
Abstract
Objective
This study measured the effect the experience of house calls might have on third-year medical students.
Methods
Students were surveyed via an anonymous online survey at the start of their geriatrics clerkship, again at the end of their clerkship, and once more three months later. Empathy was measured using the Jefferson Scale of Empathy – Student version (JSE) and student attitudes towards the geriatrics population was measured using the UCLA Geriatrics Attitudes Scale (GAS). Data were analyzed using SPSS version 27.0.
Results
No changes in empathy were found when comparing students who completed house calls versus those who did not. However, students who trained in office settings were noted to have higher JSE scores at the three-month follow-up survey, students who worked in hospital settings had higher JSE scores at the completion of the clerkship, and student who worked in assisted living facilities had higher GAS scores at the completion of the clerkship.
Conclusions
Teaching students ways to improve empathy can be challenging. The setting in which a student trains may be an area of focus for improving empathy among trainees and should be researched further.
Keywords
Introduction
Empathy is defined as “a personality trait that enables one to identify with another's situation, thoughts, or condition by placing oneself in their situation.” 1 For decades this ability has been acknowledged as a crucial skill for healthcare professionals when evaluating the patient–doctor relationship 2 as well as patient satisfaction and clinical outcomes – both of which have been found to improve with increasing physician empathy.3,4 Given the significant role that empathy can play in medical student education, several studies have examined the ways to measure empathy in medical students. 5 Additionally, over the years, several studies have found that empathy in medical students tends to decline throughout training,6,7 This decline seems to be especially true for students in their third year of medical school.8–10 Though a cause is not yet known, one recent study suggests it is the routine of patient care leading to a decrease in empathy. 11 Other causes may be less apparent such as mistreatment by superiors, social support issues, high workload, short length of stay of the patient, and poor learning environments. 6 This decline in empathy through years of training, and the proven importance of the role empathy plays in patient care, has led to attempts to teach empathy to medical students.12,13 While this can be a difficult skill to teach, studies have shown that some of these interventions have positive effects on empathy.12,14–16
As medical school progresses and students move from a classroom setting to a clinical setting, they begin to experience more of what it means to be a physician with professional and emotional responsibilities of patient care. One might think that this new learning environment would ignite a passion for their chosen field, however, studies have shown that third-year medical students have significantly higher levels of emotional exhaustion and depersonalization as well as lower levels of personal accomplishment in comparison to first-year medical students. 17 Third-year medical students also had higher regrets about entering medical school than first-year students. 17 As medical students progress through school, a greater proportion report decreased empathy and decreased idealism, and with this comes a greater risk for burnout. 17 While the exact cause of this decline is unknown it could, at least in part, be due to students’ varying experiences through their clinical rotations as prior research has shown learning environments can affect empathy. 6 In particular, one clinical experience that may vary greatly among students is making house calls. While, historically, house calls were commonplace in the United States, advances in technology and changes in the delivery of healthcare have led to decreases in home-visit popularity. However, with a growing geriatric population, better reimbursement, and a focus on reducing hospitalization, house calls have once again started to gain traction over the last couple of decades.18–20 With this increase in house calls, there has also been an increase in opportunities for medical students to travel with a physician to the patient's home to evaluate and treat their medical, social, and emotional needs while seeing exactly how a patient lives. It is hypothesized that this experience could potentially improve medical student empathy, although to date there have been few studies looking into the effect house call experiences have on this important physician trait. However, several studies have evaluated this effect through narrative essays or unvalidated surveys and some studies have assessed student attitudes and knowledge of social determinants of health among other topics after house call experiences.21–27 Validated empathy or attitude surveys have been used to assess medical students’ empathy, but they have not often been used to assess students’ empathy on house calls and could prove to provide further information on the impact the house call experience has on medical students’ empathy.8,28 Additionally, while research has shown improvements in general attitudes towards caring for older individuals following home visits 26 there is a lack of information on whether those positive attitudes correlate with increased empathy. Accurately knowing the effect of this experience could impact medical school curricula and the amount of time students spend on home care clerkships. This study set out to determine if experiencing house calls during a geriatrics rotation could be associated with increased empathy and attitudes towards older individuals in third-year medical students.
