
Abstract
OBJECTIVES
Impostor Phenomenon (IP) describes feelings of distrust in one's own capabilities or accomplishments. This experience exists across many professional settings, affecting men and women across diverse backgrounds. IP has not been studied within a military health system. The purpose of this study was to evaluate the prevalence of IP among physicians at a military hospital.
METHODS
An online survey was constructed incorporating the Clance Impostor Phenomenon Scale (CIPS) and demographic data. All physicians at the institution received the survey link via email and the survey remained open for 1 month for completion. Multivariable analysis was performed to identify significant differences among groups as well as characteristics associated with IP. Exploratory factor analysis was used to examine the factor structure of the CIPS.
RESULTS
The response rate was 25% (94/376). Forty-one respondents (44.1%) had CIPS scores ranging between 41 and 60, classifying the respondent as having moderate IP experiences. Differences in scores were noted for age and years of experience (both P < .01). No differences were noted based on gender, self-reported race/ethnicity, or surgical versus nonsurgical specialty. Active-duty respondents had a mean IP score of 62 (SD = 16) and civilian respondents had a mean IP score of 49 (SD = 12, P < .01).
CONCLUSION
With nearly half (46.3%) of respondents reporting frequent or intense IP experiences, this study underscores the pervasiveness of the issue and indicates concordance with previously published data. IP is not limited to certain subgroups or gender identity but rather is a common issue which may negatively affect a physician's well-being.
Introduction
Impostor syndrome or phenomenon (IP) are term used to describe individuals who, despite objective successes, have persistent self-doubt and fear of being exposed as a fraud. 1 This phenomenon was originally described by Clance and Imes among women. However, a recent study documents feelings of inadequacy in many professional settings regardless of gender or ethnicity.2,3 Feelings of IP exist at the beginning of medical education and persist throughout training. Imposter syndrome/phenomenon and burnout occur among American medical students and have been persistent throughout the literature.4,5 Approximately 30% of learners in medical education identify as impostors with higher rates noted among women. 5
IP is present across medical specialties. A study performed among general surgery staff and residents demonstrated higher scores on IP scales among trainees compared to staff. 6 IP was documented by Oriel et al among family medicine residents and found impostor scores correlated with depressive symptoms. 7 This phenomenon continues after residency and persists throughout careers. A study evaluating 28 physicians and their experiences with underperformance demonstrated that many participants who were at advanced stages of their careers questioned the validity of their achievements. 8
IP and the associated feelings of inadequacy can lead to frustration and unhappiness in the workplace. Gender, low self-esteem, and institutional culture are associated with higher rates of IP and in turn, high rates of burnout. 9 Quantitative studies have found statistically significant associations between IP and at least one aspect of mental health including self-esteem, burnout, depression, and psychological distress. 10 People with high levels of IP are afraid of appearing incompetent and fraudulent in front of others and are plagued by persistent self-doubts. As a result, those with IP may be less likely to pursue promotions or seek opportunities for advancement due to persistent doubts. 11 The Accreditation Council for Graduate Medical Education placed a focus on physician well-being and in July 2018, emphasized programmatic and institutional responsibility for prioritizing physician well-being, ensuring protected time with patients, and providing time for self-care. 12 A recent survey study evaluating the prevalence of IP among physicians in the United States noted higher odds of burnout among those with moderate, frequent, and intense IP. 13 This study also evaluated IP among members of the United States working population and noted physicians endorsed greater intensity of IP than workers in other fields. 13
Although the study by Shanafelt et al noted higher burnout in active military practice and veterans’ hospitals, those individuals accounted for a small portion of participants and the study did not distinguish between active-duty physicians and civilian physicians in the military healthcare system. 13 We sought to determine the prevalence of IP among physicians practicing in a military treatment facility. We hypothesize that female physicians will have higher rates of IP when compared to male counterparts and those who are active-duty military members will have higher rates of IP than civilian physicians, regardless of gender.
