
Abstract
The objective of this review is to critically evaluate the Area Health Education Center Scholars' didactic curricula and determine whether the goal of developing a sustainable rural healthcare workforce is achievable under the program. The didactic curricula from the Alabama, Florida, and South Carolina programs were evaluated using a context-input-process-product model and a mixed-methods approach. Modules were assessed for their content and mode of delivery, and whether the eight competency domains from the Council on Education for Public Health were incorporated. Student evaluations from the 2019–2020 cohort were also examined to identify themes from each module. On average, across modules, nearly all students strongly agreed or agreed that the facilitator had been responsive (97%); that the modules had been clearly outlined (95%), easy to understand (96%), not overly time-consumptive (96%), and relatable to their career (96%); and felt that their understanding had improved (97%) and felt satisfied overall (96%). Some argued, however, that parts of the content may have been lengthy and dense, and that there were insufficient materials tailored toward healthcare professionals, including the cultural barriers of populations they are expected to attend to and actionable ways to advocate for patients. Public health policy, leadership, and communication competencies were noticeably absent in several modules. It is recommended that modules be amended to include components that students felt were instructive. It is also suggested that a committee standardize the core curricula; local programs may then tailor them as needed.
Introduction
Not enough medical graduates choose to work in rural and medically underserved areas, especially in primary care. 1 Immersive learning experiences and tailored curricula have been shown to be important factors in encouraging students to work in these areas. 1 In the 1970s, Congress established the Area Health Education Center (AHEC) program—funded by the Health Resources and Services Administration (HRSA)—to recruit, train, and retain a healthcare workforce committed to rural and medically underserved areas. 2 Over 120 medical schools and 600 nursing and allied health schools are now partnered with 1 of the 300 AHEC programs strategically located across the US, according to the National AHEC Organization (NAO). 2 The AHEC Scholars program is for students who wish to supplement their education with knowledge and experiences specific to the needs of rural and underserved communities.2–4 It requires a 2-year commitment, consisting of 80 h of experiential activities and 80 h of didactic learning. However, little guidance was provided, resulting in each program developing its own ad hoc curriculum. It is only prudent then that the didactic curricula be evaluated to determine if the program can be redesigned to better realize the goal of a sustainable rural healthcare workforce.
Methods
The context-input-process-product (CIPP) model for curriculum evaluation was adapted to evaluate the AHEC Scholars program, as shown in Figure 1. 5 The goals and plans of the program, as represented in the context and input evaluation phases, are well established. To that end, the didactic curriculum was designed, as summarized in the process evaluation phase, around 5 core topics mandated by HRSA, comprising: behavioral health integration, cultural competency, interprofessional education, social determinants of health, and practice transformation. 6 The objective of this review lies in product evaluation: to critically assess the didactic curricula and determine whether the content addresses the core values of the AHEC Scholars program and whether the goal of developing a healthcare workforce that understands the needs of rural and underserved communities is achievable under the program as currently implemented.
