
Abstract
OBJECTIVE
Determine if a longitudinal point-of-care ultrasonography (POCUS) elective for medical students is effective in improving POCUS knowledge.
METHODS
We share the format of our longitudinal POCUS elective for medical students. To evaluate the efficacy of our longitudinal elective, we compare the difference between pre-elective and post-elective scores on a POCUS test using a paired t-test with threshold of statistical significance of p ≤ .05. We also share the results of a post-elective survey evaluating the effectiveness and quality of the longitudinal POCUS elective.
RESULTS
Pretest mean score was 56.3% (σ = 13.6), while posttest mean score was 73.3% (σ = 9.4), with an average score improvement of 17.0% (95% CI 9.9-24.0%, p < .0001). All students strongly or moderately agreed that they would recommend the elective to future medical students, that they were more confident with their POCUS skills after completing the elective, that the time commitment of the elective was appropriate, and that they felt they had the time to fit the elective into their schedule as a medical school student. Most students (56.7%) strongly or moderately agreed that the knowledge gained from the POCUS elective had helped them in their clinical rotations.
CONCLUSIONS
Our longitudinal POCUS curriculum subjectively and objectively improves medical students’ POCUS knowledge while remaining accessible to students. We share our unique longitudinal POCUS elective curriculum, the format of which and its benefits are transferable to other medical schools. Through this, we hope to provide others with ideas on how they may implement a longitudinal POCUS elective.
Introduction
Point-of-care ultrasonography (POCUS) has become an invaluable tool across many medical specialties and, as a result, is becoming increasingly prevalent in medical training. POCUS training is required for Accreditation Council for Graduate Medical Education in a few medical specialties. 1 With this shift towards POCUS use in clinical practice and residency training, many medical students now view POCUS training as an essential component of their education. 2 Medical schools have responded to this demand, and the number of medical schools providing POCUS training has more than doubled in the last decade. 3 In 2021, 73% of surveyed U.S. medical schools had some degree of POCUS training available to medical students. 4 The number of medical schools offering POCUS training has continue to grow since then. 5
Medical schools have used various approaches to POCUS education. The instructors used for the delivery of POCUS education varies but typically consist of clinical faculty, residents, fellows, medical students and/or sonologists. 5 While some institutions offer a POCUS elective, it is more common for POCUS curricula to be required, especially during the pre-clinical years of medical school.5,6 Many schools with required POCUS curricula include POCUS teaching as part of other pre-clinical courses (commonly anatomy, physiology, or physical examination teachings). Others integrate POCUS curricula into clinical rotations or require completion of a stand-alone POCUS course. 7 Medical schools tend to provide more POCUS education during the pre-clinical rather than clinical phase, although it can be offered any time throughout medical school.5,7 Despite the growing incorporation of POCUS in undergraduate medical education, only a minority of medical schools have implemented longitudinal POCUS education in their curriculum.5‐7
Still, a common issue faced by medical schools in implementing or expanding POCUS training is finding the time in already demanding and busy curricula. 7 At medical schools with some POCUS training already in place, students may feel that the time allotted for POCUS education is not enough to provide them with the proficiency that they are expected to have for clinical rotations and for residency. Also, institutions may struggle to find clinicians who can step away from clinical practice to teach POCUS to medical students. The costs associated with obtaining POCUS equipment also poses a barrier to many medical schools that are considering increasing POCUS education. 7
At our institution, the required curriculum for all students currently consists of five two-hour ultrasound sessions during their anatomy course and a one-hour lecture on POCUS followed by a one-hour scanning session during their nephrology course. Many medical students at our institution desired further ultrasound experience, so medical students have partnered with a faculty member to design and implement a POCUS elective. We have purposely designed this elective to occur longitudinally over the course of six months for several reasons. First, longitudinal electives (ie occurring over several months rather than a shorter block of time) have been shown to enhance medical student education, 8 and the authors of this study had noted that preexisting longitudinal electives were a success at our school. Moreover, the unique longitudinal format of our POCUS elective addresses several of the aforementioned barriers to POCUS education.
