
Abstract
OBJECTIVES
Providing cultural competence training is recommended as a way to improve patient-centered care and reduce health disparities. Increasing awareness of implicit biases and understanding internal motivations for overcoming these biases can influence provider decisions and communications with patients. This study aims to provide a health equity and implicit bias training to healthcare providers and assess knowledge and attitude gains.
METHODS
Mid-career primary healthcare providers (n = 21) with at least 5 years of primary care experience participated in the training as a prerequisite for providing patient care in a telehealth primary care practice that overwhelmingly serves patients of color.
RESULTS
There was a significant increase in knowledge (p < .001) as well as attitudes (p < .001) in healthcare providers from pretest to posttest. Almost none (4.5%) of the providers were distracted during the training, which may be due to the interactive nature of the training that included group-based reflection discussions.
CONCLUSION
A virtual training for primary healthcare providers on health equity and implicit bias improved knowledge and equitable attitudes and had high satisfaction. Additional research is needed to determine if this type of training can influence providers’ ability to actively address known disparities in care.
Introduction
Cultural competence training during medical education is foundational to working with patients, leading to improved patient-centered care and reduced health disparities.1–3 Health disparities show up in nearly every type of care. For example, in the United States, among those 35 years and older, heart disease death rates among Blacks remain higher than among Whites, 4 and life expectancy in the United States has consistently been lower in the Black population compared to that of the White population. 5 A study examining health indicators from 1999 to 2018 found that the gap in disparities between middle-aged Hispanics and Whites increased for diabetes and hypertension. 6 Hispanics have lower levels of health literacy compared to other population groups, 7 which may contribute to disparities, particularly with medication adherence. 8 People of Color had less access to healthcare when compared to Whites, worse infant mortality outcomes, and higher prevalence of chronic conditions. 9
In 2003, the Institute of Medicine (IOM) published Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, a comprehensive report on racial and ethnic disparities in healthcare. 10 This report documented widespread stereotyping, bias, and uncertainty on the part of healthcare providers, even after adjusting for socioeconomic status. Recommendations included that cross-cultural education be embedded into the training of future healthcare providers. In response to the findings, the Liaison Committee on Medical Education (LCME), which accredits medical schools in the United States, began requiring that medical students demonstrate a standard level of “cultural competence” upon graduation. 11 To facilitate this requirement, the American Association of Medical Colleges developed the Tool for Assessing Cultural Competence Training to help ensure that medical schools meet compliance with the LCME's new standard. 12 The Accreditation Council for Graduate Medical Education expects a new practitioner to obtain competency in interpersonal and communication skills, highlighting the importance of a provider being able to communicate well with patients and families across a broad range of socioeconomic and cultural backgrounds. 13 Evidence of the need for continued cultural competence training lies in the health disparities that still persist today, 20 years after the publication of the IOM Unequal Treatment report.
Although healthcare providers are required to have cultural competency education, there is considerable variation in the content and depth provided. 11 Most cultural competence training during medical school has a total contact time of less than one week. 14 Moreover, once healthcare providers begin seeing patients, there is no standardized training in cultural competence, a time when consultation practices and norms are typically becoming established. One way to bridge the gap in widespread provider uptake of cultural competency training is for Continuing Medical Education to require the provider to complete a specific number of credits that focus on cultural competency at specific intervals throughout a provider's career. Cultural competence training should be provided at all stages of a healthcare provider's career to better address healthcare disparities.11,15 The Learning Health Systems (LHS) framework is especially applicable for providers who are actively practicing and may not be in the classroom frequently because the cyclic and iterative nature of the LHS framework sets the tone for learning in a peer-setting and enables the learner to carry the LHS process into practice and collaborate effectively with colleagues in an interdisciplinary team. 16 This type of training can lead to improved knowledge, attitudes, and skills 17 among healthcare providers and lead to increased patient satisfaction. 18
Cultural competence training can assist healthcare professionals in learning about the norms of a variety of populations to effectively deliver healthcare services that meet the social, cultural, and linguistic needs of patients. 19 Training specifically in implicit bias, a bias or prejudice that is present but not consciously recognized, is an important component of cultural competency education since such biases can contribute to health disparities by influencing provider decisions and communications. 20 Implicit biases can negatively impact the patients’ perceptions, judgments, and trust in their provider, which, in turn, can impact the patients’ engagement and adherence to treatment and increase health disparities. 21 Hagiwara et al 22 examined the effectiveness of current implicit bias training and found that awareness alone is not enough; besides, it can lead to negative outcomes. Instead, training should focus on providers’ awareness along with their understanding of internal motivations for overcoming implicit bias. Training should also help to improve provider communication behaviors by teaching strategies to overcome habitual responses to situations that may result in unconscious biases.22,23 However, a standardized method to overcoming bias in medicine has not been established. It is known that many cultural competency trainings do not result in the learners exhibiting the desired behaviors over a long period of time for myriad reasons, including limited time in the exam room to implement some of the suggested techniques and the training being too superficial to meaningfully apply to practice. 24
The present study sought to examine the effect of a health equity and implicit bias training for mid-career primary care providers on knowledge, attitudes, and satisfaction.