Methods
This work underwent a human protection review through Womack Army Medical Center (WAMC) at Fort Bragg, North Carolina and was determined to be exempt. In accordance with WAMC 32 CFR 219.104(2)(ii), the reviewer determined the protocol is exempt from IRB review as it involves survey procedures that are recorded in such a manner that the identity of human subjects cannot be readily identified and disclosure of subjects’ responses outside of research would not reasonably place the subjects at risk of civil or criminal liability. We conducted a survey-based prevalence study to identify IP in our Military Health System physician population. Dr Clance gave permission to use the Clance Impostor Phenomenon Scale (CIPS) in this population and we added questions about demographics and level of professional experience. 14 All physicians at Womack Army Medical Center received a web-based survey via email invitation in October 2021, which was created through SurveyMonkey®. The email contained a welcome letter describing the voluntary nature of the survey and served as the consent. By clicking the link in the survey, the participants indicated consent. Separate written consent forms were not utilized in this study. The email also included resources for counseling and chaplain services within the hospital. The study occurred over a 4-week period. Reminder emails about the survey were sent 2 and 3 weeks after the initial invitation, and the survey closed after 4 weeks.
The CIPS is a 20-item survey commonly used for assessing impostor phenomenon.15,16 While many scales exist in the evaluation of IP, the CIPS was chosen as it accounts for observed attributes or feelings that have not been addressed by other scales, such as acknowledging fear of evaluation or feeling less capable than peers. 1 The CIPS has been validated with high internal consistency noted during the validation study and a Cronbach's Alpha for the survey was α = .92. 16 In the survey, participants respond to questions such as “I avoid evaluations if possible and have dread of others evaluating me” and “At times, I feel my success has been due to some kind of luck.” 14 Participants indicate how true each statement is as it pertained to their own experiences on a Likert Scale with 1 indicating “not at all true” and 5 indicating “very true.” Scores are tallied with the final score determining the IP tendencies of the individual. Higher scores indicate stronger IP experiences with feelings more frequently and seriously interfering in a person's life. Individuals with composite scores of less than 40 are categorized as having few impostor experiences. 15 Composite scores between 41 and 60 indicate moderate IP experiences; a score between 61–80 means the respondent frequently has impostor experiences, and a score greater than 80 indicates intense IP experiences. 15
We classified respondents as surgical or nonsurgical based on their self-reported specialties. Surgical specialties included Urology, General Surgery, Orthopedics, Oral and maxillofacial surgery, Ophthalmology, OB/GYN, Anesthesia, Otolaryngology, and Podiatry. All other specialties were classified as nonsurgical. Race/ethnicity groups were pooled into the following categories: White, Black, Asian, Hispanic, and other.
Statistical analysis
Medians with associated interquartile ranges (IQR) were used to summarize nonnormally distributed continuous data while means and standard deviations are presented for normally distributed data. Differences in group means were accomplished using a one-way analysis of variance test with partial eta-squared values provided as measures of effect size. The chi-square test of independence was used for pairwise comparisons between groups. In cases of multiple comparisons, alpha levels for significance were adjusted using the Bonferroni adjustment. An Exploratory Factor Analysis was performed to evaluate the thematic structure of the survey. The Kaiser–Meyer–Olkin (KMO) measure of sampling and the Bartlett test were performed to evaluate for variance among any notable factors. Measures of internal consistency were assessed using Cronbach's alpha. Significance was declared at P < .05 for all tests. All data was analyzed by using SPSS Version 25.0 (SPSS, Chicago, IL).
Results
A total of 376 surveys were sent during the study period. Ninety-three individuals completed the survey with a response rate of 25%. The median time to complete the survey was approximately 4 min (230 s; IQR 170-327). No correlation was found between time spent completing the survey and CIP scores, r(91) = .04, P = .71. Demographic data is depicted in Table 1.
Self-reported sample demographics.
