after the project. The main project limitation relates to who took part: as noted above, not all healthcare professionals were represented, and on the service user side, any service users who were not sufficiently competent with technology could not participate. The duration is also a potential limitation; this was a relatively short project. Longer term projects with specific focused interventions could be considered, for example, offering the project to a team that is struggling with team-building challenges or service user engagement. Self-selection of participants is another significant limitation, as it is likely that those who continued to participate were more amenable to the learning methodology.
Limitations of the research methodology stem from the fact that all interviewers were doctors, which might have influenced the content and depth of the interviews. Additionally, the interview topic guide was developed specifically for the project and, due to the small sample size and the novelty of the research question, it was not validated or pilot tested. In the future, a mixed research group of healthcare professionals and service users would be ideal, and a focus group could be considered. The second major limitation was the time that had elapsed since the project had been completed. This was a concern, but researchers were reassured by the details of recall, and this time lapse allowed for more reflection on the legacy of the project.
The perceived reduction in a pre-existing hierarchy of power and any associated potential for positive change in the mental healthcare systems can be regarded as a good outcome. This finding should, however, be treated with some caution, not only because it may not have been experienced in the same way by all who took part but also because this was a self-selecting group. Those who were highly motivated to be involved in eight sessions of collaborative role-playing were perhaps not representative of all service users or healthcare professionals.
Conclusion
This study aimed to explore participants’ experiences in a co-produced experiential learning environment, designed to playfully engage with mental health practice. Participants appreciated the initiative's theatre-based approach, noting enhanced communication and interpersonal skills. Integrating such methods into healthcare education is promising. Despite a 9-month gap post-project, participants’ positive memories suggest lasting impact on both professional work and personal lives. Future research could longitudinally assess theatre-based learning's alignment with curricula and its effects on service users’ recovery, staff wellbeing, and outcomes like self-efficacy and emotional intelligence.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241278175 - Supplemental material for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry
Supplemental material, sj-docx-1-mde-10.1177_23821205241278175 for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry by Thomas Walker, Tomos Jones, Hugh Grant-Peterkin, Rupal Dave and Frank Röhricht in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241278175 - Supplemental material for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry
Supplemental material, sj-docx-2-mde-10.1177_23821205241278175 for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry by Thomas Walker, Tomos Jones, Hugh Grant-Peterkin, Rupal Dave and Frank Röhricht in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241278175 - Supplemental material for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry
Supplemental material, sj-docx-3-mde-10.1177_23821205241278175 for Evaluating Outcomes of a Co-Produced Theatre-Based Experiential Learning Project in Psychiatry by Thomas Walker, Tomos Jones, Hugh Grant-Peterkin, Rupal Dave and Frank Röhricht in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank the Medical Education team at East London NHS Foundation Trust for their operational and administrative support. They are grateful for the enthusiastic and professional facilitation of the training program by the Playing On theatre company, in particular the artistic director Jim Pope.
Authors contributions
FR developed the study design, provided supervision for the project and contributed to completing the manuscript for publication together with TW and HGP; RD, TJ and TW conducted the qualitative thematic analysis, analysed and interpreted the data and wrote the results section. All coauthors read and approved the final version of the manuscript.
Availability of data and materials
At reasonable request.
Consent for publication
Written informed consent was provided by the participants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval and consent to participate
Ethical approval for this study was approved on the eighth of July 2021 (reference number G2106e) from the East London NHS Foundation Trust ethics committee, specifically for service evaluation projects. Written informed consent was obtained from all participants after they had the opportunity to review the study procedures.
Experience and training of researchers
TW has undertaken previous published research using qualitative research methods and thematic analysis. HGP had training in qualitative research as part of his MA in Medical Education and has undertaken previous published research using qualitative methods. RD is currently undertaking an MSc within which she has received training in qualitative research methods and thematic analysis. TJ previous researched in the UK with the Bi-polar Disorder Research Network and in Australia with the Centre for Forensic Behavioural Science, Melbourne. FR has wide experience participating in research programmes, leading research teams as Principal Investigator and conducting quantitative and qualitative data analyses.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.