Methods
This study was conducted from July 2018 through June 2019 at Rowan University School of Osteopathic Medicine and was approved by the university's Institutional Review Board on May 15, 2018 (Study ID: Pro2018002355). Data were collected from third-year medical students participating in the four-week-long geriatrics clerkship via an anonymous digital survey. All students over the age of 18 and completing the geriatrics clerkship during the study timeframe were included. Any students not meeting these criteria were excluded. During the clerkship, students were assigned to clerkship sites throughout the state of New Jersey and worked in a variety of settings including inpatient hospital settings, outpatient/office settings, assisted living facilities, and long-term care facilities. Additionally, some of these students also accompanied physicians, nurse practitioners, or hospice nurses on house calls. This combination of various clerkship sites and clinical settings allowed for diverse experiences among the students. Assignments were left to the clerkship director to meet the learning needs of the students and were not altered or affected by the researchers. The study was conducted using the Jefferson Scale of Empathy Student version (JSE-S) 29 and the University of California at Los Angeles (UCLA) Geriatric Attitudes Scale (GAS). 30 The JSE-S is a validated, well-established instrument for measuring empathy among medical students. 29 Respondents are asked to answer likert scale questions on a scale of 1 to 7 for questions about empathy in the clinical setting. The GAS is a 14-item questionnaire on attitudes toward older adults and their care. 30 Additionally, students were asked to answer questions about their experiences during the clerkship such as the settings in which they worked, what percentage of patients seen were on house calls, how likely they are to go into geriatric medicine, and how likely they are to incorporate house calls into their future practice. Demographic data including age and gender were collected as prior research has indicated these variables can impact empathy in medical students. 31 Participants were invited via email to complete the survey at the start of the geriatrics clerkship, again at the end of the clerkship, and once more 3 months following the clerkship as illustrated in Figure 1. Surveys were conducted via Qualtrics and partial student ID numbers were used to track surveys across the three points in time in which they were conducted to maintain anonymity. Participation in the study was not mandatory and students who chose not to participate were not penalized in any way. Informed consent was obtained electronically prior to the start of each survey in accordance with IRB protocol. Those who did participate received minimal compensation in the form of electronic gift cards. For completing each of the first two surveys in the complete set of three, each participant received a $5.00 gift card. The participants received a $7.50 gift card for completing the third and final survey. The survey contained a separate link provided upon completion of the survey where the student could enter his or her email address to be compensated and maintain anonymity. Data were analyzed using SPSS version 27. 32

Timeline of surveys.
We used a program published by researchers at UCLA to determine the necessary sample size. 33 All parameters were estimated due to the lack of pre-existing research literature. The minimum number of participants required assuming a low-to-moderate effect size (Cohen d = .25) and Power (1-β error probability) set at .8 would be 95 participants. We anticipated that fewer participants would complete the follow-up surveys, although attempting to estimate rates was complicated since research on attrition from longitudinal studies typically examines rates for in-person data collection and longer timeframes. Given that our study was online (easily accessible with minimum time commitment), we estimated that we would need to recruit approximately 160 participants (40% attrition) to capture 95 participants for all time periods.
Statistical analyses
Repeated measures ANOVAs were used to examine differences in JSE and GAS scores across all time points. Post-hoc tests (Tukey HSD statistic for multiple comparisons) were used to identify statistically significant differences between time points. Potential violations of the equal variance assumption are examined with the Levene statistic. Pearson's bivariate correlation coefficients were used to examine the relationship between JSE and GAS total scores across all three-time points. A conventional p-value of ≤ .05 (two-tailed) was considered statistically significant for all statistics employed.
Results
Scores for all measures and subscales were normally distributed with no extreme outliers, other than two participants who reported low scores on the Compassionate Care subscale of the JSE (ie, > 3 SD from mean). We decided to retain these participants given their scores were otherwise in the normal range for the other subscales, therefore these anomalies were likely due to true variance and not inconsistent or random responding. Levels of inter-item reliability (alpha) were all acceptable (JSE total score α = .87; subscales: perspective taking α = .86, compassionate care α = .81, walking in people's shoes α = .77; GAS total score α = .77).
Of the approximately 191 students in the third-year class, 123 students (62 males, 61 females; 64% of full class) completed the baseline survey, 97 students (49 males, 48 females; 51% of full class) completed the time 2 survey, and 60 students (27 males, 33 females; 31% of full class) completed the time 3 survey. A total of 55 students (29 males, 26 females; 29% of the full class) completed all surveys; see Figure 1.