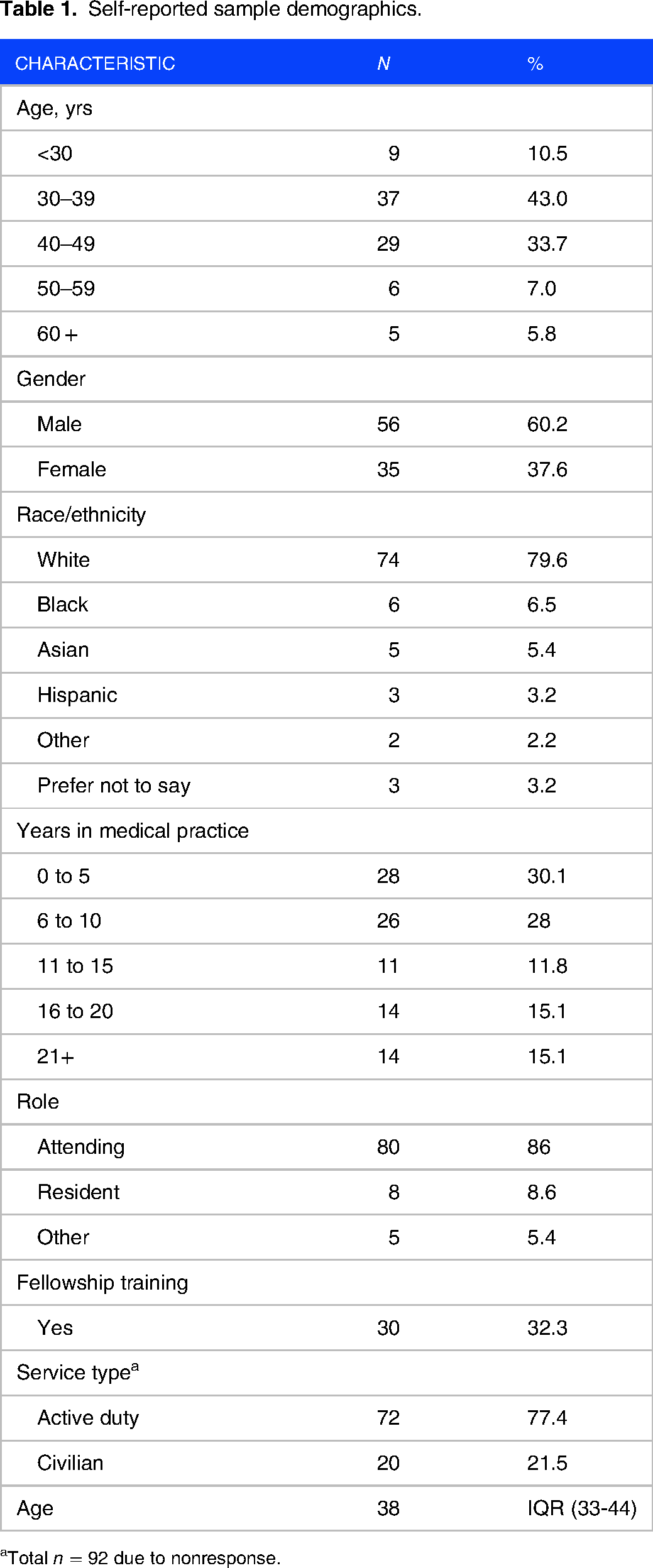
Total n = 92 due to nonresponse.
The mean CIP score was 59 (SD = 16), indicating moderate IP experiences. In total, 9 respondents (9.7%) had few IP experiences while 41 (44.1%) had moderate IP experiences. More than a third of the sample (n = 33; 35.5%) had frequent IP experiences and 10 respondents (10.8%) had intense IP experiences. An analysis of variance revealed no significant differences in IP score based on self-reported gender or race (both P > .05). There was no difference in IP score between surgical and nonsurgical respondents, nor between those with and without fellowship training (both P > .05).
We performed a post hoc power analysis to determine if the lack of difference based on gender was due to the modest sample size and lack of statistical power. The analysis revealed that based on observed means, a sample size of approximately 1372 would be needed to obtain the standard 0.80 level of statistical power. Results confirmed that our sample size was adequate to detect differences based on gender. Thus, it is unlikely that the limited sample size limited the significance of our statistical comparisons.
