
Abstract
Objectives
Medical Assistance in Dying (MAiD) was legalized in Canada in 2016, necessitating greater education and training in MAiD for physicians and nurse practitioners. To meet this need, the Canadian MAiD Curriculum (CMC) was developed to offer a nationally accredited, comprehensive, bilingual, hybrid (synchronous and asynchronous) educational program to support and enhance the practice of MAiD in Canada.
Methods
This work describes the process of developing the CMC, including its guiding principles and framework. The CMC was guided by constructivism and adult learning theory, preliminary literature review, 5 key principles based on a needs assessment survey, as well as consultation with diverse partners.
Results
Seven modules were developed: (1) foundations of MAiD in Canada, (2) clinical conversations that includes MAiD, (3) how to do an MAiD assessment, (4) capacity and vulnerability, (5) providing MAiD, (6) navigating complex cases with confidence, and (7) MAiD and mental disorders. An eighth topic on clinician resilience and reflection was woven into each of the 7 modules.
Conclusion
This curriculum ensures that consistent information is available to healthcare providers concerning the practice of MAiD in Canada. To ensure sustainability, the CMC will continue to be updated alongside the evolution of MAiD policy and services in Canada.
Introduction
Canada legalized Medical Assistance in Dying (MAiD) in 2016, which enabled adults suffering from a “grievous and irremediable medical condition” to seek the assistance of a physician or nurse practitioner in ending their life. 1 In 2021, MAiD eligibility was clarified to include individuals whose natural death may not necessarily be reasonably foreseeable. 1 A further extension to make MAiD available to individuals suffering solely from mental illness has twice been deferred due to concerns of readiness and is anticipated to become available to patients from March 2027.2–4
From 2016 to 2022, 44,958 people in Canada chose to end their lives using MAiD, 3 with numbers rising annually.3,5–7 MAiD legislation is an amendment to the Criminal Code of Canada. However, the organization and delivery of healthcare is the responsibility of each the 13 Canadian provinces and territories. 8 As a result, the implementation of MAiD across Canada, including the education and training of MAiD practitioners, has not yet been standardized.
A burgeoning literature on MAiD in Canada has identified a need for greater education and training to guide healthcare providers in the new and evolving practice of MAiD.9–15 In the early years of MAiD practice, some optional educational programs emerged to fill this gap. For example, the Canadian Medical Association provided a course on MAiD, 16 which was available in English only (and is no longer publicly accessible); while Collège des Médecins du Québec provided French-language guides and tools for clinicians for Track 1 (ie, a request for MAID made by a person whose natural death is reasonably foreseeable). 17 Clinicians seeking to learn more about how to provide MAiD care could access periodic teaching sessions put on by the Canadian Association of MAiD Assessors and Providers (CAMAP), 18 a not-for-profit and now charitable organization founded in 2016 to support the diversity of professionals providing MAiD-related care. Individual organizations or locoregional MAiD clinicians also occasionally and irregularly provided teaching; and in some areas of the country, one-on-one mentoring was available, though not consistently. Indeed, a lack of sufficient knowledge and training has been recognized as a barrier to becoming or staying involved in MAiD work by many physicians and nurse practitioners. 19
In 2021, CAMAP was approached by Canadian parliamentarians to create a national MAiD training curriculum. The goal was to fill an unrealized need to ensure that the training for all clinicians involved in MAiD care is uniform, accessible, and encourages interdisciplinary collaboration and support. Implemented as a national quality improvement initiative related to MAiD practice, the Canadian MAiD Curriculum (CMC) was CAMAP's response to this request. The CMC aimed to create a comprehensive, nationally accredited, bilingual, hybrid (synchronous and asynchronous) curriculum to help standardize a high-quality approach to MAiD practice in Canada. The aim of this manuscript is to describe the process of developing the CMC, including its guiding principles and framework. We also outline the intended implementation and evaluation plan.