Scores on the JSE and GAS measures were all significantly correlated (p < .001) at the corresponding collection periods (T1 r = .557; T2 r = .627; T3 r = .450: see Table 1).
Pearson bivariate correlations between GAS (geriatric attitude) and JSE (empathy) scores across time points.

** < .001; * < .05
Repeated measures ANOVAs were used to examine gender differences in JSE and GAS scores across all time points. While there were no significant gender differences in JSE scores, males were seen to have somewhat lower scores across all time points.
However, there were significant gender differences in GAS scores at the first time point (F(1.98, 103.31) = 3.605, p = .03), with males scoring lower. The scores essentially converge by the final time point (ie, no statistically significant differences) indicating that mean scores for males slightly increased while female scores slightly decreased compared to the first time point.
Repeated measures ANOVA analyses were also conducted in order to compare both JSE & GAS indicators (separately) over three time periods. The Levene statistic indicated that the equality of variance (homogeneity) assumption was met for JSE and GAS scores across time points. However, we did not find any statistically significant difference between specializations in either of the scores.
We hypothesized that students with greater exposure to housecall experiences during their geriatric clerkship (second-time point) would develop a stronger sense of empathy and improved geriatric attitudes due to directly witnessing patients’ home environments and interacting with clients in their personal spaces. To examine this hypothesis, we created groups based on the percentage of time spent during a rotation performing home visits, ranging from 0%–19%, 20%–39%, 40%–59%, and 60% or above. The decision to use 20% increments was made during the construction of the original questionnaire in an attempt to simplify the test taker's experience (vs open-end or sliding scale estimates) and the later interpretation of findings. The vast majority of students (n = 102) fell into the first category, with only four students exceeding 20%. Contrary to our expectations, levels of empathy and geriatric attitudes were generally poorer in those who engaged in more housecall activities: JSE M(SD): 107.96(12.17) versus 86.75(7.27); t(104) = 3.453, p = .001; GAS M(SD): 51.73(7.55) versus 41.50(3.70), t(104) = 2.688, p = .008. However, the small number of students (n = 4) in the + 20% house call group limits the generalizability of this finding.
In order to examine if there were any differences between specialty interests among students, we created four combined groups that we labeled (1) Primary Care (ie, Family Medicine, Pediatrics, Preventative care), (2) Ambulatory Surgery (ie, Otolaryngology, Ob/Gyn, Orthopedics, Ophthalmology, Plastic Surgery, Urology), (3) Psychiatry / Neurology, and (4) Other. We conducted a repeated measures ANOVA to evaluate levels of empathy and geriatric attitudes between these four specialty groupings across the three time periods. However, no significant differences were indicated. In light of this, we sought to examine if experiences (or lack of experiences) in specific types of settings (ie, office, hospital, assisted living, housecall, long-term care, sub-acute rehab) during the second time period of data collection were related to levels of empathy or geriatric attitudes at any of the data collection time points during the study. There were only two students who indicated that they never worked in an office setting, which was deemed too small for group comparisons. Of the remaining settings, there were significant relationships to emerge involving hospital and assisted living settings. Specifically, students who spent a portion of their time in hospital settings (n = 92) versus those without hospital experiences (n = 14) reported significantly higher empathy at the first follow-up period: JSE M(SD) 108.32(11.94) versus 99.57(15.06), t(104) = −2.464, p = .015. Students with experiences in assisted living environments (n = 38) versus those without assisted living experience (n = 21) reported more positive geriatric attitudes: GAS M(SD) 52.37(6.35) versus 47.95(7.71), t(104) = -2.369, p = .021. No significant differences were found in either GAS or JSE scores when analyzing house calls, sub-acute rehab, and long-term care settings.
