
Abstract
OBJECTIVES
Self-directed learning (SDL) competency is important for physicians to stay abreast of advances in their field and to provide the best available evidence-based care to their patients. Therefore, an essential responsibility of medical educators is to ensure the development of SDL skills in their students. The first objective of this study was to investigate longitudinally the degree to which medical students were ready to engage in SDL. The second objective was to examine students’ perceptions of their SDL development throughout training.
METHODS
A 2-part study of preclinical and clinical medical students was carried out at a midwestern U.S. university. In Study A, a longitudinal assessment of preclinical medical students’ readiness to engage in SDL was conducted by administering an SDL readiness survey (SDLRS). In Study B, third- and fourth-year medical students were asked to reflect on their SDL development, in addition to completing the SDLRS.
RESULTS
After validating the Hendry and Ginns version of the SDLRS in preclinical medical students during Study A, we found that 3 of the 4 subscales remained constant over the 3 iterations of the survey while the self-determination subscale increased significantly between the first and third iteration of the survey. In Study B, an analysis of the clinical medical students’ comments indicated a perceived increase in their SDL abilities and a growing appreciation of SDL. However, the SDLRS scores of clinical students did not differ from the results observed in preclinical students in Study A.
CONCLUSIONS
The results of the SDLRS indicated that the experience of students in our medical school has a positive influence on self-determination by the end of the preclinical years. Furthermore, analysis of the reflections of clinical students indicated ongoing development of SDL skills throughout their medical school training that were influenced by a wide range of experiences.
Introduction
One of the many challenges faced by healthcare providers is the need to stay up to date with medical advancements to provide evidence-based patient care. 1 The Liaison Committee for Medical Education (LCME) recognized the need to address this challenge when it added the requirement for medical schools to incorporate self-directed learning (SDL) activities into curricula. 2 The COVID-19 pandemic magnified this challenge, as seen by rapidly changing recommendations for prevention, diagnosis, and treatment.3,4 The volume and pace at which new medical knowledge becomes available underscores the critical need for physicians to maintain their professional competence by identifying their own learning needs, finding credible sources of information, and adapting their approach to patient care based on the best available evidence.1,5 Therefore, it is essential that medical schools provide training to develop the SDL skills that physicians must integrate into their practice over the course of their careers.
The concept of SDL, putting the responsibility of the learning process on the individual, has been around for decades and has been described in several ways. Candy provided a useful framework of SDL by defining it as a triad of autonomy, autodidaxy, and learner control. 6 Knowles described SDL as a process in which the individual takes the initiative by assessing their own needs, creating goals, and developing learning strategies on their own instead of relying on others to direct their educational needs. 7 Grow proposed a 4-stage model of SDL based on the degree of teacher versus learner control. 8 In situations where the teacher is the “sage on the stage,” students are dependent on the dissemination of knowledge from the instructor and have little control over their own learning goals. At the other end of the scale, self-directed students set their own goals and benefit from having teachers serve as facilitators or consultants who “guide on the side.” Hiemstra and Brockett proposed an SDL model that takes into consideration 3 main elements: (1) the personal attributes of the learner, (2) the process which involves the teaching-learning transaction, and (3) the context which encompasses the environmental and sociopolitical climate. 9 Others have shown that educational, cultural, and familial environments influence the ability of students to take ownership of their learning.10,11 Ricotta et al reported on the outcomes of the 2019 Millennium Conference, devoted to SDL in medical education, at which invitees described 4 factors that expanded on an SDL model originally proposed by Garrison.12,13 The revised model includes factors that are important for institutions to foster SDL in medical education: (1) the institutional environment, (2) personal attributes of the trainees, (3) assessment of SDL, and (4) pedagogy and faculty development.