Mean IP score by age categories is depicted in Figure 1. Differences in IP scores were found with respect to both age and experience (both P < .01). Older age and longer experience were associated with lower IP scores. The measures of effect size for age and experience were η2 = 0.19 and η2 = 0.19, respectively. This indicates a large effect for each characteristic on the IP score. Additional differences in IP scores were noted between active duty and civilian respondents (P < .01; η2 = 0.12). Active-duty respondents had a mean IP score of 62 (SD = 16) and civilian respondents had a mean IP score of 49 (SD = 12). Table 2 shows mean CIP scores by subgroup.
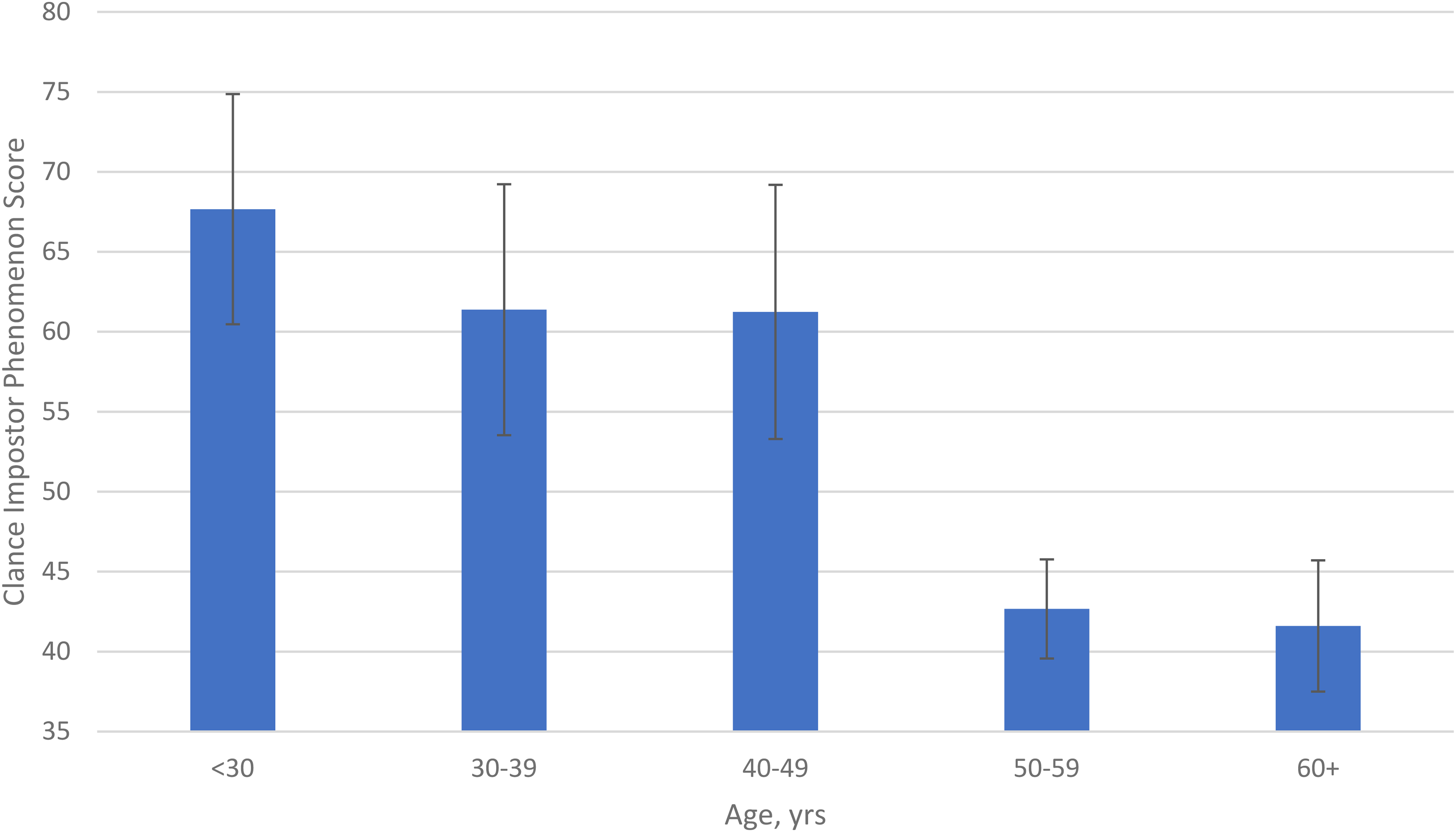
Mean Clance impostor phenomenon score by age category.
