
Abstract
OBJECTIVE
Increasing workforce capacity to provide knowledgeable, skilled, and affirming care for transgender and gender diverse people is critical to reduce health inequities; however, few clinicians receive sufficient training on this topic. This article describes Advancing Excellence in Transgender Health (AETH), an annual international conference that offers continuing professional development on evidence-based medical and behavioral healthcare for transgender and gender diverse people across the lifespan
METHODS
Registration data and post-conference evaluation data were descriptively analyzed to assess conference reach, participant satisfaction, and participant intentions to change practice.
RESULTS
Between 2015 and 2022, AETH trained 2677 participants from all US states and 24 countries. Based on post-conference evaluations, 2017-2022, participant satisfaction was high (mean ≥4.4 on a 5-point scale) on all measures, including meeting learning objectives, quality of presentations, and relevance to practice. Participants reported intentions to: implement new information or skills (86.7%); create or revise protocols, policies, and/or procedures (63.2%); and seek additional information (64.2%). To increase equity, the conference waives fees for transgender and gender diverse participants and offers free online sessions. The conference also holds sessions specifically for transgender and gender diverse participants to promote opportunities for community-building, self-care, and professional networking.
CONCLUSION
The broad reach of AETH demonstrates a large demand for more continuing professional development on transgender and gender diverse healthcare. This conference has expanded the availability of training designed to increase and enhance clinical workforce capacity to meet the health needs of transgender and gender diverse communities in the US and across the world.
Keywords
Introduction
Transgender and gender diverse (TGD) people have gender identities that do not correspond with their sex assigned at birth based on societal norms. Although definitions vary, here we define transgender people as having a binary gender identity (ie, girl/woman or boy/man), and gender diverse people as having a gender identity beyond the binary gender paradigm, including people who identify as nonbinary (ie, having a gender identity that does not correspond to the two traditional categories of girl/woman or boy/man), gender fluid (ie, having a gender identity that changes over time), or as agender (ie, having no gender identity). Some people identify as both transgender and gender diverse. Widespread societal stigma and discrimination adversely impact the health of TGD people and increase barriers to accessing providers with skills in administering and managing gender-affirming hormone therapy.1–7 Research indicates that the receipt of gender-affirming care (ie, “health services to support a person's process of living and being perceived in alignment with their own gender identity and expression” 8 ) improves quality of life and mental health outcomes for TGD people,6,9,10 yet the number of clinicians trained to care for TGD people lags behind the demand.4,11–14 Most medical undergraduate and graduate programs offer minimal, if any, curricular hours specific to TGD healthcare, and no programs offer medical residencies in TGD-specific care.12,15–18 Health professional organizations, such as the American College of Physicians and American Medical Association, and global organizations such as the World Professional Association for Transgender Health (WPATH), 19 have recognized the need for more educational interventions to enhance clinicians’ knowledge of and skills in TGD healthcare. 16 To improve TGD patient access to knowledgeable gender-affirming care, it is critical to increase the availability of continuing professional development in TGD healthcare.
This article describes the development, design, reach, and evolution of Advancing Excellence in Transgender Health (AETH), an annual continuing professional development conference started in 2015 that aims to increase the capacity of clinicians and other members of healthcare teams to deliver best practices in gender-affirming medical and behavioral healthcare for TGD people across the lifespan. We present findings from post-conference evaluation surveys on participants’ satisfaction and intentions to change practice.
Methods
AETH Conference Setting and Development
AETH was developed by the Division of Education and Training at The Fenway Institute (TFI), Boston, MA, an interdisciplinary center for research, education, training, and policy focused on optimizing the health of sexually and gender diverse people and those affected by HIV. TFI is a program of Fenway Health, a federally qualified health center that has pioneered gender-affirming care protocols and has expertise in providing high-quality care for TGD communities.20,21 TFI's Division of Education and Training specializes in developing and delivering educational training and resources on sexually and gender diverse health for healthcare organizations, including federally qualified health centers, academic and community hospitals, student health clinics, and other healthcare organizations across the US and internationally. In 2015, TFI initiated the AETH conference in response to a high volume of requests from its networks for more in-depth, comprehensive training on TGD health.
