
Abstract
Objectives
To assess the impact and utility of an intensive care unit (ICU) rotation during the coronavirus disease 2019 (COVID-19) pandemic and the need for mandatory ICU rotations in training for all clinical specialties.
Methods
A mixed methods study was conducted from January to September 2021 at the Aga Khan University Hospital, including resident doctors who rotated through COVID ICU between May and September 2020. An online survey was undertaken, followed by two focused group discussions (FGDs).
Results
Fifty-nine complete responses out of a total of 86 were analyzed. Around 42.3% (n = 25) of doctors belonged to medicine/allied specialties and 57.6% (n = 34) had previous ICU experience. Both groups, with and without prior ICU experience, found the rotation equally challenging (82.3% (n = 28) versus 84% (n = 21), P = .776) and gained similar practical skills (35.3% (n = 12) versus 16% (n = 4), P = .072), however, those with experience gained significantly more knowledge (58.5% (n = 20) versus 32% (n = 8), P = .047). On opinion regarding mandatory ICU rotation, the majority agreed to have a mandatory rotation (82% (n = 28) versus 72% (n = 18), P = .421)) with an optimal duration of 1 to 2 months. The FGDs found that all residents encouraged the idea of mandatory training in ICU which must be tailored to their training specialty and suggested extending the duration beyond 1 week to ensure learning.
Conclusions
COVID ICU rotation was a good avenue for learning and the idea of mandatory ICU training was supported. Mandating ICU rotation might theoretically enhance response to emergencies. More research is needed to understand for feasible incorporation of ICU training in the curriculum.
Introduction
Critical care medicine training has come to be inherently understood as an important part of medicine, pulmonology, anaesthesia, and surgery training programs across the Western world. This program not only improves patient safety by ensuring better interdisciplinary care, but it also provides trainees with significant opportunities for professional development and crisis resource management.1–3 However, most non-Western countries, including Pakistan, do not require critical care rotation as a mandatory component of surgical and medical subspecialty training programs.4,5 As the reason for which the specialty is undervalued, and there is no specified curriculum requirement in place by accreditors like the College of Physicians and Surgeons, Pakistan (CPSP). Only a few training programs require residents to rotate in intensive care units (ICUs), such as pulmonology, cardiology, and anesthesia for a specified period. Other residency programs do not require critical care rotations, including those in neurology, palliative care, and surgical specialties such as general surgery and neurosurgery.
ICU patients are often managed by clinicians who are not intensivists in Pakistan and other low- and middle-income countries.1,2 However, the needs of an ever aging population means that a significant unmet demand for well-trained critical care providers has been predicted and highlighted over the last two decades.3,4 This was rapidly illustrated during the coronavirus disease 2019 (COVID-19) pandemic, when in addition to medical equipment shortages, there was a dearth of nurses and intensivists in ICUs across almost every country in the world including Pakistan.6–8 This called for tough, bold, and decisive approaches to bridge the gap between demand and supply in severely resource-constrained ICU setups to provide an acceptable level of care to the critically ill during the pandemic.9,10 On the one hand, the situation provided an opportunity to develop the competence of residents who had no prior ICU experience to work and perform successfully in a high-burden setting, but on the other hand, it raised important questions regarding the contents and quality of existing training programs.
During the first surge of COVID in Pakistan, a 14-bed closed ICU was designed for COVID 19 patients which was functional from May 2020. The unit was staffed with intensivists and residents from various clinical and nonclinical departments at the hospital. As a result of a shortage of medical staff, residents from specialties where ICU rotations are not part of the training program were also assigned duties in COVID's ICU. The roster was based on shift system, and the ICU team comprised three residents assigned to each shift with one senior resident having prior experience of rotation in general ICU such as cardiology, pulmonology, nephrology, or internal medicine residency programs. The other two junior residents were assigned from a variety of specialties including surgery and allied sciences, neurology, gastroenterology, and others (family medicine, oncology, and microbiology) with no or minimal exposure to ICU as part of their curriculum. On average, the resident teams typically cared for 10 to 12 critically ill patients, and they took 12-h alternate calls with a 24-h interval in between. The rotation schedule was carefully designed to avoid burn-out and minimize the psychological impact given the extent of the pandemic, the fear of contracting the disease, the taxing need of donning and doffing the personal protective equipment (PPE) and always keeping masks on. In October, dedicated medical staff were hired and placed in the unit while residents were sent back to their primary specialty rotations. During the study period, most of the patients admitted to the COVID ICU were suffering from severe respiratory failure complicated by severe acute respiratory distress syndrome, septic shock, and multiorgan failure, especially acute kidney injury, and myocarditis.