In this paper, we outline the format of our longitudinal POCUS elective, present data on students’ POCUS knowledge before and after the elective and share student feedback on the elective. Our hypothesis was that implementation of longitudinal POCUS elective would be effective in expanding students’ knowledge and comfort with POCUS while mitigating the barriers that commonly prevent medical students from participating in an elective (eg, time, scheduling conflicts). Our primary outcome was the change in medical student participants’ POCUS knowledge as assessed by a pre-/posttest following completion of elective. Secondary outcomes included participant satisfaction and demonstration of usefulness of the skills learned during the elective in clinical clerkships. Our hope is that this paper may provide a framework for other medical schools and residency programs that wish to start or expand POCUS training in their curricula.
Methods
The reporting of this study follows the STROBE guidelines (Supplementary File 1). 9 This observational study occurred at the Mayo Clinic in Rochester, Minnesota from May 2021 to October 2023. The POCUS elective curriculum is comprised of 20 educational hours spread over six months and is open for up to 30 s-year students to participate. Our medical school has a 1.5-year preclinical curriculum prior to beginning clinical rotations, so the second-year students who take the elective are finishing their preclinical training and transitioning to their clinical training. This timeline is designed to prepare students to use POCUS during their clinical rotations. Students who complete the elective earn elective credit which counts towards a graduation requirement.
The curriculum consists of two hours of instructional videos (Appendix 1) on the basics of POCUS including organ-specific (ie renal, cardiac, gallbladder, lung) scanning and anatomy to be viewed prior to the first group session, three three-hour group sessions (Table 1) in the Mayo Clinic Multidisciplinary Simulation Center (MCMSC) where students learn and practice POCUS on persons employed as simulated patients, and nine hours of clinical experience when students perform POCUS on patients alongside a physician during real clinical encounters. In selecting the pre-course videos, we reviewed several instructional POCUS videos and selected those that were freely accessible, that were appropriate for medical students new to POCUS, and that would be applicable to the Simulation Center and clinical sessions.
Overview of each POCUS elective simulation-based group session. The three sessions are spread across approximately six months. Each session is held twice to allow for smaller group sizes. In addition to these group sessions, the curriculum includes POCUS educational videos for independent study and POCUS clinical experience.

The elective is organized, led, and annually updated by two-to-four student elective leaders and a faculty leader. Elective leaders have completed the elective the year prior and receive elective credit for leading the elective. The faculty leader uses personal time to lead the group sessions. The faculty leader and four other faculty members provide the instruction during the clinical experiences, which occur during regular clinical activities without additional full-time equivalent (FTE) allotment for teaching. The MCMSC gives open access to approved courses without charge. The persons serving as simulated patients during group sessions are employed by the MCMSC. Ultrasound scanners are available in the MCMSC (portable scanners on wheels) and the clinical areas for ordinary clinical use (portable scanners on wheels and hand-held scanners). No purchases have been necessary for this elective as the Simulation Center at our institution, including the persons serving as simulated patients, can be used without direct cost to educators. Therefore, the elective requires no funding, and there is no budget.
For each of the three group sessions, two different evening sessions are offered, and students can attend either based on their schedules. Group sessions are deliberately held in the evenings to minimize scheduling conflicts for medical students and elective instructors. Group sessions are limited to 12–16 students and are instructed by the three medical student elective leaders and the faculty leader, making the student to instructor ratio 3-4:1 during the first and third group sessions. An emergency medicine physician is present for the second session, making the student to instructor ratio 2-3:1. Groups of 3-4 students are paired with one instructor and practice at stations that each contain an ultrasound machine and a simulated patient to practice scanning on. An overview of each group session is provided in Table 1.
In the first group session, students are provided an overview of the elective and complete an image-based examination (herein referred to as the “pretest”) to establish baseline competency in common POCUS anatomy and pathology (Supplementary File 2). Following completion of the pretest, students learn the common indications for POCUS, how to operate an ultrasound machine, and practice obtaining POCUS images on simulated patients. Organs scanned on simulated patients include the heart, lung, gallbladder, liver, kidney, and bladder.