The data for this study were originally collected as program evaluation data not intended for generalizable human research or publication. The Fenway Community Health Institutional Review Board (IRB) granted the authors a memorandum stating that if the project had been prospectively reviewed, it would have been deemed not human subjects research and therefore excluded from participant consent and IRB review per 45 CFR Part 46.
Curriculum Design
The principal goal of AETH is to prepare interdisciplinary healthcare teams to provide TGD care that is grounded in current research evidence and evidence-based standards of care. Specifically, the conference aims to train clinicians on: (a) the routine primary medical and behavioral healthcare needs of TGD patients (eg, tailoring prevention screening based on current anatomy; addressing the impact of stigma and discrimination on mental health); (b) culturally responsive communication and environments (eg, using correct pronouns and names; mitigating implicit bias in patient interactions; using gender-inclusive language on forms); and (c) medical care specific to affirming the gender identity of patients (eg, managing gender-affirming hormone therapy as well as gender-affirming surgery referrals and follow-up; supporting patient autonomy in medical decision-making). The conference also aims to support healthcare teams in developing a patient-centered and integrated model of care that welcomes, values, and affirms gender diversity. The conference designers prioritize a holistic approach to TGD care by emphasizing the integration of primary medical and behavioral healthcare, and by recognizing the importance of systems-level data collection and application to promote continuous quality improvement at healthcare organizations. To promote integrated care, the conference encourages interdisciplinary teams of healthcare clinicians and staff to attend together, although registrants may also attend individually.
AETH is led by three co-directors in collaboration with four programmatic and administrative staff. Most members of the AETH team have lived experience as TGD people. The co-directors have a combination of expertise in TGD-focused primary medical care, behavioral healthcare, and research. Each year, the AETH team refines the core curriculum and agenda based on the previous year's evaluation data and on recent advances in TGD healthcare. The AETH curriculum takes a comprehensive approach, offering sessions on a broad array of topics relevant to medical and behavioral healthcare, as well as interdisciplinary and non-medical topics (Table 1). Each year, the conference adds between three and seven new session topics in response to participant requests as well as emerging research and topics.
Topics covered in the Advancing Excellence in Transgender Health conference, 2022.