The challenge highlighted the need for new horizons of understanding and policy development to ensure the availability of a force of personnel trained to an adequate baseline of competencies and comfort in critical care, in the case of future scenarios threatening the healthcare systems like the COVID-19 pandemic. Since post-graduate trainees constitute most of the frontline healthcare physician workforce, the role of their training should be explored, assessed, and expanded to ensure future success in similar situations.
This study aims to investigate the residents’ experience of working and learning during a short COVID ICU rotation and the challenges encountered. The secondary objective was to explore the perception of the residents’ regarding the need for making ICU training a mandatory part of their training.
Materials and Methods
This study was conducted from January to September 2021 after the approval of the Ethical Review Committee (ERC 2021-5763-15395) at Aga Khan University (AKUH), Karachi, Pakistan. In line with the pragmatic approach, a mixed-methods study design (QUAN-Qual) was chosen to explore the residents’ experience during a COVID ICU rotation and its perceived impact on the need for a mandatory ICU rotation. All residents who rotated in the unit from May to September 2020 were eligible for the study. Those who spent less than a week in the ICU were excluded from the study.
Quantitative Phase
A survey was created in Research Electronic Data Capture (REDCap) to measure residents’ perceptions regarding their learning and practical experience of working in the COVID ICU, barriers to learning, and their opinion about mandating an ICU rotation as part of training. Pilot testing of the survey was conducted with five residents before administering it to eligible participants to check its readability and clarity. All 86 residents who rotated in the COVID ICU from May till September 2020 were invited to participate in the survey via email with an enclosed consent form designed on REDCap. Weekly reminders were sent to achieve the maximum response rate.
Statistical analysis
The data were analyzed using Statistical Package for the Social Sciences (SPSS) version 19. For all the variables proportions and percentages were calculated. The results were stratified for the previous experience and inferential statistics (chi-square or Fisher's exact test) were employed to determine its association with the learning experience and opinions regarding mandatory ICU rotation. A P-value less than .05 was considered significant.
Qualitative Phase
A descriptive exploratory study following the quantitative phase aimed at gaining in-depth insight about residents’ perceptions and experiences regarding the mandatory COVID ICU rotation. This study used two focus group discussions (FGDs) with 6 and 8 residents respectively, of 45 to 60 min each. All the 59 residents who completed the survey were contacted via email for voluntary participation in the FGDs. Out of the 42 residents who consented to participation, fourteen were purposefully selected to ensure representation from multiple disciplines, years of training, prior experience in ICU, and varying duration of rotation in COVID ICU in each FGD.
A qualitative research interview guide was developed based on the findings of the quantitative phase, and in consultation with the research team to ensure consistency between the two focus groups. The interview guide was piloted on two fellows who were not part of the study sample. Written informed consent was obtained from all the participants prior to conducting the FGDs. The FGDs were conducted via zoom with video recording (allowing nonverbal cues to be noted). Both the FGDs were facilitated by the same researcher who was not directly involved with the training or assessment of residents (QR) to mitigate interviewer-interviewee power relationship. Saturation of information was reached in the second FGD and thus data collection was stopped.
FGDs were audio recorded and verbatim transcribed. Voice recognition software was used to produce an initial transcription which was then corrected by the researcher. Researchers wrote additional notes during the FGDs to facilitate the data analysis process. Transcripts were anonymized before analysis to remove any identifiers.
In line with the pragmatic paradigm, a six-step thematic analysis was employed for data analysis. 11 An inductive approach was adopted keeping an open mind while conducting the discussions and the analysis, allowing for new themes to emerge in the analysis. 12
The anonymized interview guides transcripts were analyzed independently by two researchers (FK and QR). FK is an anesthesia faculty who was involved in designing the structure of the COVID ICU rotations and service. QR is a medical graduate with training and experience in conducting qualitative studies, and is heavily involved in postgraduate medical education as a medical educationist. The researchers familiarized themselves with the transcripts by in-depth reading and re-reading. This was followed by generating an initial set of codes for emerging concepts of interest independently. The codes were explored and grouped into branching concepts called sub-themes and themes. The two researchers (QR and FK) discussed the findings with all the authors and the themes were named and defined with consensus with all the authors.
The study findings from the quantitative and qualitative phases were combined and interpreted together after the data collection and analysis of each phase to gain a richer understanding of the trainees’ experience during their COVID ICU rotation.
Strategies to Optimize Trustworthiness in the Study
To ensure trustworthiness in the conduct and the results of the study, the Lincoln and Guba framework was adopted. 13
Credibility was established using invitation for voluntary participation in the study, data collection by a nonclinical team member with experience in qualitative studies thus facilitating rapport building and openness of the residents during discussions, purposive sampling by including trainees from different disciplines, levels of training, and varying experience in ICU, use of participants’ verbatim quotes, triangulation at person and data collection levels, and comparing and confirming the findings with the quantitative phase, respectively.