This study was conducted according to the Standards for Quality Improvement Reporting Excellence for Education (SQUIRE-EDU). 20 All evaluation activities referred to in this paper were approved by Queen's University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (File #: 6037011) and the University Health Network Research Ethics Board (REB #22-5225.0.1) UHN Research Ethics Board (#18-6305).
Methods
Theoretical framework
Both constructivism21,22 and adult learning theory 23 guided the development of the CMC. Constructivist theory emphasizes the importance of interaction between learner and material, suggesting that learning objectives are met by “constructing” rather than “acquiring” knowledge, thus supporting the use of content that promotes active engagement and problem-solving rather than rote memorization. 21 Among the guiding principles for effective adult education posited by Knowles et al 23 is the importance of adult learners feeling that their learning has immediate utility, is focused on issues that directly affect them, and will result in performance improvement. Adult education is most effective if learners also have autonomy in controlling their learning and are able to learn in a climate that is collaborative, respectful, mutual, and informal. 23
Both constructivist theory and adult education theory emphasize the need for the curriculum content to be tailored for the learner, with immediate applicability to real-life clinical situations. This framework informed the CMC's development, as the curriculum aims to leverage MAiD practitioners’ existing subject matter expertise; use realistic and relatable case examples; and provide information that has concrete and immediate applicability to clinical practice.
Curriculum development principles
The guiding principles that informed the foundation for the CMC were created through the preliminary work of CAMAP, including consultation with invested partners and a formal needs assessment of physicians and nurse practitioners across Canada.19,24 A needs assessment survey was conducted between December 2021 and March 2022, with a focus on identifying educational and training needs as well as motivations and barriers to becoming and staying involved in MAiD practice. An online, cross-sectional, mixed-methods survey was distributed by CAMAP to practicing physicians and nurse practitioners across Canada through member lists of partner organizations. 19 In addition, feedback from CAMAP training events dating back to 2018 was also used to inform the development of the curriculum.
Needs assessment survey results
A total of 257 responses were collected from the needs assessment (67% female), with 40% of respondents indicating that they were or had been involved in MAiD. 24 Respondents were physicians (57%) and nurse practitioners (33%), and practiced in a range of settings including in the hospital (60%), community (34%), and university (6%). 24 In terms of substantive content, the areas that were most frequently identified as being “important” related to assessing MAiD in the context of certain patient populations (eg, those with depression, neuropsychiatric disorders, or somatization disorders), as well for those who have communication challenges. Among the top factors identified as “helpful” in promoting MAiD involvement by both practicing MAiD clinicians and those not involved in MAiD practice included peer support to review complex cases and best practice guidelines. Compared to their counterparts, practicing MAiD clinicians were more likely to consider interprofessional support for the MAiD process (eg, administrative, social work, and nursing), compensation/easy access to billing codes, and support for completing documentation as helpful promoting factors. In both groups, approximately 50% reported that accredited low-cost education would promote more involvement in MAiD work.