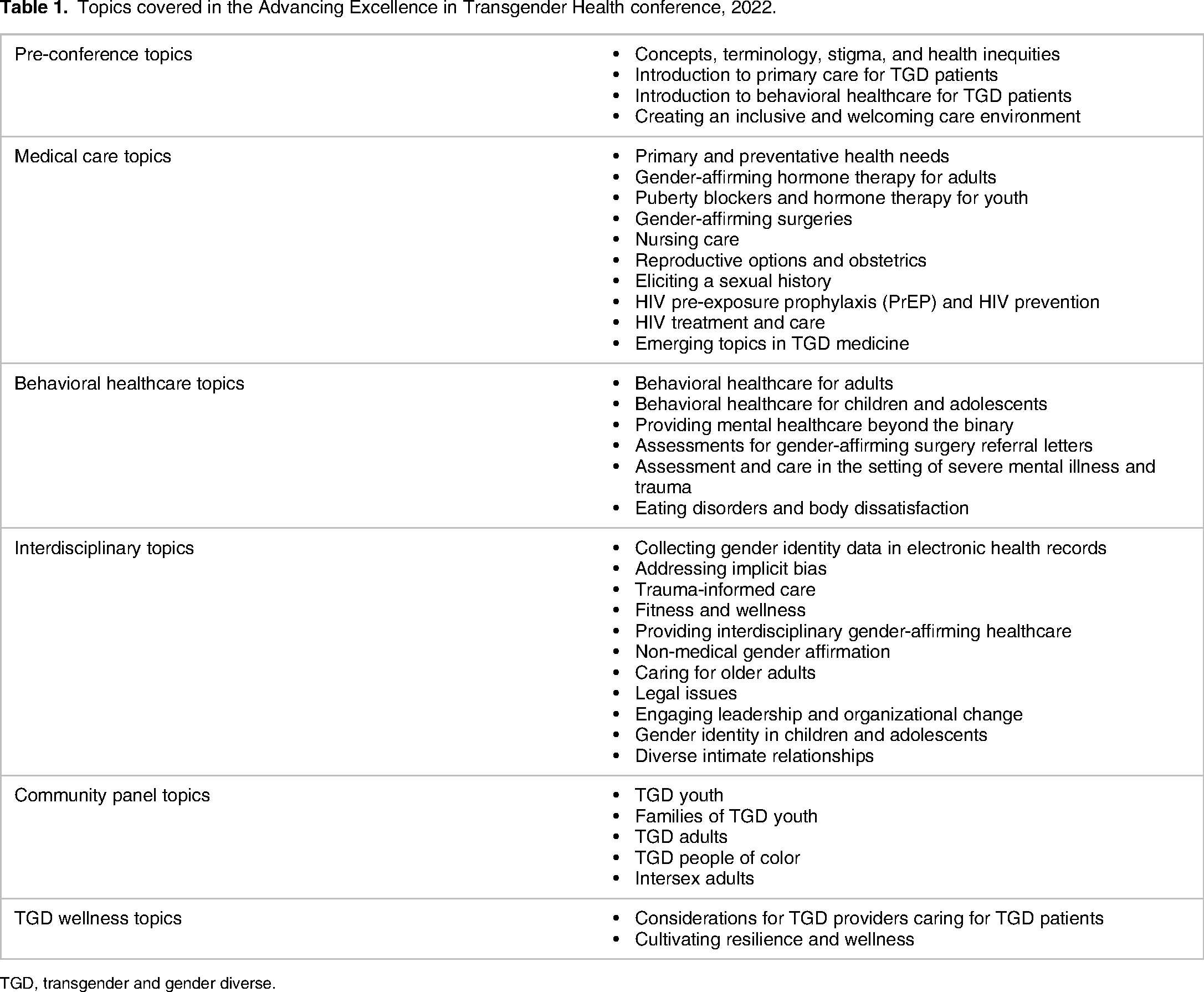
TGD, transgender and gender diverse.
To identify qualified speakers, the course directors select experts in TGD health from within Fenway Health, Harvard Medical School (HMS), and national networks of clinicians, researchers, and community members. As part of this process, the co-directors ensure that presenters represent a range of TGD identities and diverse racial and ethnic identities. To meet the goals of the conference, AETH staff provide guidelines to presenters on ways to develop content through an intersectional and health equity lens that promotes TGD patient well-being and resilience. Nearly all speakers receive high evaluation scores and are asked to return each year to present on their topic of expertise, with refinements as needed based on participant evaluations and new research evidence. While about 80% of speakers return each year, the remaining 20% have scheduling conflicts or changes in career priorities that prevent them from returning. On rare occasions, a speaker is not invited to return due to low evaluation scores.
Conference session formats include: (a) didactic presentations, with case studies and discussion, led by one or two speakers with expertise in TGD-focused patient care or research; (b) facilitated community panels consisting of three to five TGD people, and sometimes family members, who share their lived experiences with accessing and engaging in healthcare; (c) expositions, poster sessions, and networking opportunities; and (d) sessions exclusively for TGD participants as a way to build networks of social and professional support among TGD people working in healthcare. Some sessions occur simultaneously to allow time for all priority topics to be featured throughout the conference.
In 2015 and 2016, TFI piloted AETH as an in-person two-day conference at Fenway Health, Boston, MA, for a maximum of 130 participants. As demand for attending the conference exceeded capacity, TFI started hosting the conference at offsite Boston-based facilities that could accommodate a larger audience as well as concurrent breakout sessions. In addition, the conference expanded to three days and began a partnership with the HMS Continuing Education (CE) program. HMS CE now oversees the registration system, markets the conference, and offers CE credits for physicians and nurses through the Accreditation Council for Continuing Medical Education and American Nurses Credentialing Center's Commission on Accreditation. Each year the conference also receives accreditation to provide CE credits to social workers, mental health counselors, and psychologists. With the onset of the COVID-19 pandemic in 2020, TFI moved the conference from in-person to a virtual meeting platform, allowing for larger numbers of participants while enabling continuation of the same conference structure and content.