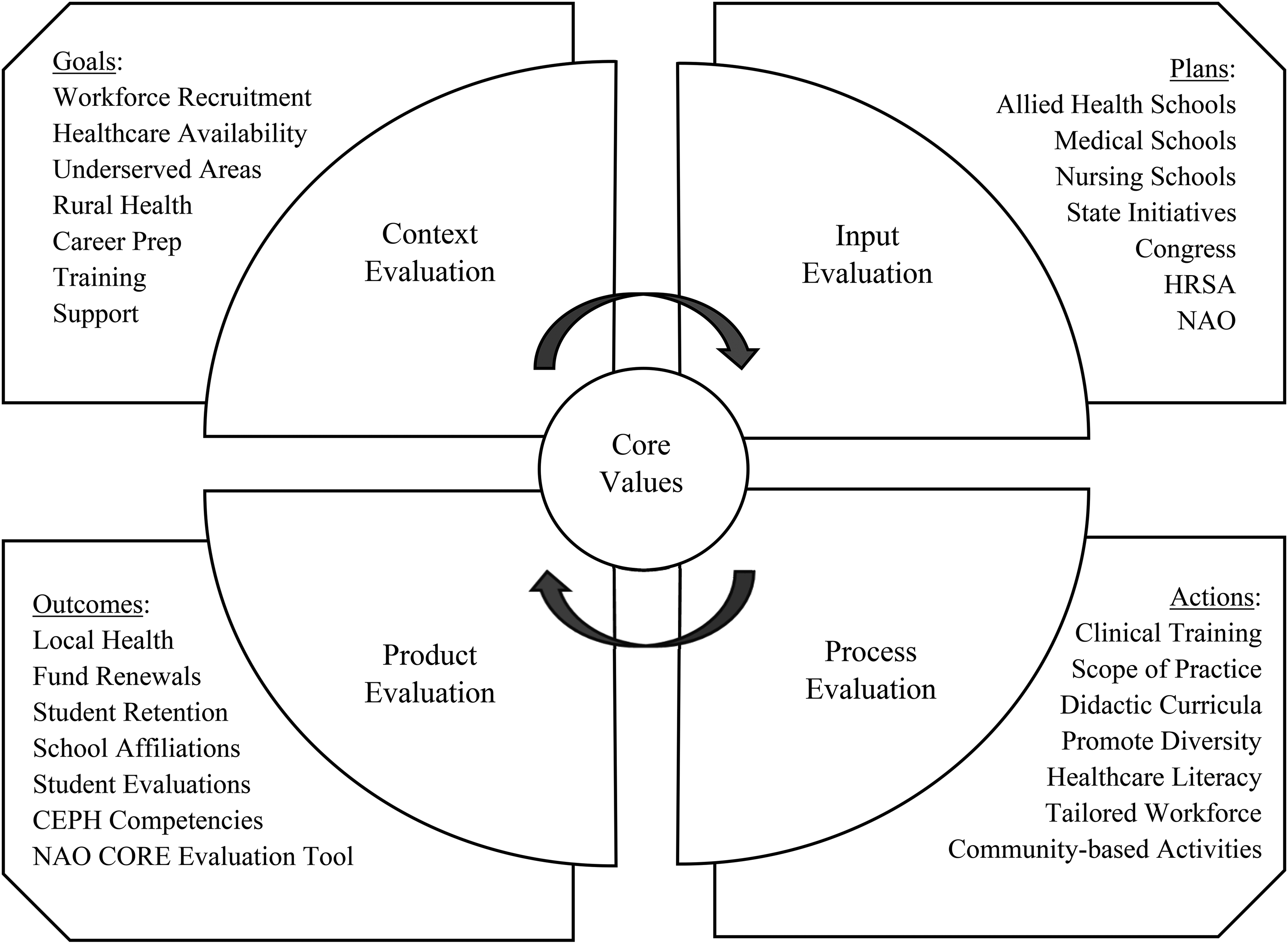
CIPP evaluation model adapted for the AHEC scholars program.
This critical review was performed independently, explored all aspects of the curricula, and examined programs from multiple states. Here, the AHEC Scholars' didactic curricula from Alabama (AL), Florida (FL), and South Carolina (SC) were evaluated using a mixed-methods approach. Each of the 5 modules from all 3 state programs was examined to assess its content and mode of delivery, and whether the 8 competency domains from the Council on Education for Public Health (CEPH) were incorporated. 6 Student evaluations for each module from the 2019–2020 cohorts in AL and SC were also analyzed; students were asked (not required) to complete these evaluations. Students in the AL cohort were asked to complete a 7-item survey to rate the following on a 5-point Likert scale: responsive facilitator, relatable to career, time appropriate, easily understandable, understanding improved, clear objectives, and overall satisfaction (Supplemental Table 1). Students in the SC cohort were asked to complete a 2-item survey to rate the usefulness and appropriateness of the content on a 5-point Likert scale (Supplemental Table 1). Neither survey was validated or pilot-tested before implementation. Both cohorts were also asked open-ended questions on what they most and least liked about each module. The proposed work was approved by the Southeast Regional AHEC Scholars Learning Collaborative.