Methods
This pilot study, which was conducted from May 2021 to October 2022 in New York, was a part of the virtual onboarding of primary care providers throughout the United States in an effort to measure the impact of the curriculum used to train providers. The study was deemed exempt by Teachers College Columbia University Institutional Review Board (IRB 23-024).
Intervention
Spora Health, a virtual primary care platform focused on decreasing health disparities for Black, Indigenous, (and) People of Color patients, developed a health equity and implicit bias training for healthcare providers. Although a nationally representative survey of ambulatory physicians found that only 19% said that their practice requires cultural competency training for new hires, 25 this type of training is a requirement to be a provider at Spora Health. This training was designed for primary care providers, including physicians, physician assistants, and nurse practitioners, who are mid-career, which is defined as having at least five years of experience. Informed consent was not required; however, providers granted written consent when signing up for the course, understanding that completion of the in-person portion of the training was required before they could see patients. The training had the goal to increase knowledge of health disparities of the target patient population, promote equitable attitudes, and provide evidence-based strategies for behavior change. The training incorporated educational strategies and methods based upon expert consensus 26 and used an integrated approach that combined clinical experiences with didactic instruction and self-reflection, which is more likely to enhance student awareness and knowledge. 27 The training was grounded in Adult Learning Theory, which includes internal motivation to learn28,29 and aimed to reduce the amount of time spent in a lecture style of learning, instead opting for frequent discussion and activities. The training was intersectional, meaning that each module topic examines the patient experience through their own simultaneous membership of multiple interconnected social categories such as race, gender, social class, etc, and how these interact within a context of systems and structures of power.30,31 For example, the module on non-verbal communication looked at non-verbal communication disparities between the patient and provider by race, as well as other identities that lead to non-verbal disparities and known methods for resolving this. The training was comprised of 11 modules that took place in two parts; in the first part, there were six modules that were live-facilitated virtually, and in the second part, there were five modules that were asynchronous and self-paced.
Study design
This virtual, cohort-based training sought to improve patient–provider interactions as a result of improved cultural competency. As seen in Figure 1, providers first completed a pretest that assesses knowledge and attitudes at baseline related to the subjects covered in the training. Providers were then grouped into small cohorts, typically of three to five providers, and completed the first part of the training, which spans six modules that are facilitated live in two days through an online video conference platform. The first day consisted of modules on non-verbal communication, verbal communication, and health literacy (see Figure 1), followed by a behavior change activity. The second day consisted of modules on trauma-informed care, motivational interviewing, and maternal health (see Figure 1), followed by another behavior change activity. The behavior change activities were based on the Fogg Behavioral Model (FBM), 32 which asserts that for a person to perform a target behavior, he or she must (a) be sufficiently motivated, (b) have the ability to perform the behavior, and (c) be triggered to perform the behavior. The providers spent time working independently to design a behavior change plan that incorporates information learned throughout the day. The providers then showcased their plans to the entire group.