Dependability was attained by including the researcher with expertise in qualitative research in the team, transcription verbatim of the FGDs, and reading the transcripts multiple times to ensure accurate interpretation and to minimize the potential for researcher's bias, and independent interpretation of transcripts by two researchers with consensus on subthemes and themes.
For confirmability, two researchers were involved in the read up and analysis to remove bias and to confirm the data's accuracy, meaning and relevance. Additionally, supporting interview excerpts were provided for the emerging themes. 14
Transferability was achieved by purposive sampling of participants to acquire maximum variation and providing details of the participant demographic and work setting thus leading to a thick description, and data collection by the nonclinical researcher to mitigate interviewer-interviewee power relationship. 15
Results
Quantitative Phase
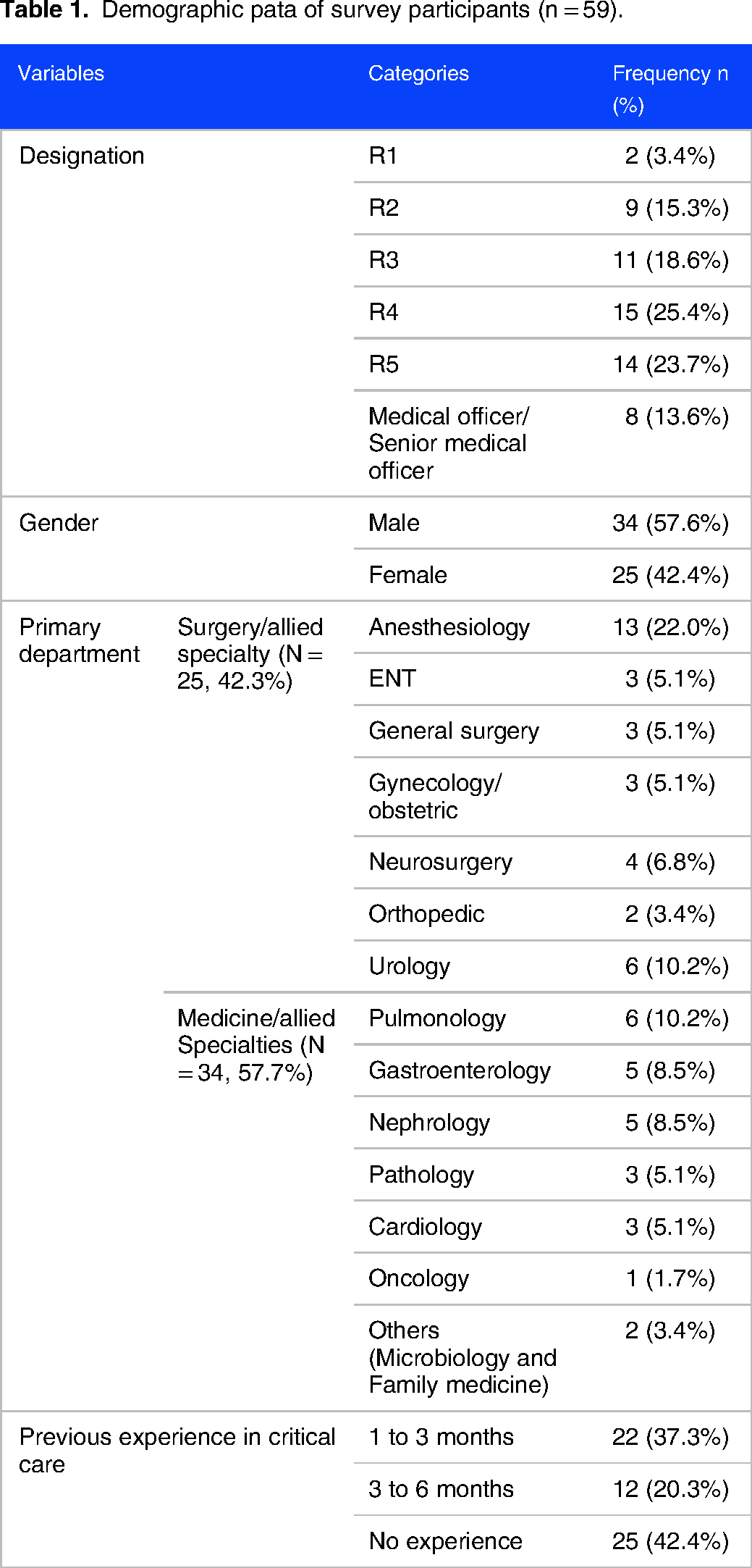
A total of 68 out of 86 eligible residents responded to the study (Figure 1: COREQ flow diagram). The final analysis included 59 forms that were completely filled out, resulting in a response rate of 69% (59/86). A total of 57.6% (34) of respondents were males. The respondent demographic data, level of training, primary department, and previous experience in critical care are displayed in (Table 1). Almost half of the residents were working as a resident level 4 or 5 with 57.6% (34) belonging to Surgical and allied programs and the remainder training in Medicine and allied specialties. A little less than half of the respondents (42.4%) had no prior experience in critical care while the remaining 57.6% reported varied levels of experience ranging between 1 and 3 or 3 and 6 months.