Results
Both the AL and FL AHEC Scholars programs host their didactic curricula in Google Classroom. Each core topic is designated its own module, which is divided into approximately 6 sections. Embedded within each section are links to external content, primarily relevant articles, videos, and podcasts; students are then asked to work in teams or individually to reflect on the materials. The content is engaging; however, students may feel overwhelmed by how the modules are compartmentalized into numerous sections and the inordinate number of links to external media. Although similarly formatted, the modules and their contents do differ between the AL and FL programs. In contrast, the SC AHEC Scholars program hosts its didactic curriculum on its own restricted website 6 ; the user interface is clean and simple, but perhaps not as conducive to discussions or collaboration as Google Classroom. As with the AL and FL programs, the SC program also designates each core topic with its own module, which is usually divided into approximately 2 sections. Embedded within each section are links to external content, including relevant videos and articles; students are then asked to individually complete short quizzes comprised of matching or multiple-choice questions to check their knowledge. Although the videos and articles are lengthier than those required in the AL and FL programs, the reduced number of links to external media may be more palatable to students already overwhelmed by their degree coursework. However, it is noteworthy that there are no team activities, and not 1 student replied to or commented on another student's responses to the discussion questions, suggesting that there are components of the Google Classroom platform that may be useful here.
Behavioral health integration
Behavioral health integration, as defined by the NAO, is the development of integrated primary and behavioral health services to better address the needs of individuals with mental health and substance use conditions. 7 As shown in Table 1, the CEPH competency domains incorporated by each program in this module vary. Although it is not necessary to address all the domains in any particular module, it is notable that AL incorporates all 8 except for public health policy; whereas FL additionally excludes leadership and SC additionally excludes evidence-based approaches. As described in Table 2, most students in AL rated all 7 items very positively; only 3% to 5% of students felt either ambivalent or responded negatively. However, of all the modules evaluated, the proportion who rated strongly agree was the lowest for the following items: responsive facilitator (71%), easily understandable (61%), understanding improved (61%), clear objectives (62%), and satisfaction (60%). All students in SC rated the 2 items positively; the data are not tabulated due to small samples, and most modules had <10 respondents. Almost all students from AL and SC enjoyed the videos, but some students from AL felt overwhelmed.
Incorporation of the CEPH competency domains in the AHEC scholars' didactic curricula.

Abbreviations: AHEC, Area Health Education Center; AL, Alabama; CEPH, Council On Education For Public Health; FL, Florida; NAO, National AHEC Organization; SC, South Carolina.
NAO: Development of integrated primary and behavioral health services to better address the needs of individuals with mental health and substance use conditions.
NAO: Recognize and address the unique culture, language, and health literacy of diverse consumers and communities to improve individual health and build healthy communities.
NAO: Coordinated, patient-centered model of care that involves an understanding of the contributions of multiple healthcare professionals.
NAO: Economic stability, education, social and community context, health and healthcare, and neighborhood and built environment.
NAO: Supporting quality improvement and patient-centered care through goal-setting, leadership, practice facilitation, workflow changes, measuring outcomes, and adapting organizational tools and processes to promote new team-based models of care delivery.
Student evaluations of the Alabama AHEC scholars' didactic curriculum (2019-2020).

Abbreviations: AHEC, Area Health Education Center; NAO, National AHEC Organization.
NAO: Development of integrated primary and behavioral health services to better address the needs of individuals with mental health and substance use conditions.
NAO: Recognize and address the unique culture, language, and health literacy of diverse consumers and communities to improve individual health and build healthy communities.
NAO: Coordinated, patient-centered model of care that involves an understanding of the contributions of multiple healthcare professionals.
NAO: Economic stability, education, social and community context, health and healthcare, and neighborhood and built environment.
NAO: Supporting quality improvement and patient-centered care through goal-setting, leadership, practice facilitation, workflow changes, measuring outcomes, and adapting organizational tools and processes to promote new team-based models of care delivery.