While excessive current clinical workload, discomfort when natural death was not considered reasonably foreseeable, and lacking logistical/administrative support were among the most frequently reported barriers among both practicing clinicians and those not involved in MAiD work. However, those not involved in MAiD work group was more likely to consider certain issues as prohibitive barriers. These included but were not limited to concerns such as knowledge gaps, the inability to absorb MAiD into current practice, uncertainty about documentation requirements, as well as personal or ethical concerns. 25
Regarding preferred learning format, over half the respondents identified asynchronous online modules with text and cases studies (60%); online facilitated sessions with topic expert (55%) and small group facilitated sessions with a topic expert (40%) were also commonly cited, with many participants selecting multiple learning formats. 25
Guiding principles
The following 5 principles, based on the results of the needs assessment survey and consultation with invested partners during the planning phase of the project, served as a foundation for the CMC's development:
Standardized Clinical Education: The CMC aims to enhance the knowledge, skills, and confidence of existing clinicians practicing MAiD, as well as educate new MAiD practitioners, by providing standardized training that meets the highest standards of patient-centered MAiD care with a focus on topics of greatest salience to professionals in the field. The clinical education will be standardized and accredited by all 3 relevant national organizations responsible for clinician oversight (ie, the Royal College of Physicians and Surgeons of Canada, the College of Family Physicians of Canada, and the Canadian Nursing Association). Accessibility: The CMC aims to be accessible to busy professionals and feasible to complete. The CMC is available in both of Canada's official languages (English and French) and in a variety of synchronous and asynchronous (hybrid) learning formats, so that it may be available to clinicians regardless of geography. Iterative Evaluation and Sustainability: The CMC aims to disseminate an evidence-based approach to MAiD assessment and provision across Canada. The CMC underwent iterative formative and process evaluations prior to “going live,” and summative evaluations thereafter. The CMC will continue to update and revise the curriculum based on feedback and evolving practice standards. Collaborative Partnerships: The CMC aims to facilitate opportunities for sharing knowledge, enriching discourse, networking, and collaborating among diverse invested partners across disciplines, and to encourage mentoring and training activities to develop new CAMAP teaching faculty that will advance the skills of all MAiD practitioners. Equity, Diversity, Inclusion, Reconciliation, and Accessibility (EDIRA): The CMC aims to enhance EDIRA in MAiD education and help ensure MAiD services address the needs of diverse patients, families, and clinician populations, through the inclusion of Indigenous representation as well as representation of persons with lived experience (PWLE) through its Steering Committee, some working groups, and curriculum review process.
Curriculum development and review process
The CMC's modules were developed through a rigorous multistaged, multipartner process. A National Steering Committee of key partner organizations was created to ensure the needs of these organizations were not overlooked, provide support (eg, through accreditation), review and advise on content development, and help disseminate the final CMC. The Steering Committee had diverse representation from major partners involved in the delivery of healthcare across Canada. 1 A Provincial and Territorial Advisory Council (PTAC) of CAMAP comprised of experienced MAiD assessors and providers from across the country was assembled to provide jurisdictional feedback and review of the curriculum content in development.
A group of subject matter experts from across the country were recruited to form the Canadian MAiD Curriculum Development Committee (CMCDC), who met monthly over 2 years to develop the curriculum outline and objectives. Members of the CMCDC chaired 8 working groups, comprised of 4 to 8 individuals each, who were selected by the chair of the relevant group, with attention to geographic and discipline representation, cultural sensitivity awareness and gender diversity. The working groups included multidisciplinary experts in MAiD, including physicians from a variety of backgrounds (eg, palliative care, family medicine, and psychiatry); nurse practitioners; ethicists; legal scholars; and PWLE; and included representatives from 10 of 13 provinces and territories (except Newfoundland and Labrador, Northwest Territories, and Prince Edward Island).
Working groups provided content expertise, while adult learning principles and Universal Design for Learning principles were embedded in collaboration with educational developers, instructional designers, and multimedia specialists.26–28 Graphic designers and navigation and usability experts ensured modules adhered to accessibility standards. After content development, each module was reviewed by the Steering Committee, PTAC, CMCDC, and ultimately the CAMAP Board. Following French translation, each module was further reviewed by Francophone clinicians. As such, the CMC content was involved in numerous reviews and revisions to incorporate suggested feedback, a process which took approximately 23 months in total and input from nearly 100 people.
Results
Table 1 describes the 7 modules, formats, and learning objectives that comprise the CMC, as well as an eighth topic, Clinician Resilience and Reflection, that was fully developed, with components embedded into each of the 7 modules. Due to the existential nature of the subject matter, differences in opinion or moral/ethical stance were anticipated. In cases where a working group was unable to reach consensus on particular content or a formatting point, the working group chair presented the issue to the CMCDC for resolution, with escalation to the CAMAP Board if needed. Final approval of the curriculum content and format was provided by the CAMAP Board (see Figure 1).