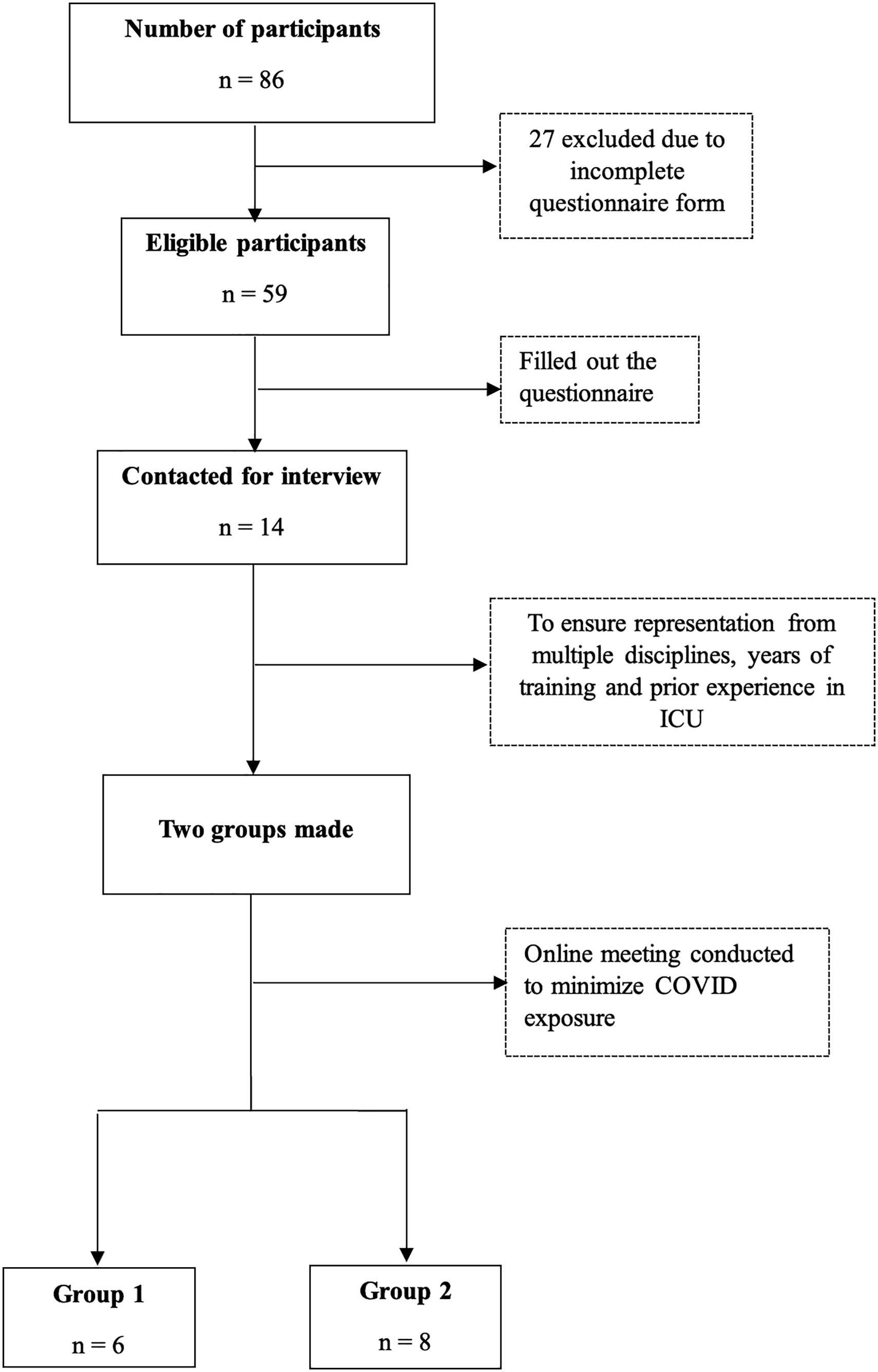
COREQ flow diagram.
Demographic pata of survey participants (n = 59).
Working Experience in COVID ICU
The working experience of the residents in COVID ICU was assessed based on six dimensions, as highlighted in Figure 2. The overall work experience was satisfying, and the residents felt well supported by both the staff (83%) and their seniors/peers (97%). A majority (68%) of the trainees reported that they were willingly sent to the COVID ICU. It was also reported that 98% of the doctors did not develop COVID symptoms or infection during the rotation.