Each year, following the conclusion of the conference, TFI posts free recordings of all conference sessions to its website. Providing cost-free online access to conference recordings helps to broaden conference reach and promote equity. During the years of in-person meetings, TFI hired a production company to record the presenters in a studio with green screen technology so that slides could be superimposed next to the speaker. Once the conference moved to a virtual platform, we recorded the presenters and panelists, with their permission, directly from the platform. TFI staff post all recordings on the National LGBTQIA + Health Education Center website, enabling any user to watch a session and receive CE credits. Having the recordings on the website also allows conference participants to view sessions they could not join due to attending a concurrent session.
Study Design and Measures
Enrollment
To measure participant enrollment frequencies and geographic origins, we extracted conference registration data from the AETH registration system between 2015 and 2022.
Post-conference surveys
We used a cross-sectional study design to evaluate participants' self-reported outcomes of the AETH conference between 2017 and 2022. We did not include evaluation outcomes from 2015 to 2016 because we started using a different post-conference evaluation survey in 2017. TFI created the post-conference evaluation survey using items developed by TFI for our other professional development courses, as well as items developed specifically for the AETH conference. When we began collaborating with HMS CE in 2018, we added HMS CE standard evaluation survey questions. The survey measured the domain of “participant satisfaction” (subdomains: content quality, ethics, and evidence base) with six 5-point Likert scale items and two yes-no items. The domain of “intentions to change practice” was measured with two multiple-choice questions, one focused on intentions to change, and one on barriers to change. The AETH survey has not been validated or pilot-tested.
Immediately post-conference, participants received a link to the online survey developed within HMS CE proprietary software. Completion of the evaluation survey was anonymous and was required of participants seeking to receive CE credits, although all participants were encouraged to complete the survey.
Evaluation analysis
To analyze the survey responses, we extracted survey data from the HMS CE system and exported the data into Microsoft Excel. For all survey questions, we combined data from all years in which a given question was used. To analyze Likert scale items, we coded responses from 1 to 5, and calculated the means.
Recorded sessions
To measure participation in web-based recorded conference sessions, we extracted data from our website's learning management system and exported the data into Excel. We did not include evaluation data of recorded sessions in this study's data analysis for two reasons: (a) the experience of watching a recorded, asynchronous, single presentation is considerably different than actively participating in a multi-day, multi-session conference and (b) the evaluation survey questions for online recordings differ from the questions in the post-conference survey.
Results
Attendance and Reach
From 2015 to 2022, the annual AETH conferences engaged 2677 unique participants. Of these participants, 2505 (93.6%) attended the conference only once and 172 (6.4%) attended at least twice. All in-person conferences reached maximum capacity for participation. The most frequently reported professional roles of participants were: physician (30.9%), nurse (16.2%), nurse practitioner (12.9%), social worker (9.6%), physician assistant (4.1%), psychologist (3.6%), counselor (2.8%), and other (19.9%). Additional professions in attendance have included administrators, pharmacists, students, researchers, nurse midwives, and speech pathologists, among others. TGD community members who do not work within the healthcare sector have also attended as a way to invest in their own community's well-being. Bringing in more people with lived experience, and inviting them to contribute their perspectives to post-presentation discussions, enriches the learning for all participants.
Participants hailed from all 50 US states, Washington DC, Puerto Rico, and Guam; additionally, 99 (4.0%) participants attended from 23 non-US countries, approximately 50% of whom were from Canada (Figure 1).

Maps Data: Google, ©2023. Countries represented by participants of the Advancing Excellence in Transgender Health conference, 2015‐2022.
Between 2020 and 2022, 3296 unique users completed watching at least one online recorded AETH conference session.