During the second group session, students learn how to use POCUS to assess a trauma patient using the Extended Focused Assessment with Sonography in Trauma (E-FAST) exam. The session begins with a large-group teaching given by an emergency medicine physician on the E-FAST indications and ultrasonography views. Next, students divide into small groups of 3-4 and practice the E-FAST exam on simulated patients with guidance from the elective leaders while the emergency medicine physician and faculty POCUS educator supervise.
The third and final group session consolidates knowledge acquired from the previous two group sessions and knowledge gained in students’ interim medical school coursework. Students in groups of 3-4 are presented with clinical case vignettes which include a thyroid nodule, cardiorenal syndrome, benign prostatic hyperplasia, and cholecystitis. Students ask targeted questions to the instructor presenting the case about pertinent medical history, physical exam findings, and laboratory result. Each case utilizes POCUS to make or support a diagnosis. The students scan the standardized patients, and after optimal views of the organs in question are obtained, the students are shown the corresponding pathologic POCUS findings for the case vignettes on a separate computer screen. For example, after scanning the normal gallbladder of the simulated patient during the cholecystitis case, students are shown a POCUS image containing gallstones, gallbladder wall edema and pericholecystic fluid. Students work through all four of the cases. After the case vignettes, students take the posttest, which consists of the same question as the pretest, and a post-elective survey (Supplementary File 3). The survey aims to obtain feedback regarding the elective and contains five questions that students answer using a five-point Likert scale (strongly disagree to strongly agree) and five open response questions. The session concludes with a group reflection on the elective where students provide additional verbal feedback. Finally, students are recruited to serve as elective leaders for the following year's elective.
As part of the elective, students are also required to schedule two separate four-hour sessions in a clinical setting. Students are provided with a list of dates/times to work alongside physician clinical preceptors to utilize POCUS during real patient encounters. Students select dates/times based on their own availability and their clinical interests. A variety of clinical opportunities are currently available to students including the family medicine procedure clinic, nephrology hospital service, outpatient nephrology clinic, outpatient hemodialysis unit, and the rheumatology procedural clinic. One student is assigned to one clinical preceptor per session (student:instructor ratio of 1:1). During these sessions, students scan between 8–16 patients to obtain diagnostic information or perform ultrasound-guided procedures under the clinical preceptor's instruction. These sessions are designed to facilitate the transfer of skills learned on simulated patients in the group sessions to real patients during clinical encounters.
In this study, we analyze the difference between pre- and posttest data to evaluate the efficacy of our elective in teaching POCUS knowledge. Additionally, we compare the pretest scores of students who self-reported watching the assigned pre-course videos to those who self-reported that they did not watch the videos to evaluate whether the selected videos are effective pre-work for the elective. We also share the feedback obtained from elective participants who completed the post-elective survey.
This study was approved as a quality improvement/quality assessment project by the Institutional Review Board at the Mayo Clinic in Rochester, MN (ID: 23-008901). Verbal informed consent for data publication was obtained from all participants and recorded in writing before participants completed the pretest, posttest, and survey. Results of the pre- and posttests and survey data were collected anonymously. Students’ pre- and posttest scores were matched using student identification numbers. Inclusion criteria for statistical analysis of pre- and posttest data included all second-year medical student POCUS elective participants from the 2023 cohort, who completed both a pre- and a posttest, and who consented for use of both pre- and posttest score data in a research publication. Only scores from the computer-based 2023 test were included, since the previous years’ paper-based tests had suboptimal POCUS images and did not show the orientation of the ultrasound probe. Exclusion criteria for statistical analysis of pre- and posttest data included denying consent for use of either pre- or posttest score in a research publication. Inclusion criteria for sharing survey responses in this paper included all POCUS elective participants who consented for use of survey data in a research publication. Exclusion criteria for sharing survey responses included denying consent for use of survey data in research.
Statistical analysis
Statistical analysis was performed using Blue Sky Statistics v. 7.40 (Blue Sky Statistics, LLC, Chicago, IL, USA). A sample size calculation was not conducted prior to performing data analysis. Pre- and posttest data was summarized as means. The difference between pre- and posttest data was compared using a paired t-test with threshold of statistical significance of p ≤ .05 and is presented as mean score improvement with a 95% confidence interval (CI). Pretest scores of students who watched the assigned pre-course videos versus those who did not watch the assigned pre-course videos are summarized as means and were compared using a paired t-test with threshold of statistical significance of p ≤ .05.