The LCME does not specify how medical schools should incorporate SDL activities into their curricula. Medical schools utilize many educational approaches in both preclinical (lecture, problem-, team-, or case-based approaches) and clinical (in-patient, out-patient, surgical, rural preceptorships, research, etc) segments of the curriculum. While SDL is naturally inherent in some of these formats,14–16 SDL activities must be intentionally designed and implemented in other formats such as lecture-based courses. 17 Numerous studies have demonstrated that SDL activities can be incorporated in a variety of medical educational settings.18–20 Regardless of the educational setting, the degree to which students define their learning goals varies with the method of content delivery.21–24
We previously published a study in which student reflections provided valuable information on how an SDL activity affected their perception of their SDL skills. 20 Themes identified in the qualitative data revealed that students perceived the SDL activity as a valuable learning experience which contributed to the skills they associated with development as a clinician. We had assumed that medical students matriculated as adult learners with competence in SDL. However, our previous research also indicated that first-year medical students recognized the need to further develop their SDL expertise. These findings were consistent with other studies that have described variability in the SDL readiness of students in health professional programs.23,25 To gain a greater understanding of the development of SDL readiness throughout the preclinical years of our medical school, we designed a longitudinal study that tracked individual students. This approach provided insight into the magnitude and direction of the students’ SDL development over time.
The first goal of the current study was to investigate the degree to which our students were ready to engage in SDL and whether their readiness scores changed throughout training. The second goal was to examine clinical students’ perceptions of their SDL development. In Study A, we used the Hendry and Ginns Self-Directed Learning Readiness Scale (SDLRS) 26 to assess the readiness of preclinical medical students to engage in SDL over time. In Study B, clinical students were assessed for their SDL readiness at a single time point and were also asked to reflect on their SDL development and factors they considered to be important contributors. Using a multimethod approach, we gained insight into SDL readiness and development in medical students over time.
Materials and Methods
Survey
We used the Hendry and Ginns SDLRS, a modified version of the SDLRs developed by Fisher, which was validated by Hendry and Ginns for medical students.26,27 The modified SDLRS used in the study was obtained directly from Hendry with permission to use granted by email on March 17, 2019. The modified SDLRS consisted of 35 items based on a 5-point Likert scale (strongly disagree, disagree, unsure, agree, and strongly agree). The SDLRS includes the following 4 subscales: critical self-evaluation, learning self-efficacy, self-determination, and effective organization for learning. Additionally, we collected student demographic information including biological sex, age, education level, and prior research experience.
Study Design
The studies described in this publication were conducted in accordance with the ethics guidelines of the University of Oklahoma Health Sciences Center and were approved by the Institutional Review Board (IRB #11972 on April 24, 2020 and IRB #9518 on July 28, 2018). Students included in these studies received medical school training at the University of Oklahoma College of Medicine, which provides 2 years of didactic, preclinical instruction followed by 2 years of clinical training.
Study A
In this study, we measured the SDL readiness of medical students in the College of Medicine at the University of Oklahoma Health Sciences Center (Classes of 2022 and 2023) at 3 time points: matriculation, the end of the first year, and the end of the second year. These students were invited to take the SDLRS during matriculation. The survey was administered to students using REDCap electronic data capture tools hosted at the University of Oklahoma.28,29 The consent form was included as part of the survey. Only students who signed individual consent forms were included in this study. Students who did not sign consent or who failed to complete all iterations of the survey were excluded. No other exclusion criteria were applied. To assess the internal consistency of the survey questions at the initial time point (matriculation), we calculated Cronbach's alpha. Cronbach's alpha provides an estimate of the extent to which the items in a scale or test are related to each other and thus can be used to assess the internal consistency of the scale or test. Each student was assigned a unique identifier to facilitate longitudinal analysis of matched data. Email invitations to participate in the second and third iterations of the survey were only sent to students who had completed the first iteration (Table 1).
Study A—Administration of SDLRS preclinical survey.