Organization structure of the CMC project participants.
Canadian MAiD curriculum topics.
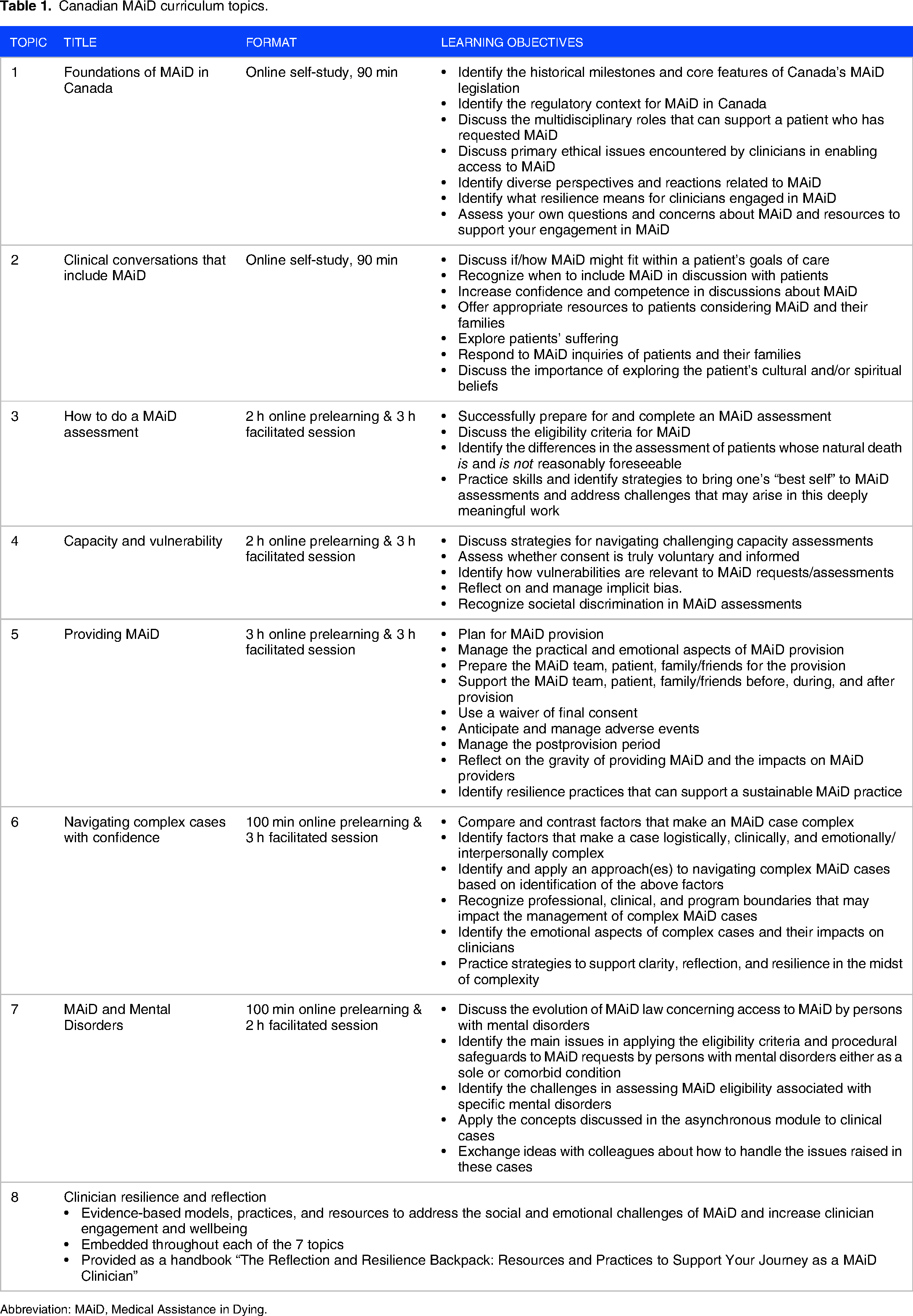
Abbreviation: MAiD, Medical Assistance in Dying.