Post-conference Evaluation Outcomes
Evaluation survey response rates ranged from 42% to 62% of participants each year, with an average response rate of 48% across all years. Participant satisfaction with the conference quality was high (4.4 to 4.7 on a 5-point scale) on all measures, including “meeting learning objectives,” “quality of speaker presentations,” and “relevance to practice” (Table 2). Satisfaction ratings differed by no more than 0.3 points between years. Additionally, over 99% of participants agreed that the conference content was “evidence-based” and “fair, balanced, and free of commercial bias.”
Post-conference evaluation responses regarding the quality, ethics, and evidence base of the Advancing Excellence in Transgender Health conference, 2017-2022.
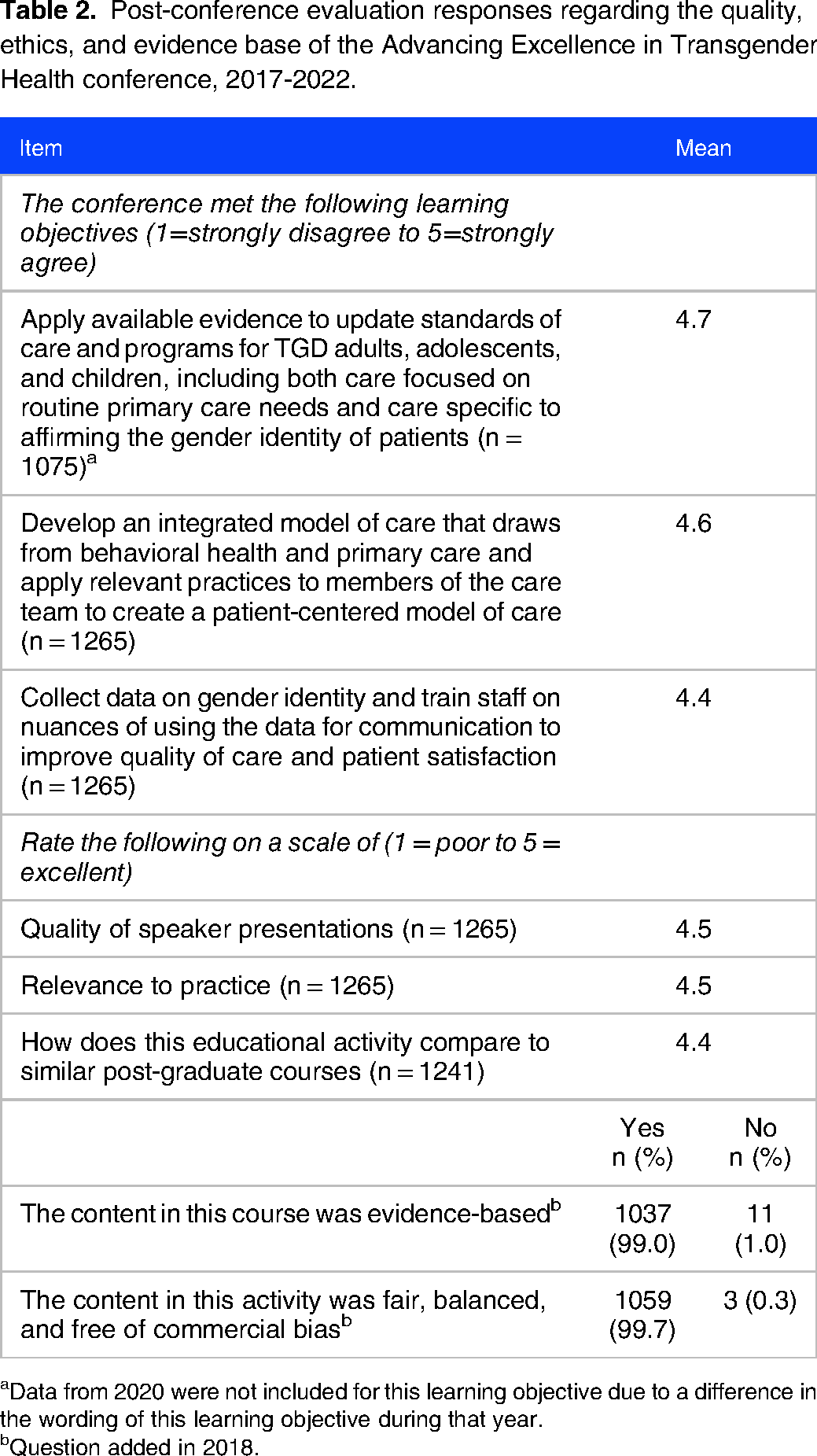
aData from 2020 were not included for this learning objective due to a difference in the wording of this learning objective during that year.