Results
Fourteen students participated in the POCUS elective in 2021, 26 students participated in 2022, and 26 students participated in 2023. Across the three cohorts of participants, 53% were male and 47% were female. 23 of 26 (85.5%) students completed both a pretest and posttest in 2023. Pretest mean score was 56.3% (σ = 13.6), while posttest mean score was 73.3% (σ = 9.4), with an average score improvement of 17.0% (95% CI 9.9-24.0%, p < .0001) (Figure 1). Students who watched the assigned pre-course videos (n = 17, 60.3%) performed significantly better on the pretest than those who did not (n = 6, 45.0%, p = .017).

Box and whisker plot of pretest and posttest scores. Means are represented by the dashed horizontal line, medians are represented by the solid horizontal line, standard deviation is represented by the dashed rhombus, interquartile range is represented by the box, minimum and maximum scores are represented by the whisker ends.
Of all POCUS elective participants from 2021-2023, 29 students (43.9%) completed the post-elective survey. Responses and response rates to each multiple-choice question are shown in Figure 2. All students strongly or moderately agreed that they would recommend the elective to future medical students, that they were more confident with their POCUS skills after completing the elective, that the time commitment was appropriate, and that they felt they had the time to fit the elective into their schedule as a medical school student. Many students (56.7%) strongly or moderately agreed that the knowledge gained from the POCUS elective had helped them in their clinical rotations. Several students (42.3%) were neutral about whether the knowledge gained from the POCUS elective had helped them in their clinical rotations. All responses to the survey's open response questions are provided in Supplementary File 4.
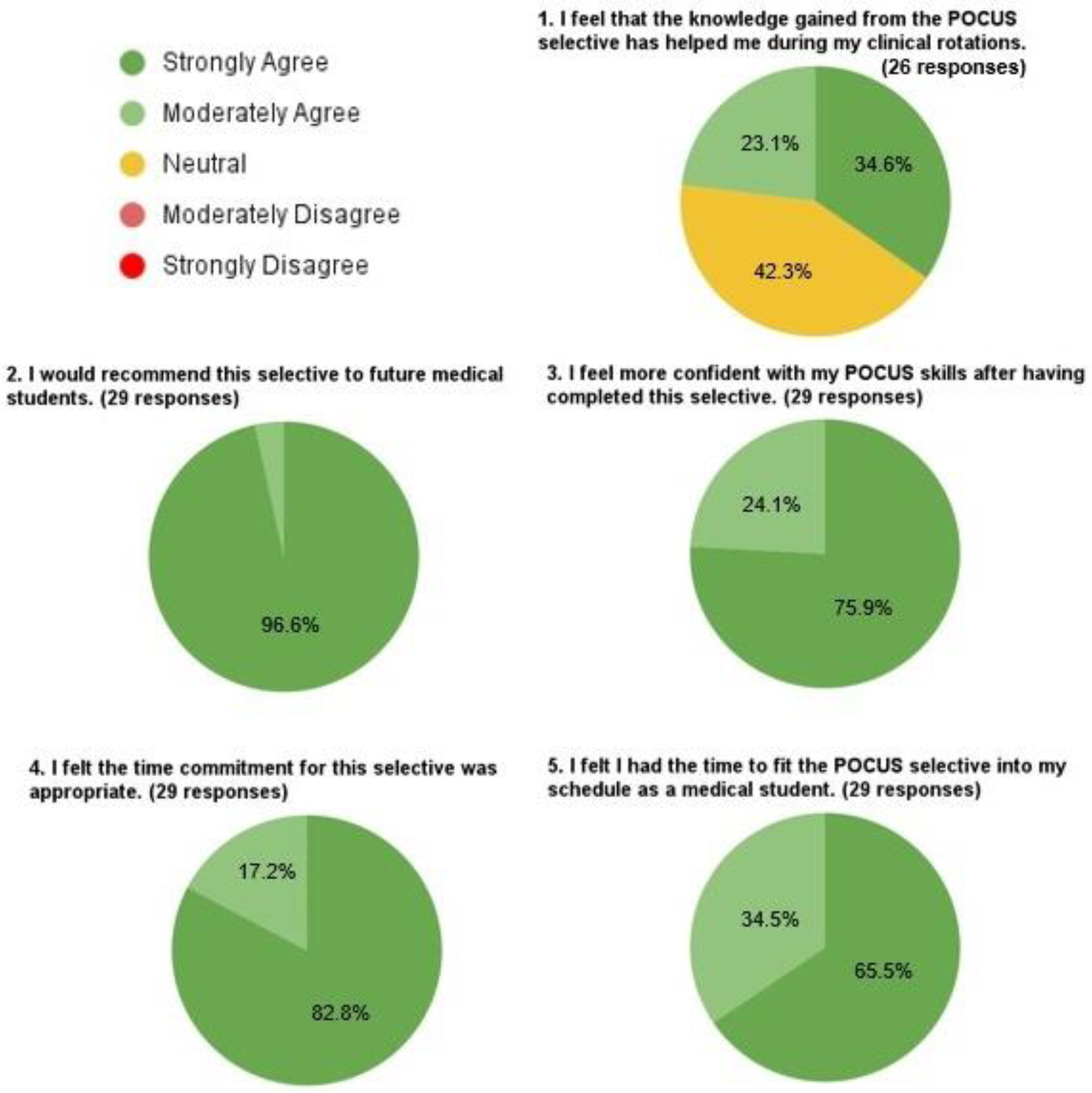
Graphical representation of student responses to the multiple-choice questions on the post-elective survey. Students answered the questions shown on a 1 (strongly disagree) to 5 (strongly agree) Likert scale. The number of students responding with each Likert score with each question is shown. Student responses to the open response questions of the survey are listed in the Supplementary File 4.
Discussion