Doctor experiences while working in COVID ICU. Abbreviations: COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Learning Experience During ICU Rotation
The results were stratified according to the previous experience ie, 34 (57.6%) residents with experience and 25 (42.4%) residents without previous experience in ICU (Table 2). The experienced and inexperienced groups were significantly different in knowledge and confidence perceived to work in other critical care areas. Almost the same percentage of the experienced and inexperienced residents (82.3% vs 84%, P-value = .776) found this rotation challenging. A low percentage of respondents from both groups felt that the rotation enhanced their practical skills (35.2% vs 16%, P-value = .072), however, respondents with prior experience reported a statistically significant enhancement in knowledge after the rotation (58.8% vs 32%, P-value = .047). Although 85% of experienced residents were confident to work in other critical care areas, 32.3% said that they may consider pursuing a career in critical care in future. The majority (64%) of residents in the group with no prior ICU rotation would not consider a career in critical care.
Learning experience during COVID ICU rotation of doctors.

Abbreviations: COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Statistically significant, P-value ≤ .05.
Performed and Observed Procedures in COVID-ICU
The residents received opportunities to perform and observe different clinical procedures during their rotation. The most observed and performed under direct supervision procedure was prone positioning (observed 89.8%, performed 76.3%) followed by mechanical ventilation (observed 76.3%, performed 61%), arterial line insertion (observed 62.7%, performed 61%), central venous line insertion (observed 62.7%, performed 54.2%), and patient transportation (observed 62.7%, performed 47.5%) while the least one was the chest tube insertion (observed 28.8%, performed 8.5%) (Supplemental Figure 1).
Barriers to Learning in COVID-ICU
According to the experienced residents, the biggest barrier to learning was the difference in critical care patients among different units and physicians (SICU, MICU, CCU, CICU) (27.1%) followed by the workload (25.4%) and lack of targeted goals of learning (23.7%). While those with no previous ICU experience, the most common challenge was inadequate exposure due to short rotation (27.1%) followed by a lack of competency-based curriculum (22%) and a lack of targeted goals of learning (20.4%) (Figure 3).

Barriers to learning in COVID-ICU. Abbreviations: COVID-19, coronavirus disease 2019; ICU, intensive care unit.
Opinion Regarding the Mandatory ICU Rotation
Overall, the residents had a positive opinion about the mandatory rotation in the ICU and no significant difference in opinion was noted between the two groups (Table 3). The majority (82.4% experienced and 72% inexperienced) were interested in having the ICU rotation as a mandatory part of the curriculum with optimal duration of 1 to 2 months. Most residents from both groups (94.2% experienced and 72% inexperienced) thought that regular and focused feedback from the supervising physician would be helpful to enhance the learning experience in the ICU.
Opinion regarding mandatory intensive care unit (ICU) Rotation.

Qualitative Phase
A total of 14 residents were included in the FGDs.
The participant characteristics are reported in Supplemental Table 1. Based on the data collection and thematic analysis, four overarching themes were identified (1) experience as a health care worker at the workplace (2) COVID ICU—a learning opportunity, (3) barriers to learning in COVID ICU, and (4) recommendation for future (Supplemental Table 2).
Theme 1: Experience as a Health Care Worker at the Workplace
Despite fear and uncertainty, the COVID pandemic ignited a passion in doctors to play their part as frontline workers
Fear and Uncertainty
The beginning of the rotation was met with uncertainty for most. Residents expressed a range of emotions ranging from fear (of contracting the disease) to reluctance (in rotating in COVID ICU). Most of the residents reported having apprehension at the time of posting. Okay. Maybe I can start first. I was a little scared, but it was a great learning experience. I was scared because this was something new and we did not know much about it at that time. (R 01) Initially, when I was going, I had that fear that I too will get affected, but then it turned out to be a good experience. (R 10) Ventilator settings, that was the most difficult part for me, because obviously, in our setting the medical ICU deals with it. So, we were not familiar with the vent settings but the attendings were really, really good and they really helped us. (R 07) This was an unprecedented, uncalled for a challenging situation and we had to face it, and cope with it. (R 9) (Supplemental Table 1). We did not know what it was like in a COVID ICU, what we are going to do, nobody briefed us; and initially, we were like literally a little bit reluctant in doing anything because obviously we haven't managed such patients. (R 08) (Supplemental Table 1).
To protect front-line workers against COVID-19, the infection control policy at AKUH mandated that all staff working in COVID-19 areas were expected to wear PPE. Also, the schedule was made such that each staff was assigned 12 h in the ICU, which increased the work hours. It was a very overwhelming rotation because you were expected to be there on job for 12 h continuously. But having your PPE on for 12 continuous hours, and the workload was a lot (R 01) (Supplemental Table 1).
The experience of the trainees in the COVID ICU was varied because of a lack of prior experience in managing COVID patients.