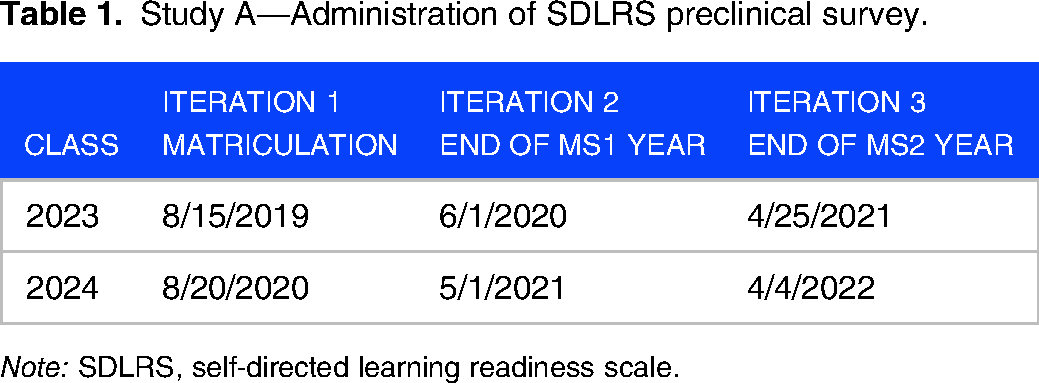
Note: SDLRS, self-directed learning readiness scale.
Study B
In this study, third- and fourth-year medical students (clinical years) in the College of Medicine at the University of Oklahoma Health Sciences Center (Classes of 2021 and 2022) were assessed for SDL readiness and development at the end of a 2-week directed-readings course. This was a new course created during the COVID-19 pandemic to continue clinical education for students removed from rotations involving direct patient care. The course was offered every 2 weeks during the 2020-2021 academic year. At the end of the course, students answered 2 open-ended questions and completed the SDLRS. The survey was administered to students through the D2L learning management system, with the consent form included as part of the survey. Only students who signed individual consent forms were included in this study. No other exclusion criteria were applied.
Students were asked to respond to the following open-ended questions: (1) Please reflect on how your knowledge, skills and attitudes toward SDL developed during medical school. Include specific examples of changes you have seen in your SDL and (2) Please describe the experiences that contributed the most to the development of your SDL knowledge, skills and attitudes. A 3-person analysis team, with prior experience in qualitative research methods, performed a thematic analysis 30 of the data using Dedoose Version 9.0.62 software. This software is designed for managing and analyzing qualitative and mixed-method research data (Los Angeles, CA: SocioCultural Research Consultants, LLC). The analysis team met 8 times over a period of 4 months to review the data, compare findings, and reach consensus on codes and themes. The initial code set was based on codes identified in a study by Hill et al 20 that evaluated an SDL activity in first-year medical students. After independent coding, we compared findings and agreed on the codes that described the data in the current study. We created operational definitions for each code and cycled back through the data to check for consistency. As we developed the final code set, we eliminated any codes not strongly iterated across the data and merged codes that conveyed concepts with similar meanings. We continued a process of constant comparison to discover relationships across codes and to identify themes that captured the essence of the coded statements. Sample statements were selected for inclusion in this manuscript that were representative of the code meaning and operational definition. Cross-checking among analysts, including a review of the codes, sample statements, and themes, ensured the credibility of the analysis process.
Quantitative data analysis
We used IBM SPSS Statistics 28.0.0.0© to analyze survey data as well as descriptive statistics to characterize participant demographics. For the validation study, we calculated and reported means, standard deviations (SD), median inner-quartile values (IQR), and minimum and maximum values of the survey subscales. Cronbach's alpha was used to confirm the internal consistency of the data collected from the first iteration. In study A, we calculated the mean and standard deviation for Likert scale responses for each of the 4 subscales across participants over 3 iterations. A one-way repeated measures analysis of variance (ANOVA) with Bonferroni adjustment for multiple comparisons was used to compare across survey iterations. To further examine differences observed in the ANOVA, we used a one-tailed t-test across survey iterations. In study B, we used Student's t-test to compare mean Likert scale responses in each of the 4 subscales between preclinical and clinical students.
Results
Study A
The main objective of Study A was to assess the development of SDL readiness in preclinical students at 3 time points during the first and second years of medical school. In Survey Iteration 1 (N = 313), 53.4% of respondents identified as male and 45% identified as female while 1.6% did not identify their sex. The percentages of male and female respondents remained constant during Iterations 2 and 3. The average age was 24 years (SD = 3), the median age was 23, and the ages ranged from 20 to 40 years.