Piloting and modifications to the CMC
To evaluate and finalize the CMC content, each of the modules (with associated reflection and resilience components) underwent pilot testing. The goals of this pilot were to determine the extent to which each module was meeting its intended outcomes and the needs of its intended users; and to determine its value, usability, and feasibility. In the pilot, learners were both current MAiD practitioners and MAiD naïve clinicians at various career stages, from both English and French-speaking regions, serving a range of patient populations, recruited through CAMAP and Steering Committee partners.
An outcome-based, mixed-methods curriculum evaluation took place from December 2022 and August 2023, and included pretopic and post-topic surveys by participants and focus groups with PWLE. An average of 61 pilot testing learners participated in each module, completing premodule and postmodule surveys to determine utility, organization, appearance, flow, and helpfulness, comfort and confidence with the material, and significant changes in their knowledge. A focus group of PWLE was also conducted for each online module. The focus group included between 4 and 6 individuals with a range of relationships to a person who had requested or received MAiD (eg, parent, partner, or friend). The PWLE were given access to the modules prior to the focus group for review. The chair of the working groups for each module led the PWLE through an overview of the online material only. After this, they participated in a group discussion, wherein they were invited to describe their perceptions about the content and helpfulness of the module for healthcare providers, and provided feedback on the content, look, and feel of the modules. These data sources were triangulated in a final evaluation report for each module. The content of the CMC was finalized and made available to learners in September 2023.
Delivery of the CMC
The CMC's target audience is any and all licensed medical or nursing practitioners, new MAiD clinicians interested in learning about MAiD assessment and delivery, and members of the current MAiD workforce who may wish to update or enhance their skill sets. The CMC is therefore a valuable learning activity for physicians or nurse practitioners who may be directly or indirectly involved in MAiD, and may in the future be available for other healthcare providers (eg, pharmacy, psychology, and social work) with an interest in learning more about MAiD.
The online platform used for delivery of the CMC modules is the Health Sci Ed Connect Desire2Learn system, hosted and maintained by the Office of Professional Development and Educational Scholarship at Queen's University, 29 as contracted by CAMAP. Access to the CMC will be available via the CAMAP website, and will be advertised through the online CAMAP communities of practice, as well as through direct communications from the organizational memberships of the National Steering Committee. Registration will remain free until March 2026 (2.5 years after hard launch), and learners will be granted access for 1 year from the time they register, during which time they can complete modules at their own pace.
Modules can be undertaken individually or together for a total of 13 h of online self-study and 14 h of facilitated sessions. Participants may select specific modules of interest for completion, though they are encouraged to complete the entire curriculum. Modules 1 and 2 are online self-studies, while modules 3 through 7 have a required online prelearning component followed by a facilitated session taught by MAiD educators (available online or in-person). Facilitated sessions will be available in each province, with regions encouraged to request and organize locally facilitated sessions.
Implementation and evaluation
The plan for dissemination of the CMC was informed by a Scoping Review and Environmental Scan of Continuing Medical Education Best Practices. The Environmental Scan included a literature review and key informant interviews with continuing medical education experts on successful strategies for encouraging participation in continuing professional development. Findings from these activities were synthesized into an Implementation Toolkit, which may be disseminated through the project's invested partners to support the uptake of the CMC in healthcare settings across Canada.
The Implementation Toolkit highlighted strategies for organizations to encourage participation within specific target audiences: current MAiD practitioners; prospective MAiD practitioners; healthcare providers who may discuss MAiD with patients; palliative care practitioners; psychiatrists and other Mental Health Professionals; francophone and Quebec anglophone participants; and interested physician or nurse practitioner trainees. The Implementation Toolkit also includes a checklist for an organization to assess its readiness to implement the CMC training, as well as template emails, flyers, and social media posts for distribution.