The trainees suggested having training sessions before posting them into the COVID ICU. There should be a training first before sending us to any such place or rotation. So, it would have been good if we are trained beforehand, especially for the surgery and histopathology residents, and OBGYN residents as well, because for them it was quite a different environment and completely different kind of patients as well. (R 01) (Supplemental Table 1).
Soon after starting, however, preparatory sessions were initiated, which were appreciated by the trainees. We were briefed before posting in COVID ICU, it was brief though but helpful. May be this started late as I went there in the second month after these rotations started … but yes, I think a 1-day workshop or a one-day boot camp sort of thing would be a good thing for focusing a little bit more on the COVID disease itself, and especially the system in the ICU. For those who don't know the system, it was quite difficult because some of our colleagues were not familiar with the system. (R 05) (Supplemental Table 1).
The residents appreciated the collaborative work environment in the ICU. All the residents appreciated the fact that they got a chance to work in diverse, multidisciplinary teams, especially trainees from other residency programs who normally do not work together. It was pretty nice … we got to interact with a lot of other people from other teams. (R 2) (Supplemental Table 1).
The residents generally reported great teamwork and collegiality among the teams. The nursing staff was also reported to be very cooperative despite the work pressures of the COVID ICU. “There was a good working environment and staff was quite cooperative. Some were really good, and some were average; they were also learning as COVID was new for everyone.” (R 04) (Supplemental Table 1).
Nursing staff initially allocated to COVID ICU were junior in experience. It was mainly because most senior nurses had other ICUs to handle. As a result, their workload and stress increased. However, this situation improved as nursing and support staff location were changed to allow more experienced nurses to be assigned to the high acuity patients in COVID ICU. The staff was new for us and so it was difficult to understand, or to make them understand what we are asking them or what we are asking them to do. So, it was a little bit difficult for me in just the first two to three days. (R 07) (Supplemental Table 1). The nursing staff was very good and very knowledgeable. At times they would do everything and just ask us to communicate the labs etc to the attending. (R 08) (Supplemental Table 1).
The teams appointed for rotation in the COVID ICU included residents from surgical and medical disciplines. At times there were also residents from no-clinical disciplines such as pathology or hematology. Although diverse in nature, care was taken while constituting teams that there should be at least one trainee with some experience in working and managing patients in ICU. The experience of the trainees also depended on the constitution of the teams. The challenge that I faced was that one of my team members was from orthopedics. That poor guy, he had no clue about ICU. I would say that it wasn’t his fault, he did his best. I am sure others would have also experienced similar situations with residents from specialties where they do not get to work in intensive care units. (R 05) (Supplemental Table 1). At my time our anesthesia resident would do everything from management to procedures. While our colleagues form surgical disciplines or from pathology would always ask about even the simplest things; this also increased the workload of the teams, but we cooperated. (R 11) (Supplemental Table 1).
Theme 2: COVID ICU—a Learning Opportunity
The residents described their time working in the COVID ICU as a great learning experience.
There were different types of patients, some without any co-morbids and some of them were with a number of co-morbids. So, a vast variety of patients were seen, and we have to work with all of them. So, it was a great learning experience. (R 12) (Supplemental Table 1). Well, I got to see COVID patients, which in my specialty, I would have never seen COVID management directly otherwise. So, I got to learn a lot more about COVID; I got firsthand experience of all the medications that we're using. (R 1) (Supplemental Table 1). Although it was a very short duration just one weeklong, but I did learn new things which we don't practice in managing the critical patients in cardiology or pulmonology or even oncology like how to prone a patient and for how long, and setting parameters related to ventilator, and it helped me in managing my patients after that rotation (R 06) (Supplemental Table 1).
Residents of the medical and allied specialties viewed it as a learning opportunity. Through close interaction, residents gained a better understanding of the management of COVID patients. This was noted by all the residents, regardless of their earlier experience in the ICU.
Faculty supervision is the mainstay of both service and residency training. This not only builds confidence in trainees but also ensures patient safety. In COVID ICU, the significance of supervision increased many folds since this rotation was not originally part of their residency training. Attending were really good, they were very responsive; wherever I called them for any query or any question, or if you're stuck somewhere. So, they used to respond promptly and adequately. So, in that way it was a great learning curve. (R 04) (Supplemental Table 1).
Theme 3: Barriers to Learning in the COVID ICU
The residents were posted in the COVID ICU for very short durations ranging from 1 to 2 weeks only, to avoid burnout and minimize the risk of exposure. While this was appreciated in terms of service and workload, this was perceived to be of minimal value in trainees’ learning. The duration was too short; I don't think it's enough to know about patients or problems with the COVID era. (R 04) (Supplemental Table 1). The only downside I would say was that we got it only for a week. So, we didn't know the long-term effects of the management. (R 08) (Supplemental Table 1).