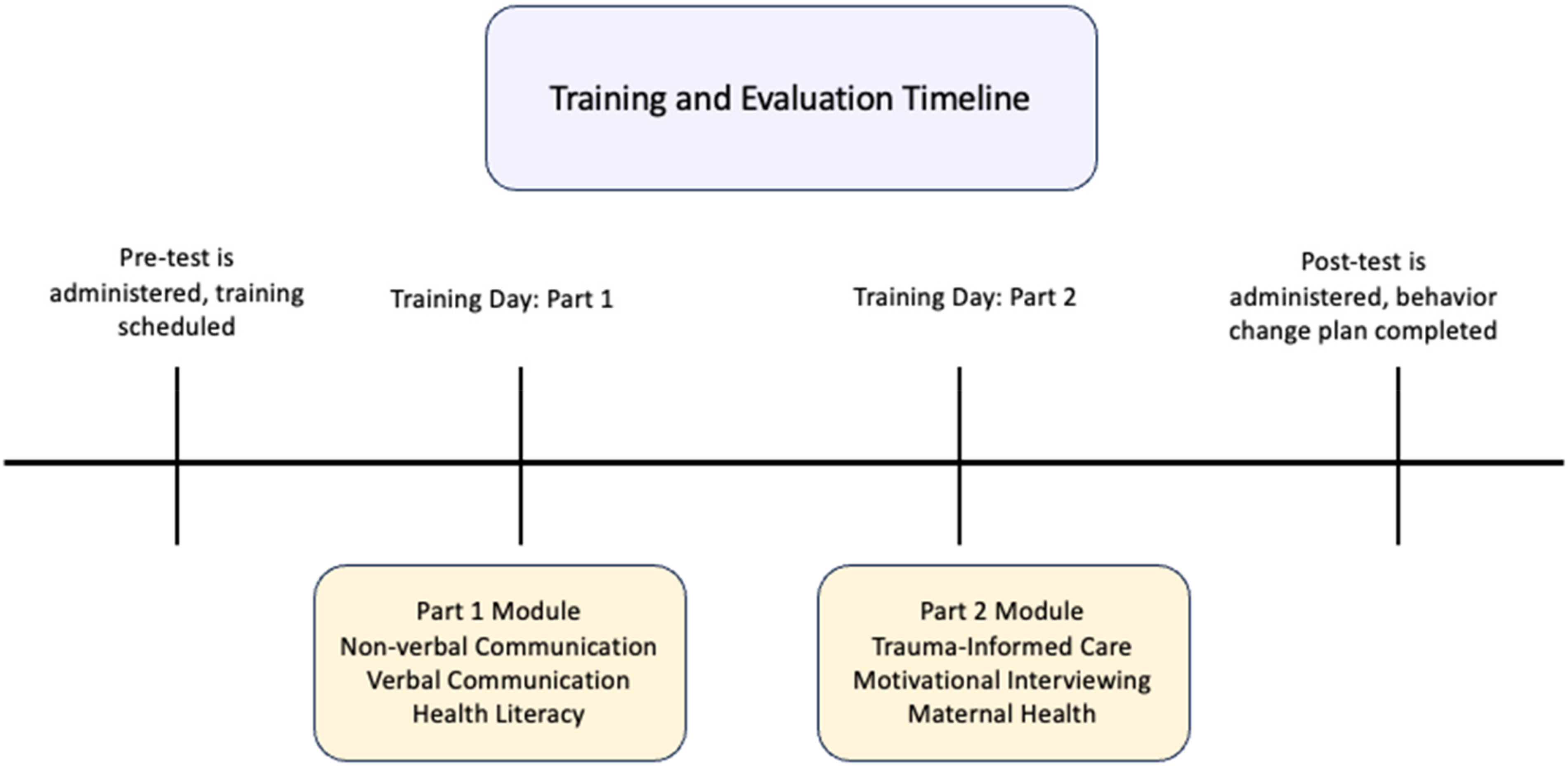
Training and evaluation timeline.
The second part of the training was comprised of five self-paced modules hosted on an online learning platform. The self-paced training covered modules on sexuality, gender and sexism, mental health and substance use, and ableism and cultural humility. The asynchronous nature of this part of the training means that discussions are moved to an online platform, where providers were asked questions similar to those asked in the live training and asked to interact with each other. The self-paced modules end with the provider designing a behavior change plan based on the FBM and uploading it to the platform for review. These were released for use to the providers once they began seeing patients through the virtual primary care platform. Providers were given 45 days to complete the training, extensions are granted if they have a heavy patient load.