Discussion
As empathy continues to be explored by researchers, gaining insight into the effects various clinical settings have on student empathy can prove to be an important factor in curricular development. The findings of this study suggest that there may be some subtle differences in student empathy based on the location of training during the geriatrics clerkship. Interestingly one of the settings that did not seem to have any impact on empathy was the patient's home. While the sample size was small, students who participated in house calls during their rotation did not show any improvement in empathy or attitudes towards geriatric patients via the JSE and GAS respectively upon completing the surveys at the second and third-time points. This is notable because prior studies have suggested clinical experiences within the patient's home may improve empathy in medical students.21–27 While the findings in this study certainly do not disprove that suggestion, it does raise into question the type of impact house call experiences can truly have on a student and if simply having this experience may have any effect on a student's empathy or attitude, for better or worse. There could be a number of reasons for this. Empathy may be too difficult to change with limited experiences as the rotation length in this study was 4 weeks. Perhaps a longer duration or a greater percentage of rotation time spent in the home setting could make a difference. Students conducting house calls are possibly less likely to experience continuity with their patients whereas students in the hospital setting are likely to see the same patients daily when rounding and possibly developing rapport with said patients. One should also take into consideration the relationship the students have with their superiors during these experiences and the complexity of the patients’ medical history – variables that can be difficult to control. Another factor could be the discipline in which the provider/preceptor works. Students were able to see patients on housecalls while working with several different providers including physicians, advanced practice nurses, and hospice nurses. Given the differences in training among these providers, the experiences of the students could vary as a result. These differences in role modeling could affect how the students view the patients and their relationships as the approach to the patient could vary from a more “team-based approach” with some providers to a more “individual” approach with others. Larger studies are needed to account for these variables and to determine if the prior findings that house calls can potentially improve medical student empathy are accurate.
In looking at other settings, the findings show higher JSE scores in students who spent time in the office and hospital settings and higher GAS scores in students who spent time in the assisted living setting. The reason for these findings is unclear. The assisted living setting is unique in that patients are provided with medical care, but typically reside in their own apartments or room. 34 But how this would differ from the experience of seeing a patient in their own home is not able to be discerned from these results.
As previously demonstrated, 10 the female participants scored higher in empathy than the males at all time points, albeit non-significant in our sample (Figure 2). A similar pattern can be seen in GAS scores, with females scoring somewhat higher at all time points. Interestingly, the difference between the two groups decreases with subsequent surveys (Figure 3). Further study into the effects a geriatrics rotation can have on medical students based on gender should be conducted.