We found that our longitudinal POCUS elective course significantly improved medical school students’ knowledge of POCUS image interpretation, as students performed, on average, nearly 20% better on a POCUS assessment after completing the course. Moreover, the post-elective survey results demonstrated that students felt the elective is accessible in terms of time commitment and scheduling. All survey respondents feel more confident in their POCUS skills, and many found information gained from the POCUS elective useful in their clinical experiences. Notably, all students who took the post-elective survey would recommend the elective to other medical students.
POCUS training for medical students has demonstrated several benefits, including better physical exam skills, better understanding of anatomy, 10 and improved clinical decision-making. 11 Therefore, many medical schools are attempting to incorporate or expand POCUS training in their curricula. As discussed, several barriers exist to the expansion of POCUS education for medical students, but the longitudinal design employed for our elective overcomes many of these challenges. First, our longitudinal curriculum offers flexibility for medical students as group sessions are scheduled in the evenings to avoid schedule conflicts, and two evenings are selected for each session, allowing students to select which session they attend according to what fits their schedule. A longitudinal curriculum also provides a feasible way to add POCUS training without having to make major changes to existing curricula. Additionally, it disperses the required resources (eg ultrasound machines, standardized patient time, physician instructor time, space requirements) over many months and allows clinicians to integrate POCUS teaching into their usual clinical activities rather than protecting specific time for POCUS education, which may allow institutions to overcome a shortage of POCUS-trained faculty members. 12
Integrating POCUS instruction into usual clinical activities has had additional benefits. Studies have shown improved patient care when POCUS is utilized.13,14 Anecdotally, our clinicians have sensed improved patient care when working with students during their clinical POCUS sessions due to the emphasis on POCUS use during these patient encounters. Moreover, during the clinical experiences, internal medicine and family medicine residents and nephrology fellows may be part of the clinical team. These residents and fellows have, under the guidance of the clinical preceptor, often taught POCUS skills to and/or learned POCUS skills from the students, which we feel has contributed to expanding POCUS knowledge and use at our institution.