bQuestion added in 2018.
In response to the question, “What impact will this activity have on your practice or with your healthcare team?” (Table 3), 86.7% of participants reported an intention to “implement new information or skills in the care of TGD patients,” 63.2% reported they would “create or revise protocols, policies, and/or procedures,” and 64.2% reported they would “seek additional information.” Only 8.5% reported they would not change their practice, due to “system barriers” (6.0%), having “no patient contact” (1.7%), or believing “the content was not convincing enough” (0.8%). When asked about potential barriers to implementing changes, 43.7% of participants indicated “institutional barriers,” while about a third reported “lack of time” (34.4%), “communication or collaboration challenges among their care team” (31.5%), and “insurance or financial issues” (29.7%). Few participants cited patient-related barriers to implementing changes, such as “lack of patient knowledge” (6.2%) or “adherence” (4.2%), and “adverse side effects” (1.6%).
Post-conference evaluation responses regarding intentions to change practice: Advancing Excellence in Transgender Health conference, 2019-2022.

Innovations and Adaptations
Over the years, the AETH course directors and programmatic staff have made adaptations to the conference in response to suggestions and feedback from participants, and based on emerging research, practice, and shifts in cultural understanding of TGD identities and health. For example, the conference has over time added sessions that are relevant to intersex communities, dedicated to families of TGD youth, and focused on intersectionality among TGD people of color. We have also increased the number of community panels offered. Panels build empathy through personal narratives, increase sensitivity to diverse TGD healthcare experiences and priorities, and highlight opportunities for improved communication and delivery of care with TGD patients. 22
Another key modification was to increase conference access for TGD clinicians and students who, as a marginalized community, may not have the financial means to attend the conference. To achieve this goal, in 2019 TFI staff began waiving the conference tuition fee for all TGD participants. Additionally, we created breakout sessions open only to TGD people. The purpose of dedicating space for TGD participants was to promote opportunities for solidarity, networking, and engaging in self-care.
Recognizing that conference participants enter with varying levels of existing knowledge and skills, in 2019 we created an optional half-day preconference to cover introductory-level TGD health content on foundational concepts and terminology, essential epidemiology, and core principles of gender-affirming care. In 2021, we also added a virtual poster session to highlight emerging research in the field of TGD healthcare. To solicit posters, conference organizers released a call for abstracts several months before the conference. The conference team then reviewed the posters for quality and accepted nine posters each year. Posters have covered a broad range of topics, including research on gender-affirming surgical techniques, violence and mental health outcomes among Asian American transgender adults, sexual and reproductive health counseling in transgender adolescents, and body mass index as a barrier to gender-affirming surgery.
Discussion
The AETH conference is unique in providing wide-ranging continuing professional development on the clinical care of TGD people across the lifespan. Between 2015 and 2022, AETH trained 2677 healthcare professionals and students through its conference proceedings. Additionally, 3296 people completed watching at least one recorded web-based AETH session between 2020 and 2022. The continuous engagement of new audiences for AETH speaks to the demand for TGD clinical training.
As of 2023, TFI and HMS plan to continue organizing annual AETH conferences and to refine and update the curriculum based on evaluation results, research findings, and changes in the healthcare environment. We will consider offering the conference in-person again, depending on the state of the COVID-19 pandemic. While virtual conferences have several benefits, such as accommodating more participants and eliminating travel costs, the open-text feedback from our evaluation survey indicates that many participants value having in-person interactions with presenters, peers, and community members. To expand access and choice, we could in the future offer a hybrid conference so that participants can choose to attend in person or virtually.