Measures
Knowledge
Questions (n = 6) were created based on key aspects of the material that were covered during the training and had high face validity. The questions at the pretest were used to assess the knowledge base of the providers. The knowledge questions were on a scale of 0 to 1. Sample questions included, “What is one main distinction between ACEs and weathering?”
Attitudes
Topics were examined and questions (n = 6) were developed based on attitudes relevant to implicit bias. 33 The attitude questions were on a five-point Likert scale and included questions such as, “Non-verbal communication (e.g., eye contact, body position, pauses in conversation, and facial expression) affects patient adherence to a treatment plan.”
Reflective questions
Posttest reflective and integrative engagement questions (n = 4) were adapted 34 and included how distracted providers were, what they liked best, what could be improved, and what other topics could be added.
Net promoter score
This was comprised of one question that measures the loyalty of customers to a company. It asked how likely a respondent is to recommend a product to their friends. It is on a scale from −100 to +100. 35 A positive score or NPS above 0 is considered “good,” +50 is considered “excellent,” and above 70 is considered “world-class.”
Procedures
Prior to the Part 1 live-facilitation training, the providers were asked to take a pretest that included one knowledge and one attitudinal question per module (n = 6), which corresponded to topics that were covered during the modules. The pretest assisted the facilitator in understanding the baseline knowledge and attitudes that the provider arrived with. Following completion of the Part 2 training, providers were emailed a posttest that had the same six knowledge items and six attitudinal items as well as the reflective questions.
Statistical analysis
Descriptive statistics were used to analyze demographics. A paired t-test was used to calculate differences in pretest and posttest scores. Two-sided p-value of <0.05 was considered statistically significant. When significant differences were found, Cohen's d was calculated to determine the effect size. The Net Promoter Score was calculated using a Net Promoter Calculator. 36
Results
There were 21 providers who completed the pretest and posttest. The majority (50%, n = 10) were Nurse Practitioners, followed by Physician Assistants (35%, n = 7), and Primary Care Medical Doctors (15%, n = 4). Two-thirds identified as People of Color (67%, n = 14) and 81% were female (n = 71). Almost half (48%, n = 10) were in their 40 s, 24% (n = 5) in their 30 s, 19% (n = 4) were in their 50 s, and 10% (n = 2) were in their 60 s.
The mean days between pretest and posttest was 16.33 (SD = 10.65). There was a significant increase in knowledge from pretest (M = 2.14, SD = 1.20) to posttest (M = 3.76, SD = 1.41), t = 5.06, p < .001, with a large effect size (d = 1.11 95% CI [0.56-–1.64]). There was also a significant increase in attitudes from pretest (M = 26.43, SD = 1.91) to posttest (M = 27.76, SD = 2.17), t = 3.92, p < .001, with a large effect size (d = 0.86 95% CI [0.35-1.35). The NPS was 91, which indicates that providers were highly likely to recommend the training to others. A high Net Promoter Score was a positive outcome for the training because the intention was to help providers feel equipped to work with patients from a variety of backgrounds, and a high score indicates that providers feel that they could recommend this training to someone who is looking to learn about cultural competency.
Almost all, 95.5% (n = 20) of the providers reported that they rarely or never experienced distractions during the training. The majority (66.7%, n = 14) of the providers indicated what they liked best about the training was the interactive components, such as the video and discussions. The other 33.3% (n=7) indicated that they liked best the reading and preparatory materials that were delivered prior to each lesson. When asked what could be improved, slightly more than half of the providers (52.4%, n=11) stated there was nothing that needed to be improved. The other (47.6%, n=10) providers indicated that they would like more flexibility in scheduling the training (eg, at night, weekends), more role-playing activities, specifically in motivational interviewing, additional preparation time before the training, time for phatic communications to increase social bonds with other providers, the length of time could be condensed, and adding stretching breaks. When asked what topics they would like added to the existing curriculum, the majority (71.4%, n=15) of providers indicated there were no other topics that needed to be included. The other 28.6% (n=6) expressed interest in topics such as epigenetics, how to approach discussions around race, Black men's health challenges, a deeper dive into trauma-informed care, specifically in a virtual primary care setting, and to include a role-playing activity that allows providers to engage with motivational interviewing.