In addition to maximizing student participation and resource utilization, the longitudinal format of the elective is also advantageous from a learning standpoint. Like many skills, POCUS requires repeated practice over time to build and maintain proficiency. Previous work has shown that longitudinal POCUS teaching leads to better skill retention compared to stand-alone workshops. 12 Students also have the benefit of acquiring new knowledge from their other medical school classes between each group session of the elective. Students frequently comment that the new knowledge they bring to each group session from their interim studies enhances their understanding of material covered during the group sessions.
Despite these benefits of longitudinal curriculum and the large number of medical schools offering POCUS education, relatively few offer a longitudinal curriculum.5,15,16 When a longitudinal POCUS curriculum is available, medical schools generally require all students to participate rather than offering it as an elective.17‐19 To our knowledge, our POCUS elective is the among the few elective (ie non-mandatory) courses that occur longitudinally and supplement a pre-existing, required medical school ultrasound curriculum.20,21 Moreover, POCUS electives at other medical schools, when available, usually focus on ultrasound skills for a specific medical specialty (eg radiology, obstetrics, emergency ultrasound, etc). 6 On the contrary, our longitudinal POCUS elective is also unique in that it aims to teach students POCUS skills that are broadly applicable across medical specialties. While our curriculum and assessment measures are unique, they are also highly replicable. Therefore, we believe that our findings of improved POCUS knowledge and high rates of student satisfaction will be seen at other medical schools if our longitudinal curriculum is implemented.
While we received very positive feedback from our survey, it is of note that 42.3% of students who took the survey responded “neutral” to whether they were helped in clinical rotations by this curriculum. Our post-elective survey did not ask for reasons, but this likely is a result of the timing of our POCUS elective which ends during the transition to rotations when some, but not all, students have begun clinical rotations. Additionally, the frequency with which POCUS is used within a specific rotation is highly variable. Students may use POCUS daily in rotations like emergency medicine or obstetrics but may not use POCUS at all in other rotations. Thus, the large “neutral” response to the question of whether students had been helped in their clinical rotations by the POCUS elective likely stemmed from whether students had started clinical rotations and, if they had, which rotations they had completed at the time of taking the survey.
One limitation of this study is the current lack of a skill-based competency evaluation of students. We have shown our curriculum to be effective in increasing POCUS image interpretation but have not investigated if it improves student's ability to obtain POCUS images. In the future, we will consider implementing a skill-based examination. Also, the number of scans students perform during the two clinical sessions is less than what is ultimately required to become truly proficient in clinical POCUS. However, our elective is designed as an introduction to POCUS, and we believe these clinical scans are an excellent start to developing comfort and skill with POCUS outside of the Simulation Center.
Another limitation of our study is that we did not perform a power analysis to estimate the required sample size prior to performing the study. Still, we ended up with a large enough sample size and difference in pre-to-posttest scores to detect a statistically significant difference. A final limitation was that while posttest scores did show significant improvement from pretest scores, the average posttest score was still only 73.3%. There are several possible explanations for this. First, we intentionally made the test challenging, so that we could better discern improvement from pre-to-posttest. However, the test was not validated on elective participants beforehand, so it is possible that there were problematic questions or images. For example, certain test questions had POCUS views not reviewed during hands-on practice, such as testicular and musculoskeletal ultrasound findings. Additionally, many of the test questions incorporated pathology that elective participants did not see while scanning standardized patients. This could have led to lower overall test scores, as students did not have the opportunity to practice obtaining and reading these ultrasounds. In future years, we plan to gather feedback about the test from students. If they have concerns regarding the structure of specific questions, we will modify the test questions accordingly.
We additionally gained written and verbal feedback from students to further improve our elective. One common suggestion from students was to incorporate more pathology identification into our curriculum. With future cohorts we plan to incorporate an ultrasound mannequin (CAE Vimedix) which is available on our campus that can simulate many different pathologies on ultrasound into the group sessions. This ultrasound mannequin has the added benefit that POCUS views can be shown alongside anatomy renderings, which students found helpful when showing similar side-by-side images during our curriculum. Students also found the case vignettes in the third group session with their associated pathologic POCUS findings extremely valuable, so we plan to incorporate summarizing case vignettes at the end of the first and second group sessions. Students also noted that they may forget some information between the group sessions and suggested we incorporate more review material from previous sessions. In addition to increasing the amount of review material we cover during group sessions, we plan to provide a monthly POCUS Newsletter email that includes a review of previous topics covered, interesting POCUS cases, and suggested reading. Lastly, several students expressed a desire for additional sessions. Therefore, we are considering implementing an Advanced POCUS elective for students desiring more POCUS education after having completed this course.