Residents in medicine and allied specialties considered their posting an excellent opportunity to learn, but trainees in surgery considered it a burden. The national postgraduate curriculum for surgical and nonclinical specialties does not require ICU experience, so surgical residents referred to it as a waste of time and effort. Since they lacked experience in managing medical cases, especially in the ICU, they felt unable to contribute. I am a fourth-year surgical trainee, but I worked as an intern. I was only assigned clerical work like writing notes or orders, chasing labs, taking over. Occasionally I assisted in procedures, but I could never contribute to managing the patients. We were only there as a workforce but not helpful, which was very frustrating. I am sure other surgical residents also felt the same. (R 14) (Supplemental Table 1). There is no such thing as ICU exposure. We only get to learn that COVID is a grave condition, but no learning took place beside that; this is just unfair to expect senior or graduating surgery residents to do the scut work. Also, it is waste of human resource. (R 13) (Supplemental Table 1).
These challenges were also acknowledged by their peers from medicine where they witnessed their struggles first-hand. I think it was not such a great experience for our colleagues from surgical or non-clinical disciplines. They did what they could but that was very limited. Obviously, we understood that they had never been to ICU as it's not part of their curriculum, so they won’t be able to take decision about the medical condition of the patients; they were asked just to be there. So, I won’t say it was their fault, they tried their level best. (R 07) (Supplemental Table 1).
Theme 4: Future Recommendation:
Residents noted that the ICU played a vital role in patient care and that one should be able to assess the severity of patients’ conditions and make appropriate decisions. While many medical subspecialties require ICU training, surgical subspecialties don't, so any such rotation must be tailored to the specialty. ICU rotation should be made part of every residency training. It may be surgical ICU for surgery residents and medical ICU for medical and allied trainees. (R 3) (Supplemental Table 1).
Training before posting into the COVID ICU was encouraged by all residents to teach them about the disease as well as the functioning of the ICU while also enabling them to set clear learning objectives for the rotation. There should be a training first before sending us to any such place or rotation. So, it would have been good if we are trained beforehand, especially for the surgery and histopathology residents, and OBGYN residents as well, because for them it was quite a different environment and completely different kind of patients as well. (R 01) (Supplemental Table 1).
Residents also suggested extending the duration of the ICU rotation from 1 week to ensure at least some learning. The duration of any such posting should be 2-4 weeks at a stretch, not interrupted, so one can learn about the ICU related stuff, but not more than 4 weeks (R 10) (Supplemental Table 1).
Discussion
The initial COVID had been very challenging worldwide due to a variety of reasons, including a shortage of skilled human resources to provide care for critically ill patients. It is the first study of its kind from this region of the world that examines the impact of resident's short COVID ICU rotation which was implemented to address the shortage of health care professionals in providing patient care. In addition to the many challenges posed by this pandemic, the situation also presented opportunities for us to learn what specialty residents are capable of performing in a highly challenging critical care environment. In this study, we aimed to assess the educational value of a short ICU rotation especially through the lens of a resident with no prior experience and not mandated to go through an ICU rotation during the residency training. It was noted that students with and without prior experience in the ICU had different experiences at the end of the rotation. Our findings highlight the importance of longitudinal incorporation of ICU training in the residency curriculum as we found that those with prior ICU experience reported greater confidence, better management skills, and improved knowledge, which is consistent with previously reported findings.16,17 Residents also reported longer retention of learning, reflected in the ability to deal with critically ill patients in their specialty later. The short duration of exposure might have affected the responses of the residents with no prior ICU experience as their learning was compromised significantly, yet their perception of the educational value of such a rotation remained unaltered. This is supported by the finding that despite reporting minimal to no improvement in knowledge and skills, the majority favored the inclusion of ICU rotation as a mandatory part of their residency curriculum with a minimum duration of 1-2 months. Increasing the duration of ICU rotation beyond 1-2 months does not seem to impact the competency levels of residents as reported by Mullon et al, 18 hence primary focus should be on the quality of the rotation as a learning value and minimizing the challenges faced by the residents.