Discussion
Providers significantly increased their knowledge of key aspects of the material that was covered during the training as well as significantly increased their attitudes regarding implicit bias from pretest to posttest. The large effect sizes of both outcomes indicate that there is also practical significance. Research suggests that unconscious bias can be altered when the recipient becomes aware of the unconscious bias and is motivated to change. 23 However, there continues to be a need to determine whether awareness and improved knowledge translate into actual behavior change. 17 There is some suggestion that implicit bias is not a strong indicator of behavior. 22 Nonetheless, studies have demonstrated that this type of training can improve patient satisfaction among minority groups. 18
Providers were expected to complete the training on their personal computers in a small group facilitated video conference. Providers were notified that they should be in a quiet setting where they would not have any distractions in order to facilitate peer-based discussion and learning during the scheduled time. Advance notice of this expectation was shared during the sign-up period, along with time slots available to take the training. Literature on online learning often mentions readily available distractions affecting learner performance,37,38 but this appeared not to be an issue for the providers. Several factors might explain this. Firstly, there was an expectation of a quiet, dedicated learning environment with defined time boundaries. Secondly, if a learner attended the training while distracted, such as driving, they were asked to reschedule. Thirdly, the training was mandatory for providers before they could start seeing patients, so focusing and not being distracted increased the likelihood of successful completion, which had tangible benefits for the provider. Lastly, it could be that the training itself was engaging so that the providers were not distracted. The training was highly interactive and included group-based reflection sessions where discussions were held about potential bias and meaningful strategies to use to manage bias in real-world clinical environments, which can foster openness and engagement. 39 Providers were extremely likely to recommend the training, which has been shown to be positively related to engagement and less turnover intent. 40
There were limitations, including a small sample size, although it was helpful to have this many providers participate in a pilot study. In addition, validated measures were not used to assess learning attitudes regarding implicit bias. While there are assessment tools available,41,42 there is a lack of consensus on the value of some of these assessment tools, such as the Implicit Association Test, 43 for long-term learning, or as a program evaluation tool. The measures used in this study assessed the specific outcomes and objectives of the training that the providers completed. The knowledge and attitude questions were carefully constructed based on content from a literature review, an examination of the topics delivered, and face validity was sought with experts. Another limitation could have been social desirability bias. The completion of the training was required for employment at a virtual primary care practice explicitly focused on better serving the needs of People of Color, so it may be that providers wanted to present very equitable attitudes on both the pre- and posttest to avoid negative perceptions from their employer. However, if this was the case, there would not have been such a large effect size from pre to posttest; therefore, the significant change in attitudes that was found is most likely meaningful.
The goal of the training was knowledge, attitudes, behaviors, and satisfaction, which was met and should improve care for People of Color. Future research should include a larger cohort over a longer time period and examine patient outcomes, which was not able to be captured in the current study. The next steps will be to assess whether self-reported provider behaviors tie back to patient surveys that report on trust and overall satisfaction. A meta-analysis found that when patients have higher trust in their healthcare professional, they report more beneficial health behaviors, higher satisfaction, higher health-related quality of life, and better symptom-oriented subjective outcomes. 44 Trust in the healthcare professional can have a positive impact on health behaviors which, in turn, leads to improvements in health outcomes. 45
Conclusion
The results suggest that a virtual training for mid-career primary care providers on health equity and implicit bias has the ability to increase knowledge and equitable attitudes. This training can contribute to improving providers’ ability to actively address known disparities in care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231219614 - Supplemental material for Evaluation of a Virtual Health Equity Training for Mid-Career Primary Healthcare Providers
Supplemental material, sj-docx-1-mde-10.1177_23821205231219614 for Evaluation of a Virtual Health Equity Training for Mid-Career Primary Healthcare Providers by Katherine J. Roberts, and Elise Omaits in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231219614 - Supplemental material for Evaluation of a Virtual Health Equity Training for Mid-Career Primary Healthcare Providers
Supplemental material, sj-docx-2-mde-10.1177_23821205231219614 for Evaluation of a Virtual Health Equity Training for Mid-Career Primary Healthcare Providers by Katherine J. Roberts, and Elise Omaits in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors would like to thank Dan Miller for his support in this project.
DECLARATION OF CONFLICTING INTERESTS
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KJR received funding from Spora Health for the data analysis and EO received no funding for this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.