Conclusions
In this paper, we share our unique longitudinal POCUS elective curriculum for medical school students. The longitudinal, flexible design of the elective offers many advantages in terms of accessibility, participation, resource allocation, and quality of education. Our curriculum is highly regarded by students and was associated with objective and subjective improvements in students’ POCUS knowledge. Still, we have identified several ways to improve the course further for future students. We believe that the format of our elective and its benefits are transferrable to other medical schools, and it is our hope that sharing our experience may be helpful for other medical schools looking to implement or modify existing POCUS education.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241260244 - Supplemental material for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study
Supplemental material, sj-docx-1-mde-10.1177_23821205241260244 for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study by Ethan Crispell, Malavika Nair, Max Giesken, Molly O’Shea, Michael Sischka, Larry Liu, Jonika Weerasekare and James Gregoire in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205241260244 - Supplemental material for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study
Supplemental material, sj-docx-2-mde-10.1177_23821205241260244 for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study by Ethan Crispell, Malavika Nair, Max Giesken, Molly O’Shea, Michael Sischka, Larry Liu, Jonika Weerasekare and James Gregoire in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205241260244 - Supplemental material for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study
Supplemental material, sj-docx-3-mde-10.1177_23821205241260244 for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study by Ethan Crispell, Malavika Nair, Max Giesken, Molly O’Shea, Michael Sischka, Larry Liu, Jonika Weerasekare and James Gregoire in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205241260244 - Supplemental material for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study
Supplemental material, sj-docx-4-mde-10.1177_23821205241260244 for A Longitudinal Elective Facilitates Point-of-Care Ultrasonography Education for Medical Students: An Observational Study by Ethan Crispell, Malavika Nair, Max Giesken, Molly O’Shea, Michael Sischka, Larry Liu, Jonika Weerasekare and James Gregoire in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We thank the staff and simulation patients of the Mayo Clinic Multidisciplinary Simulation Center for facilitating the POCUS simulation group sessions.
Author contributions list
Study concept: LL, JW, JG
Study Design: LL, JW, JG
Statistical analysis: MS, EC, MN, MG, MS
Drafting of paper: EC, MN, MG, MO, MS, JG
Editing of paper: EC, MN, MG, JG
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
No funding was received to conduct the study. If accepted, the article processing charge will be covered by the Mayo Clinic Division of Nephrology & Hypertension's allowance for research publications. The authors received no financial support for the research, authorship, and/or publication of this article.
Consent
Verbal informed consent for data publication was obtained and recorded in writing from all participants prior to all data collection. Data from participants who denied consent for data publication was excluded.
Ethical committee
This study was approved as a quality improvement/quality assessment project by the Institutional Review Board at the Mayo Clinic in Rochester, MN (ID: 23-008901).
Supplemental material
Supplemental material for this article is available online.
Appendix 1. Pre-Elective POCUS Educational Videos
POCUS Geek. Ultrasound Physics. Published 26 September 2016. Accessed 26 November 2023.
POCUS Geek. POCUS – Basic Renal Ultrasound. Published 14 December 2018. Accessed 26 November 2023.
https://www.youtube.com/watch?v=Pw60zHMKTWo&list=PLMoMZ6 POCUS Geek. Bedside Ultrasound Basic Cardiac US. Published 26 September 2016. Accessed 26 November 2023.
POCUS Geek. POCUS: Lung Ultrasound - Basic Anatomy and Lung sliding - Updated - second Edition. Published 15 August 2023. Accessed 26 November 2023.
POCUS Geek. POCUS - Gallbladder Ultrasound Anatomy. Published 31 December 2018. Accessed 26 November 2023.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.