Mean clance impostor phenomenon scale (CIPS) scores.

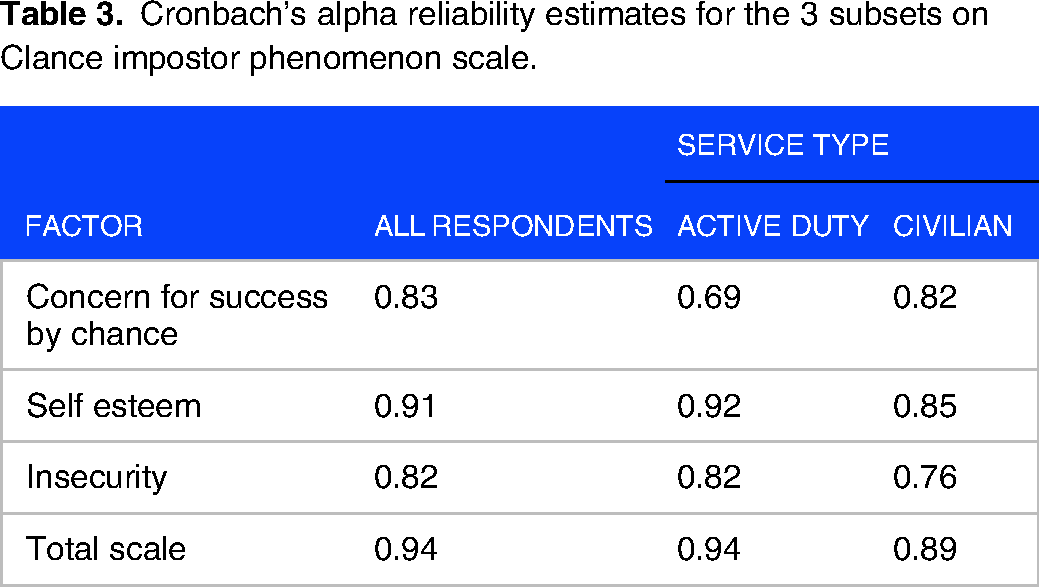
Finally, an Exploratory Factor Analysis was conducted to determine what, if any, underlying thematic structure exists in the survey data. KMO measure of sampling adequacy (KMO = 0.90) and Bartlett test (P < .001) indicated sufficient common variance among the variables for factor analysis. The analysis revealed three factors accounted for 54.1% of the variance in the survey items: self-esteem, concern for having achieved success by chance, and insecurity. Cronbach's alpha for the survey was 0.94, indicating high internal consistency among the three identified factors as indicated in Table 3.
Cronbach's alpha reliability estimates for the 3 subsets on Clance impostor phenomenon scale.
The three factors identified in the exploratory factor analysis were assessed by the following questions in order of strength of correlation: self-esteem (questions items 13, 15, 6, 14, 20, 4, 18, 17, 12, 1, and 3), concern for having achieved success by chance (questions 11, 9, 5, and 2), and insecurity (questions 10, 16, 7, 19, and 8). Like the overall IP score, no differences were found among any of the individual factors based on gender, race/ethnicity, fellowship training, or specialty (surgical vs nonsurgical). In contrast, respondent age was associated with lower IP scores across all factors (all P < .05), indicating as age increases, IP scores decrease. Figure 2 shows mean survey responses by factor and age. Years in medical practice were associated with significant improvements in self-esteem and concern for having achieved success, both P < .01. We found no differences in mean responses for insecurity based on the number of years in medical practice, P = .09.

Mean survey responses by factor and age.