We recognize several areas for growth. Now that more clinicians have received introductory-level training and have real-world experience with TGD patients, we will consider offering advanced-level medical and behavioral health tracks. Another consideration is to provide more experienced participants with training and resources that will in turn equip them to educate colleagues at their own organizations. As shown in the evaluation survey results, many participants reported institutional barriers and challenges in collaboration with members of their care team. Train-the-trainer workshops that prepare organizational “champions” to lead local training programs and act as change agents could help to overcome some of these barriers.23,24 In addition, future evaluation surveys could ask participants to complete open-text responses to specify the barriers they expect to encounter.
AETH should be viewed within the greater arena of professional development on TGD healthcare, as participation in one conference cannot fully prepare a clinician to provide comprehensive care. As found in the evaluation survey, two-thirds of participants intended to seek additional information after the conference, thus demonstrating a need for more TGD health resources and training programs. Examples of such programs include the WPATH clinical training program on the WPATH Standards of Care, 14 and the University of California San Francisco's Center of Excellence for Transgender Health multidisciplinary clinical training tracks that occur the day prior to its biennial research and policy conference. Several medical professional organizations offer online TGD training opportunities, 16 as does our organization, the National LGBTQIA + Health Education Center, which, in addition to the AETH session recordings, produces free TGD health-focused webinars and publications and operates a Project Extension for Community Healthcare Outcomes (ECHO) on TGD health 25 that emphasizes participant-led case discussions and peer-to-peer knowledge sharing. 26
Our conference evaluation had several limitations. First, we collected only post-conference survey data. Although we could not calculate pre/post changes in knowledge or perceived skills, we did measure intention to change practice, which is associated with behavioral change among health professionals.27,28 Additionally, we did not perform validity, reliability, or pilot tests of our evaluation survey.
Another limitation was that only 48% of AETH participants were represented by the evaluation data. Because CE credits were contingent on completing the evaluation survey, clinicians may have been over-represented among survey respondents as compared to administrators, researchers, and allied health professionals. Efforts are underway to increase future evaluation response rates from non-clinician participants.
Conclusion
Expanding clinical workforce capacity to care for TGD people across the world is critical, given this population's stark health inequities, unique medical care needs, and limited access to clinicians trained to serve them. The AETH conference serves as an important component of the growing continuing professional development resources on culturally responsive and evidence-based medical and behavioral healthcare for TGD people. Further, the AETH conference model could be replicated to meet ongoing global needs for continuing education on TGD clinical care. To adapt the AETH model, experienced gender-affirming care organizations could recruit local subject matter experts, within a given region or country, in order to facilitate culturally specific tailoring of content, representation of local perspectives and priorities, and local professional community building. Ultimately, the goal is to increase the capacity of healthcare teams globally to deliver evidence-based, culturally responsive gender-affirming medical and behavioral healthcare for TGD communities.
Footnotes
Acknowledgements
We extend our thanks to the Massachusetts League of Community Health Centers for their support of the conference. Thank you also to Michele Hatchell of The Fenway Institute for designing the figure, and to Ayanna Besson of The Fenway Institute for assistance with the analysis.
Authors’ Contributions
Conceptualization: all authors; methodology: S Mitnick; data analysis: S Mitnick, J Bruno, and H Goldhammer; writing original draft: H Goldhammer; Writing–review and editing: all authors; funding acquisition: AS Keuroghlian; supervision: AS Keuroghlian
Declaration of conflicting interests
AS Keuroghlian and SL Reisner declared royalties as editors of a McGraw Hill textbook on transgender and gender diverse healthcare. All other author(s) declared no relevant conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Grant U30CS22742 from the Health Resources and Services Administration Bureau of Primary Health Care to Dr A. S. Keuroghlian, the Principal Investigator. The funder was not involved in the writing of the article or in the decision to submit the article for publication.