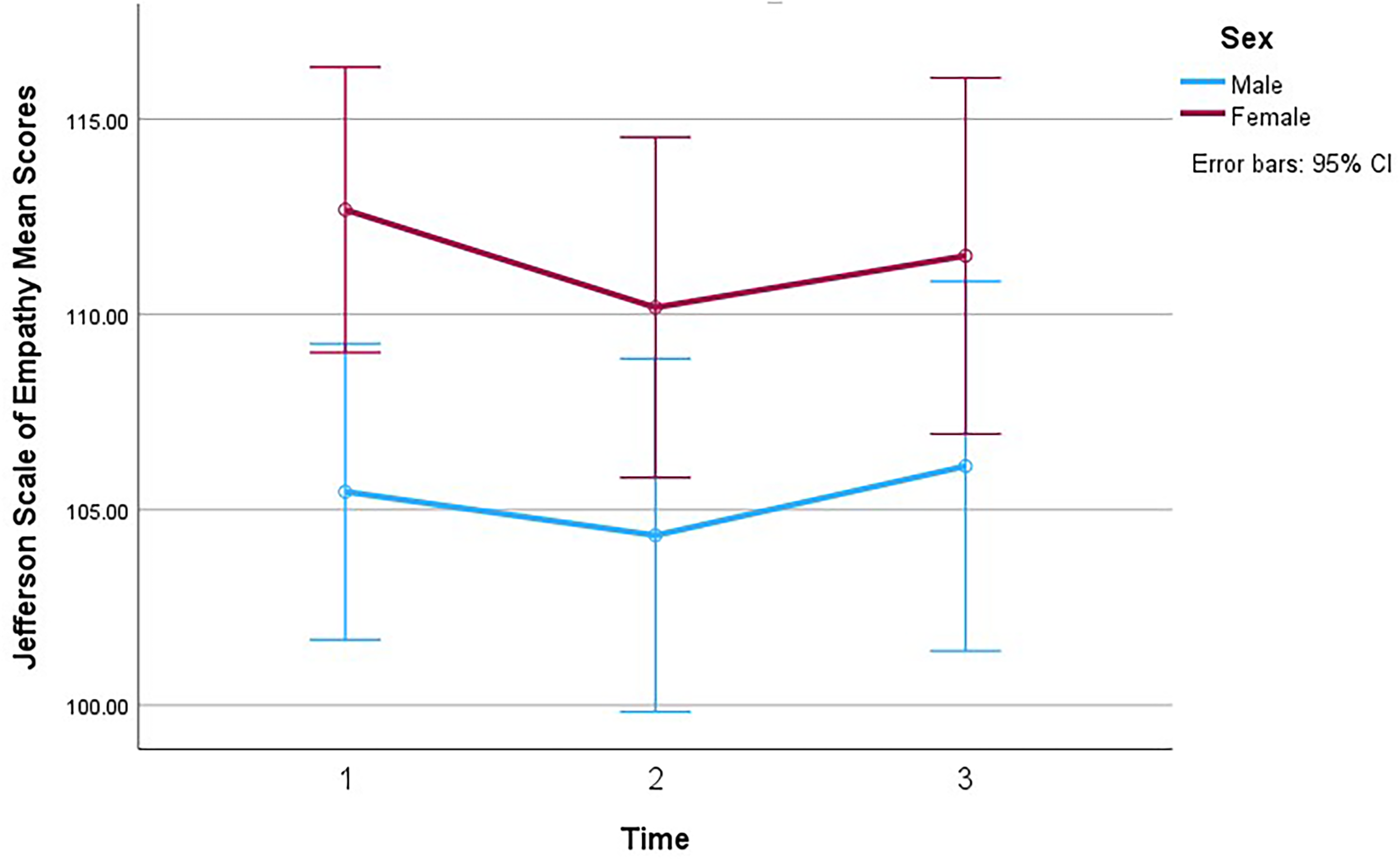
Empathy over time (by gender).

GAS over time (by gender).
It should be noted that this study has several limitations. One such limitation is small sample size. The sample size decreased with each subsequent survey and could have limited the results as the initial goal of 160 subjects was not met. Because students were not randomized to each clinical setting, the amount of time spent in each setting varied among students and could be a factor in the results. Future studies should attempt to randomly assign students to each setting and record time spent in those settings. Future studies should also aim to include multiple schools as this study was a single-center study, further limiting the results.
Another limitation of this study was the survey design. We intended for there to be a more normally distributed range of exposure to various settings and unfortunately, the number of total patients seen via house calls was relatively small. As such our survey, which asked about patients seen on house calls in 20% increments, was not as accurate as we had hoped. Future studies would do well to record patient logs so each patient seen could be accounted for regardless of clinical setting.
One must also consider what factors or variables were not explicitly reviewed in this study. Is there something about the house call experience that impedes the building of empathy? Some things to consider are the act of driving between homes, the limitation of medical resources in a patient's home, and the different dynamics of a physician–patient relationship outside of the standard clinical setting. Possible factors within the hospital and office settings that encourage empathy building should be considered as well. Some things to examine are the continuity of care a student likely experiences when working in an inpatient setting, the familiarity of an office or hospital setting, and the abundance of resources available.
Another variable that could influence these results is prior experience. As the participants were surveyed at different points in time in their third year of medical school, the amount of, and type of, experience varied from one participant to the next. These prior experiences could be a factor in how one views house calls, or other clinical settings, in the context of empathy building.
Conclusion
Teaching empathy to medical students can be challenging and discovering new ways to improve empathy within the curriculum would be a helpful addition to medical education. Further research is still needed to find the cause of empathy decline in the clinical years of medical school. Additionally, the location and setting of a student's training could prove to be a significant factor in empathy development or decline among physicians in training.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231175804 - Supplemental material for Empathy and the Medical Student House Call: The Effect of Clinical Settings on Empathy in Third Year Medical Students
Supplemental material, sj-docx-1-mde-10.1177_23821205231175804 for Empathy and the Medical Student House Call: The Effect of Clinical Settings on Empathy in Third Year Medical Students by Philip B. Collins, Thomas Dinzeo, Jennifer C. Sepede, John F. Bertagnolli and Christian White in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
Permission to use both the Jefferson Scale of Empathy and the Geriatrics Attitudes Scale were obtained from the creators prior to the start of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was internally funded by the department of Family Medicine at Rowan-Virtua School of Osteopathic Medicine
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.