Discussion
To the authors’ knowledge, this is the first study to evaluate the prevalence of IP within a physician population in the military health system. We hypothesized that we would see similar gender differences in the prevalence of IP in a military population and that active-duty military physicians would have higher rates of IP than civilian physicians, regardless of gender. While we did find that active-duty physicians had higher mean IP scores when compared to civilian counterparts, we did not find gender differences in the prevalence of IP. Among all physicians at this Military Treatment Facility, 44% of respondents had moderate IP experiences. Age and a higher number of years in practice were associated with lower IP scores.
The prevalence of IP varies across the literature, with rates cited ranging from 22% to 60%. 17 Given this range, it is difficult to compare the extent of IP between military and civilian physicians, though within our sample size, military physicians had significantly higher IP scores, and thus more intense IP experiences compared to civilian counterparts at our institution. Other than the finding noted by Shanafelt et al which found higher burnout among individuals in active military practice and veterans’ hospitals, there are no studies that have evaluated IP in the military healthcare system. 12 Physicians practicing within a military health system face unique stressors such as the threat of deployment, schedule instability secondary to the deployment of colleagues, and military-specific training requirements which may account for higher burnout among military and veterans’ physicians as noted by Shanafelt et al. 12 These unique stressors may be a contributor to the higher CIPS scores noted among the military physicians in our study.
Our findings are also consistent with those reported in academic literature, in that IP is more prevalent among younger and less experienced physicians.6,7 Given that this phenomenon has been described among multiple studies in medical education, we should start to anticipate that learners and those undergoing life transitions, such as starting medical internships, graduating residency, or starting a medical practice, will have IP experiences. Utilizing mentorship or coaching in this setting may aid in combating IP, particularly among those early in their career.
The strengths of this study include the first application of the CIPS tool within a military population with Chronbach's alpha score demonstrating reliability within this population. This allowed us to reliably identify the prevalence of IP within our study population and serves as a conversation starter about IP in our institution. Fast completion time did not impact scores as we found no correlation between time spent completing the survey and CIP score. Lastly, the providers responding to the survey came from a broad range of both surgical and nonsurgical disciplines, ensuring a representative sample of medical professionals.
Limitations to our study include our response rate. Those individuals who elected to complete this survey maybe those who have IP tendencies, thus selection bias for the topic of interest may have occurred. This study was conducted at a single institution and the majority of respondents were attending physicians; therefore, we cannot apply these findings to all military physicians at large. While our findings may not be generalizable, they highlight that IP is more prevalent in members of the Armed Services versus civilian employees in our organization. Lastly, due to the novel nature of the study, we lacked established variance data with which to run an a prioi power analysis. Consequently, the sample size was determined by the response rate. Although a post hoc power analysis demonstrated the validity of our results, a larger sample would have permitted more detailed subgroup analyses.
Conclusion
This study underscores the pervasiveness of IP experiences in a healthcare setting and indicates concordance with previously published data. IP is not limited to certain subgroups or gender identity but rather is a common issue which may negatively affect a physician's well-being. This study provides an initial step toward a discussion of IP within our organization and beyond and conversations can begin in Grand Rounds and Faculty Development events. Additional research is needed across the military health system to identify those experiencing IP and those at the highest risk of burnout. Additional research is needed to determine protective or compensatory behavioral traits among individuals with low CIP scores as well as characteristics associated with high CIP scores. Regardless, having honest conversations regarding IP and its effect on medical providers across all levels of training and practice will help to shape the future of medicine.
Footnotes
Acknowledgments
Dr Pauline Clance for her guidance regarding IP and permission to use the CIPS in our study population at Clance Impostor Phenomenon Scale (CIPS). From The Impostor Phenomenon: When Success Makes You Feel Like A Fake (pp. 20-22), by P.R. Clance, 1985, Toronto: Bantam Books. Copyright 1985 by Pauline Rose Clance, PhD, ABPP. Use by permission of Dr Pauline Rose Clance. Do not reproduce/copy/post online/distribute without permission from Pauline Rose Clance. Approved link to the CIPS available at ![]() .
.
Ms. Jennifer Kuntz, Womack Army Medical Center medical librarian, for assistance in journal formatting and submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.