Website analytics tools, as well as a registration survey that inquires how learners heard about the CMC, will assist in evaluating the relative success of various communication strategies.
Engaging clinician learners to become CMC faculty through “Train the Trainer” sessions is part of the ongoing implementation strategy. Train the Trainer sessions are available to physicians and nurse practitioners who complete portions of the curriculum for modules that they wish to teach, and have the necessary experience, interest and skillset.
In addition to the formative pilot evaluations to refine the development of the CMC, long-term success also relies on demonstrating its effectiveness at improving accessibility and consistency of MAiD care and addressing the recognized gap in healthcare systems. Therefore, in alignment with SQUIRE-EDU standards, the CMC includes an outcome evaluation framework to evaluate its impact on clinician knowledge and MAiD practices and measure broad-scale system-level impacts of delivery of the CMC. A combination of prospective and retrospective data collected through healthcare provider surveys and the federal MAiD reporting database will be used to determine the impact of the CMC on clinical care (Figure 2).

CMC evaluation framework.
Discussion
The CMC was rigorously developed and offers a standardized, accredited, bilingual, hybrid curriculum for delivering MAiD in Canada. In Canada, there is no required training for physicians and nurse practitioners prior to assessing or providing MAiD. The CMC also is not a required prerequisite but is encouraged for interested healthcare providers. This curriculum currently aims to benefit physicians and nurse practitioners with potential broad impacts on improving learners’ knowledge, skills, and confidence through providing accessible, standardized, and rigorous training in the relatively new practice of MAiD. In the future, allied healthcare providers (eg, pharmacy, psychology, and social work) may also benefit from participating in the CMC given their important role in MAiD practice. 30
Particularly given the evolution of MAiD policy in Canada,2–4 and potential changes in the future (eg, MAID where mental disorder is the sole underlying medical condition or advanced requests), 31 the CMC also offers the potential of providing an added layer of quality by enhancing the skillset of MAiD clinicians. It is possible that a greater emphasis on healthcare providers’ knowledge, training, and preparedness in MAiD will also translate into the general public having greater confidence in the practice of MAiD in Canada. However, similar to other accredited curricula, 32 we anticipate the challenge that the CMC may face in attracting and ensuring wide curriculum participation in an already busy target population with a demanding schedule.
One challenge in the development of the CMC was creating the knowledge base while anticipating evolving legislation, with ensuant limited clinical experience or research evidence in the Canadian context. As a result, some of the developed curriculum had to rely on expert opinion rather than a large evidence-base of best practices. This was particularly relevant to module 4 on assessing capacity and vulnerability and module 7 on MAiD and mental disorders. To address this, the modules clearly indicate the level of evidence and, where applicable, the need for greater evidence to substantiate the information presented. Areas with a paucity of evidence are important foci when updating future CMC iterations, as greater research becomes available. Relatedly, the complexity of the topic of assisted dying15,33–35 and diverse perspectives on MAiD in Canada among experts13,36–38 means that reaching a consensus in developing the CMC was not always possible. A clear governance structure (see Figure 1) made escalation of concerns and decisions possible and reduced deadlock; this is an important takeaway for other curricula development programs where the subject matter is debated or novel.
In the curriculum, the CMC uses realistic and relatable case examples throughout its teaching, with one module (ie, module 6: “Navigating Complex Cases with Confidence”) focusing on attending to complex cases. Nevertheless, this training may have shortcomings similar to other curricula that uses didactic learning to support clinical proficiency. As Gewarges et al 39 write, “[d]idactic education about the medical and legal domains of MAID alone is insufficient to support learners’ needs. Experiential case-based learning with supervisory support has the potential to enhance training in end-of-life care in general, and specifically in MAID”. While the CMC is an important step forward in the standardization of MAiD medical education and professional development, further experiential training would beneficially complement completion of the CMC.