SDLRS validation study
Cronbach's alpha scores between .66 and .79 were obtained in all subscales, falling within the acceptable range for the purpose of this study (Table 2).
Study A—Validation of SDLRS (N = 313).

Note: SDLRS, self-directed learning readiness scale.
Longitudinal SDLRS
The SDLRS was administered at 3 time points during the first 2 years of medical school: matriculation, end of the first year, and end of the second year. In the first survey iteration, the mean scores for the SDLRS subscales ranged from 3.5 to 4.4, with self-determination scoring the lowest and learning self-efficacy scoring the highest (Table 3). These results were similar in the second and third survey iterations, except for the subscale self-determination. ANOVA results indicated a significant effect of time, with Wilks’ Lambda = 0.90, F(2, 72) = 8.18, p < .05, and partial eta squared = 0.102. Pairwise comparisons of the survey iterations revealed a significant difference in self-determination score, p < .01, between the first and third iterations. When we factored in sex, we saw a statistically significant increase in the scores for self-determination. For males, the increase occurred (p < .05) between the first and second iterations, and remained constant between the second and third iterations. For females, the increase was seen between the first and third iterations (p < .001). In the third iteration, there was no statistical difference between males and females (p = .12). We found no statistical difference across iterations due to age, year of education, or prior research experience.
Study A—SDLRS scores in preclinical students.

Statistically significant compared to Survey Iteration 1, p < .01.
Note: SDLRS, self-directed learning readiness scale.
Study B
The main objective of Study B was to explore students’ reflections on their SDL development during medical school. In this study (N = 62), 33.9% of respondents identified as male and 66.1% identified as female; 66.1% were third-year and 33.9% were fourth-year students. The average age was 27 years (SD = 2.4), median age was 26, and the ages ranged from 22 to 37 years.
SDLRS preclinical versus clinical
We investigated the impact of clinical training on student responses to the SDLRS. Due to COVID-19, we had the opportunity to collect SDLRS data from a subset of clinical students in either the third or fourth year. The data collected from these students were not linked to the longitudinal data collected from students in Study A. Therefore, we used the Student's t-test to compare SDLRS responses between students who had completed their preclinical studies (Study A, Survey Iteration 3) and third- or fourth-year clinical students (Study B). The results indicated that there was no statistically significant difference in the SDLRS data between the preclinical and clinical student responses (Table 4).
Study B—Comparison of preclinical versus clinical SDLRS scores.

Note: SDLRS, self-directed learning readiness scale; SE, standard error, M, mean.
Student perspective of engagement with SDL
We assessed clinical students’ perspectives on their SDL development during medical school through 2 open-ended questions. These questions asked students to reflect on how their SDL knowledge, skills, and attitudes developed and to describe what experiences contributed to these changes. We identified a set of 18 primary codes that included 8 from a previous study 20 and ten new codes. After review and discussion by the analysis team to identify commonalities, 4 initial codes were merged into broader categorical codes, eg, the initial code of “experiential learning” was merged into the final code of “clinical curriculum,” resulting in a set of 14 final codes. We grouped the 14 final codes into 3 themes: Contributors, Self-Awareness, and Proficiency (Table 5). These themes represent the concepts conveyed in the student responses to the 2 open-ended questions on how their knowledge, skills, and attitudes toward SDL developed.
Study B—Summary of thematic analysis.

Note: SDL, self-directed learning.
Contributors: The contributors theme includes descriptions of various components of the medical school experience that students perceived as contributing to the development of their SDL knowledge, skills, and attitudes. Students made statements identifying independent learning and studying for classes in the preclinical didactic courses and preparation for board exams as contributors, I think a lot of the “independent learning” lectures we receive in our first and second years of medical school helped me learn how to manage my time and ability to teach myself. It was great preparation for studying for Step 1. They highlighted research and SDL assignments associated with their development as self-directed learners, assignments throughout the preclinical years in medical school prepared me for looking up information in the clinical years. I have definitely grown in my ability to research and comb through databases for information. Students also noted that clinical experiences contributed to their SDL development, I think the things that contributed the most were the time spent on wards learning about my own patients. I think that's when I had to utilize SDL the most to understand and coordinate all my knowledge up to that point into a well-thought-out plan.