Despite the lack of a well-defined curriculum or goals, an online critical care course was offered over 8 h using the traditional experiential model, whose benefits were felt by most residents regardless of prior experience in the ICU. Several residents suggested during the focused discussions that a boot camp or a workshop with performance-based curriculum delivery, would have been more appropriate in improving the learning outcomes. There is evidence that the addition of a brief “hands-on” course or boot camp involving simulations and case scenarios, focused on essential aspects of critical care like mechanical ventilation, infection control practices etc, improves the quality of learning and care delivery.19,20
Several other barriers to learning were identified by our study. Both groups agreed on “the lack of targeted goals of learning” and “lack of competency-based curriculum’ as the most significant obstacle compromising the educational value of the rotation. It has been previously shown that one month of ICU rotation with a competency-based approach, increases the residents” confidence (31%-96% P < .001) in something as complicated as mechanical ventilation settings, provided the objectives are well-defined and regular instruction and supervision is maintained throughout the rotation. 21 In another study, perceived adequacy of ventilator knowledge and awareness of learning objectives during ICU rotation were found to be significantly associated with better performance (77% vs 70%, P = .0005) on the postrotation evaluation test. 5
Concerns about short patient safety and a perceived lack of future relevance were additional significant obstacles to learning, as noted in previous studies.22,23 Though it was understandable from a nonclinical resident's point of view, most surgery residents were unable to find relevance during focused discussions. This was surprising since treating surgeons are generally involved in postoperative intensive care following major interventions. This is also partly explained by the lack of defined learning goals and competencies and thus, can also be largely alleviated by providing clear objectives along with continuous supervision and feedback. Moreover, resident satisfaction with critical care training was strongly associated with awareness of learning objectives and adequate time for instruction, and lack thereof had a strong negative correlation. 5
Our study has several implications and should be understood in the context of the growing need for critical care services in the country and the ongoing deficit of intensivists. The significance of an ICU rotation in a trainee's professional growth and competence in managing his sickest patients cannot be overstated. Nevertheless, incorporating critical care rotation as a mandatory part of all residency programs will not yield the desired results as unfortunately, even the existing residency programs with mandatory ICU rotations, do not incorporate targeted goals of learning and competency-based education methods. Program-level interventions are needed to maximize the educational benefit of such a rotation. For a well-designed rotation, competencies and learning objectives must first be categorically defined, keeping in view specialty-specific needs. Multiple teaching strategies should be opted like lectures, simulations, case scenarios, and bedside discussions, before and during the rotation followed by standardized assessment tools to objectively and reliably evaluate the competency level achieved.
Strengths and Limitations
The main strength of our study lies in the exceptional setting where residents across diverse specialties completed rotations within a single ICU, where uniform protocols were followed, and encountering a comparable patient population. The resident could manage moderate to severe acute respiratory distress syndrome, septic shock, and acute renal failure requiring continuous dialysis and end-of-life care. Limitations of our study include single center experience, nonrandom sampling, and a very short duration of ICU rotation, which was unavoidable to minimize burnout and risk of exposure to COVID-19. This study questionnaire was only piloted with five (6%) trainees and was not validated using a standardized tool. Additionally, the FGDs were conducted many months after the residents had completed their COVID ICU rotation, which may have introduced recall bias. We also relied on the self-reporting of the learning outcomes as it was not possible to assess individual competencies objectively or subjectively, during a short rotation, due to the limitations posed by the pandemic situation.
Conclusion
In summary, our study highlights that the extent of the reported challenges encountered by specialty residents during a mandatory COVID ICU rotation suggested that traditional training/exposure to ICU is not adequate. This is due to the lack of targeted goals of learning, competency-based curriculum, and perceived lack of relevance. Increasing the basic critical care knowledge and procedural skills of residents would improve the likelihood of better patient outcomes, reduced utilization of critical care resources and increased cost savings. Improving the quality of critical care training will also enhance our emergency preparedness in the face of the ongoing pandemic and/or similar situations in future.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231222084 - Supplemental material for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study
Supplemental material, sj-docx-1-mde-10.1177_23821205231222084 for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study by Muhammad F. Khan, Ayesha Aziz, Qamar Riaz, Waleed B. Ghaffar, Fiza Khan and Asad Latif in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231222084 - Supplemental material for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study
Supplemental material, sj-docx-2-mde-10.1177_23821205231222084 for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study by Muhammad F. Khan, Ayesha Aziz, Qamar Riaz, Waleed B. Ghaffar, Fiza Khan and Asad Latif in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205231222084 - Supplemental material for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study
Supplemental material, sj-docx-3-mde-10.1177_23821205231222084 for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study by Muhammad F. Khan, Ayesha Aziz, Qamar Riaz, Waleed B. Ghaffar, Fiza Khan and Asad Latif in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-4-mde-10.1177_23821205231222084 - Supplemental material for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study
Supplemental material, sj-pdf-4-mde-10.1177_23821205231222084 for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study by Muhammad F. Khan, Ayesha Aziz, Qamar Riaz, Waleed B. Ghaffar, Fiza Khan and Asad Latif in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205231222084 - Supplemental material for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study
Supplemental material, sj-docx-5-mde-10.1177_23821205231222084 for The Impact of Short Intensive Care Rotation on Residents’ Experience in the COVID-19 Pandemic: A Mixed-Methods Study by Muhammad F. Khan, Ayesha Aziz, Qamar Riaz, Waleed B. Ghaffar, Fiza Khan and Asad Latif in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to acknowledge the help provided by Ms. Maheen Fazal in manuscript formatting and journal submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
The study was approved by the Ethical Review Committee (ERC 2021-5763-15395) at Aga Khan University (AKUH), Karachi, Pakistan.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.