A unique strength of the CMC was the design of weaving the eighth CMC topic on clinician resilience and reflection into each of the 7 modules rather than leaving it as a stand-alone module. This information is particularly important given the specific interpersonal, financial, and professional challenges clinicians experience in providing MAiD. 40 Reflective practice allows learners to engage in a process of self-questioning and evaluation of their clinical experiences in order to promote greater self-understanding, professionalism, and improved patient care. 41 There are a handful of reflective guides that have been developed to support providers in being introspective to improve their MAiD practice.30,42 Incorporating clinician resilience and reflection in the CMC is critical to help healthcare providers evaluate their moral position and prepare them for practice.
Limitations
There are limitations to the development process and the CMC, mainly related to representation of diverse groups. Involvement of PWLE, such as caregivers and family members of patients who had received MAiD, was limited during the development process. While PWLE had the opportunity to review the CMC and participate in focus groups prior to the CMC's hard launch, the primary focus of piloting was on ensuring inclusion of a broad base of English and French clinicians, as representative of the primary target audiences for the CMC. Despite best efforts, there was limited representation from disability community groups and national palliative care groups, as both groups declined to participate. Nevertheless, several individual palliative care clinicians were involved at various levels, and a large palliative care center was involved on the National Steering Committee. The CMC was also successful in engaging some representation from Indigenous communities and chronic pain groups.
The CMC was developed in advance of the establishment of best practice standards, and with limited evidence-based research to guide the curriculum content, although several CAMAP guidance documents were used. Curriculum content was therefore primarily based on existing clinical practice, CAMAP's previous multiyear experience in half-day MAiD education and training workshops, feedback from attendees from CAMAP's educational webinars, symposia, and conferences, and the needs assessment. 19 Future standards and guidelines will support the iterative refinement of the CMC.
Conclusion
This article described the process of developing a comprehensive, nationally accredited, bilingual, hybrid curriculum on MAiD in Canada. The 7 modules within the CMC were purposefully developed and guided by constructivism and adult learning theory frameworks, and the 5 guiding principles that emerged from the needs assessment and consultation with invested partners. Throughout the development of this curriculum, numerous partners were engaged and consulted, and the needs and contexts of diverse learners were at the forefront.
The CMC was created with sustainability in mind, which is especially important given the evolution of MAiD policy and services in Canada. The CMC is currently being assessed and adapted based on feedback during phase one of the implementation. This work is being completed by a newly established CAMAP “Curriculum Review Committee,” which has established terms of reference, membership, and a work plan. Ongoing evaluation of the CMC will support modifications and revisions to ensure it continues to meet the needs of learners as legislative and clinical landscapes evolve.
Footnotes
Acknowledgments
We thank the members of the Canadian MAiD Curriculum Development Committee, the project's National Steering Committee, all working group subject matter experts, CAMAP’s provincial/territorial advisory council, and persons with lived experience from across Canada who contributed to the development of the curriculum.
Declaration of conflicting interests
Authors and institutions report honoraria and payment for their work on this project. ML also reports payment for providing expert testimony related to MAiD. All other authors declare no other conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CMC Project was funded by the Health Care Policy and Strategies Program of Health Canada. The views expressed in this paper are those of the authors and do not necessarily reflect those of Health Canada.
Authors’ Contributions
GKS, KH, HB, ND, AAP, SS, AS, SG, GG, and ML were responsible for conceptualization and drafting of this manuscript as well as supporting the evaluation of the CMC. JM and MSS were involved in the development and revision process of the CMC. SG, GG, and ML were responsible for developing the CMC and funding acquisition. All authors reviewed and provided feedback on the final manuscript. All authors approve the final manuscript version.
Ethical Approval
All evaluation activities referred to in this article were approved by Queen's University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (File #: 6037011) and the University Health Network Research Ethics Board (REB #22-5225.0.1).