Self-awareness: The theme of self-awareness includes student reflections on their traits, behaviors, and feelings regarding SDL throughout the medical school experience. Students described feelings of confidence and enjoyment of SDL, SDL assignments throughout medical school have prepared me to be a self-starter who is capable of setting and meeting personal academic goals and I enjoy SDL activities because it allows me to learn in a way that allows me to remember the information best. Their reflections encompassed their past and current knowledge, skills, and attitudes toward SDL, I am much more inclined to seek out information that I did not know instead of just shrugging it off and forgetting about it. I am much more likely to read textbooks or journal articles for pleasure, which is something I would never have imagined that I would do. I am much more inquisitive than I was before starting medical school. They also considered their SDL development as it related to their professional identity, I will not be able to learn everything I need to know at any point of my career, and I will eventually reach a point where the questions I have will only be answerable in literature, rather than in reference texts and I think SDL is imperative as a medical student to develop into a competent physician.
Proficiency: The theme proficiency includes student perceptions of how SDL advanced their skills in knowledge acquisition. Students commented on their ability to manage time and work efficiently, instead of cramming information, I understand how to better organize my time to become more efficient and proactive. Students discussed the development of specific skills, As a medical student, learning more complex topics that don't always have one quality, consistent resource, I have become better at looking for information in other resources, including those online and looking to peers. They also discussed the challenges of developing their SDL skills, SDL has not been easy for me, as I like to have clear goals set out for me when it comes to learning. Since being on the wards, I have somewhat improved in my ability and willingness to seek out information independently (eg, via UpToDate), but I still do not feel very confident in my ability to do so. Additionally, students reflected on the quality and depth of learning they gained through SDL, When I began to approach the assignments for this course, my goal was to complete the required elements, but I quickly became engrossed in the learning I was doing and wanted to really understand the topics of my reports.
Overall, student reflections provided insight into the impact of medical school experiences on the development of self-directed learners. Students referred to the changes they experienced in how they engaged with learning through SDL activities, One example of change that I have experienced in my SDL has been a diminishing of emphasis on completion for its own sake, and a return to focus on the content itself.
Discussion
In this study, we examined the impact of the medical school experience on students’ SDL across all 4 years of training, using both qualitative and quantitative methods. In Study A, using the Hendry and Ginns version of the SDLRS 26 validated in our population of medical students, we found that 3 of the subscales remained constant over the 3 iterations of the survey while the self-determination subscale increased significantly between the first and third iterations of the survey in preclinical students. In Study B, an analysis of clinical students’ comments indicated a perceived increase in their SDL abilities and a growing appreciation of SDL, although their SDLRS scores did not differ from the results observed in Study A.
Assessment of students’ readiness to engage in SDL has commonly used survey instruments that measure factors characteristic of adult learners including attitudes, abilities, and personality traits.26,27,31,32 Williams and Brown found that the survey modified by Hendry and Ginns, a 4-factor 36-item model, best fits the medical student data in a confirmatory factor analysis compared to Fisher et al’s 40-item SDLRS or 29-item SDLRS.26,27,31,33 Williams and Brown recommended that researchers use the survey instrument modified by Hendry and Ginns to measure SDL readiness in undergraduate medical students which is why we chose to use this instrument. 33
As reported in a scoping review, many studies have examined the readiness of medical students to engage in SDL at a single time point, typically administered at matriculation. 23 In one longitudinal study, Premkumar et al found that SDLRS scores significantly decreased in 5 different cohorts of Canadian medical students at the end of their first year, and these scores did not change throughout their medical school careers. 34 In a subsequent study with students at a medical school in India, Premkumar et al reported comparable results, with SDLRS scores decreasing over the course of training compared to scores at admission. 35 Kim and Yang administered the Korean version of the SDLRS (SDLRS-K-96) to Korean medical students every semester for 3 years. 36 They found that SDLRS scores increased after the first year but remained stable over the next 2 years. To date, longitudinal studies have not provided consistent results regarding SDL readiness in medical students. This may be due, in part, to the variability in measurement tools, curricula, and timing of administration of surveys. Furthermore, quantitative surveys alone may not be the most effective method for measuring SDL readiness. 37
In our longitudinal SDLRS study (Study A), we found no correlation between age or years of education and SDLRS scores. Other studies have shown a correlation between SDLRS scores and age. However, students in those studies matriculated at a younger age than students in Western medical schools and therefore may not be an appropriate comparison.25,35,38 In our study, self-determination was the only 1 of 4 subscales that changed, showing a significant increase over the 2 preclinical years. We observed gender-related differences in self-determination scores at the end of the first year. However, this difference was not observed by the end of the second year. Studies on self-determination theory in medical students have suggested that there are gender differences although this could be due to gender-related differences in self-assessment ratings.39,40 We have no explanation for why there were no gender-related differences in self-determination scores by the end of the second year for these 2 cohorts. It will be important to explore gender-related differences in SDL readiness to provide the appropriate support for all students.
Self-determined behavior is characterized by intrinsic motivation, typically driven by enjoyment, interest, or satisfaction, and a sense of control which facilitates the transition from dependent to the independent learner.41,42 This transition is critical as medical students become entrusted with patient care.43,44 Self-determination theory is a general theory of motivation that can be applied to all areas of life.42,45 According to self-determination theory, motivation exists on a dynamic continuum that is influenced by the learning environment, in which students may be unmotivated, extrinsically motivated, or intrinsically motivated. Self-determination theory also posits that 3 psychological needs must be fulfilled to stimulate and sustain intrinsic motivation: autonomy, competence, and relatedness. 42 One goal of medical education is to produce self-directed learners who are intrinsically motivated to learn which can be achieved by providing an environment that fosters autonomy, competence, and relatedness. 46 Self-determination was the subscale in which our students scored the lowest at the beginning of medical school, and thus had the most room for improvement. Consistent with other longitudinal studies34–36 we saw no further increase in any of the SDLRS subscales in clinical students compared to preclinical students. However, evidence for understanding how they developed self-determination was provided in our qualitative data from these same students (Study B). When clinical students reflected on their medical school experiences to date, they described developing SDL proficiency through being challenged and an increased awareness of their preferred learning methods (competence). Some students reported engaging in SDL beyond class requirements out of personal curiosity (autonomy). They imagined themselves using this process in their future practice as they developed their professional identities (relatedness).
The results of many studies, using various SDLRS instruments, indicate that medical students are ready to engage in SDL;26,34,35,47–49 however, without qualitative data, the SDLRS scores alone may not provide a full understanding of their SDL abilities. 37 Qualitative analysis of student perceptions is essential to provide insight into the impact of the medical school experience on the development of SDL. To our knowledge, there are few qualitative studies that explore medical student perceptions of SDL. Hill et al studied first-year students’ perceptions of their SDL skills following completion of an SDL activity. 20 Their findings indicated that not all students enter medical school with the same level of SDL skills, and these skills are positively impacted by opportunities to practice. Students recognized the need to further develop their SDL skills in concrete ways, such as improving their information literacy and time management, while recognizing the importance of SDL for future patient care. Premkumar et al conducted focus groups with preclinical students to capture their perceptions of SDL. 35 The authors identified 2 themes, the learning culture and assessment, that play crucial roles in how SDL is facilitated or deterred in their curriculum. Liu et al conducted structured interviews with medical students who had recently completed their core clerkships. 22 These authors reported that SDL in the clinical setting was driven by patient care and students recognized the importance of SDL in delivering evidence-based care.
The qualitative data in the current study provided a broad view of clinical students’ perceptions of their SDL development and the experiences that contributed to it. Like the Liu study, 22 our students commented on the value of the clinical experience to their continued SDL development. The LCME mandates that SDL activities be included in the curriculum. However, when asked about contributors to SDL development, our students described the impact of the medical education experience, including activities that were designated as SDL as well as those that were not. Activities not designated as SDL assignments, such as the preparation required for board exams or patient care, were highlighted as important contributors. Our data are consistent with the report by Burk-Rafel et al which demonstrated that medical students self-directed their learning in preparation for the Step 1 licensing exam using cocurricular and third-party resources. 50 As we saw with our students, medical students from the United Kingdom, in a letter to the editor, recognized the importance of SDL in their careers. 43 These students acknowledged that they receive feedback on their SDL abilities through various exams. However, they also encouraged medical educators to address and minimize ambiguity over the depth and duration spent on self-learning activities as a way of increasing confidence in the knowledge gained. 43 When discussing the development of SDL in medical students at our institution, SDL skills, knowledge, and attitudes were impacted by multiple experiences embedded throughout the 4 years of medical school. A caveat of this study is that students were not provided with the LCME, or any other definition, of SDL. Therefore, they answered the survey questions using their own concept of SDL.
One limitation is that our study was conducted at a single medical school in the midwestern United States; therefore, the results may not be generalizable to medical students at other institutions. Another limitation is that, in our longitudinal study of preclinical students (Study A), almost all students completed the first iteration of the survey during matriculation but only a subset of these students completed all 3 iterations. Finally, Study B took advantage of an opportunity presented during the COVID-19 pandemic, and due to this circumstance only a small number of students, who were at different stages of their clinical training, were available to participate. Although we were able to administer the SDLRS to both preclinical and clinical students, the clinical students in Study B were not part of the longitudinal Study A. A final limitation of this study is the absence of a power analysis in determining the sample size. Instead, the study's design relied upon the inclusion of all available respondents within the class cohorts. This approach, while aligning with our academic instructional and research objectives, may introduce limitations associated with the representativeness and generalizability of the findings.
Without the benefit of a thematic analysis of open-ended questions in the current study, we would have missed the depth and breadth of students’ experiences as they described how they developed their SDL skills, knowledge, and attitudes throughout medical school. These findings highlight the importance of considering multiple sources of data in evaluating the effectiveness of SDL in medical education, a finding supported by a systematic review of SDL assessment practices. 51 Future studies should include rigorous qualitative work, such as interviews, to further elucidate the impact of the array of educational experiences on SDL development in medical students.
Conclusions
The results of the longitudinal SDLRS indicated that by the end of the preclinical years, students experienced a positive change in the self-determination subscale. Our qualitative results suggested that a broad range of activities across the medical school experience appears to have a positive impact on our students’ transition to self-directed learners. While we have specifically designed discrete activities within courses to develop SDL skills, students’ comments indicate that their SDL capabilities were also influenced by a variety of other learning activities throughout their 4 years of medical school. By using a multimethod approach, we begin to appreciate the impact of the entire medical school experience on our students’ development as self-directed learners. Our current findings build on previous reports in the literature and provide a more comprehensive understanding of medical students’ SDL experiences over the course of 4 years of medical school.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205241242261 - Supplemental material for A Longitudinal Assessment of Self-directed Learning Readiness and Development in Medical Students
Supplemental material, sj-pdf-1-mde-10.1177_23821205241242261 for A Longitudinal Assessment of Self-directed Learning Readiness and Development in Medical Students by Megan Roberts, Alix Darden, Brandt Wiskur and Molly Hill in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to thank Drs Graham Hendry and Paul Ginns for providing the revised SDLRS survey. We would like to acknowledge the support and input from our colleagues in the Academy of Teaching Scholars Health Education Research Organization (HERO) at the University of Oklahoma College of Medicine. Thank you to the students at the University of Oklahoma College of Medicine for their willingness to participate in this education research study. Thank you to the following for the thoughtful review of the manuscript, David L Gordon, MD, Sylvia Hurst, PhD, David Kelley, MD, Frederick Miller, PhD, and Mary Moon, PhD.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
Megan Roberts, Alix Darden, and Molly Hill all had equal roles in conducting this research and contributed extensively to the joint authorship of this research report. Brandt Wiskur provided statistical analysis of quantitative data and contributed to writing methods and tables related to this analysis.
Consent
All participants included in studies A and B provided informed consent, granting permission for anonymized, aggregate evaluation data to be analyzed and shared with other medical educators in the interest of improving medical education. Only students who signed individual consent forms were included in the studies.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.