Module adapted to incorporate pandemic-related content.
The course facilitator was responsive to my needs.
I have identified actions I will take to apply information from this course to my career.
The time necessary to complete this course was appropriate.
The information was presented in ways I could understand.
My understanding of the subject matter improved as a result of this course.
Course objectives were clearly defined.
Overall, I was satisfied with this course.
Cultural competency
Cultural competency, as defined by the NAO, is training healthcare providers to recognize and address the unique culture, language, and health literacy of diverse consumers and communities to improve individual health and build healthy communities. 7 As shown in Table 1, FL remarkably incorporates all 8 CEPH competency domains in their module; AL only omits leadership and SC only omits public health policy and planning and management. As described in Table 2, the majority of students in AL rated all 7 items very positively; only 4% to 8% of students felt either ambivalent or responded negatively. However, of all the modules evaluated, the proportion rated strongly agree was the lowest for the items, responsive facilitator (71%) and time appropriate (57%). Many students from both AL and SC enjoyed the readings, but felt that there was not enough material tailored to healthcare professionals, particularly understanding the cultural barriers of immigrants, tribal populations, minorities, the incarcerated, and the uninsured and underinsured. Furthermore, more than any of the other modules, students felt it was redundant and that the time required to complete the module was disproportionately excessive.
Interprofessional education
Interprofessional education, as defined by the NAO, is a coordinated, patient-centered model of care that involves an understanding of the contributions of multiple healthcare professionals. 7 As shown in Table 1, AL remarkably incorporates all 8 CEPH competency domains in their module; SC excludes public health policy and planning and management, whereas FL excludes evidence-based approaches, leadership, and communication. As described in Table 2, most students in AL rated all 7 items very positively; only 2% to 4% of students felt ambivalent or responded negatively. However, of all the modules evaluated, the proportion of students who rated strongly agree was the lowest for the item, clear objectives (62%). Many students from AL liked the interactive component of this module, allowing them to interact with their peers from varying professions and to discuss their thoughts; however, others felt the content was not easily accessible and it was difficult to determine their progress. Meanwhile, students in SC enjoyed the TED talks but some felt that there were not enough examples of actionable ways to make an impact.
Social determinants of health
Social determinants of health, as defined by the NAO, include economic stability, education, social and community context, health and healthcare, and neighborhood and built environment. 7 As shown in Table 1, FL incorporates all 8 CEPH competency domains except for leadership in their module; AL also omits interprofessional practice while SC also omits public health policy and planning and management. As described in Table 2, most students in AL rated all 7 items very positively; only 2% to 5% of students felt ambivalent or responded negatively. Furthermore, of all the modules evaluated, the proportion of students who rated strongly agree was the highest for the following items: responsive facilitator (78%), easily understandable (73%), clear objectives (68%), and satisfaction (68%). Most students from AL enjoyed the online poverty simulation that was included but felt both the videos and articles were lengthy and dense. While students in SC appreciated the incorporation of relevant clips from feature films.
Practice transformation
Practice transformation, as defined by the NAO, is supporting quality improvement and patient-centered care through goal-setting, leadership, practice facilitation, workflow changes, measuring outcomes, and adapting organizational tools and processes to promote new team-based models of care delivery. 7 As shown in Table 1, AL remarkably incorporates all 8 CEPH competency domains in their module; SC additionally excludes interprofessional practice and FL additionally excludes leadership. As described in Table 2, most students in AL rated all 7 items very positively; only 2% to 5% of students felt ambivalent or responded negatively. However, of all the modules evaluated, the proportion of students who rated strongly agree was the lowest for item, relatable to career (65%); but, it was the highest for the following items: time appropriate (72%), understanding improved (72%), and satisfaction (68%). Many students from AL liked that the content corresponded to what they were currently learning in their degree coursework; others felt the links to secondary source materials were unreliable. Students from SC thought that the level of content was insufficient. With the emergence of severe acute respiratory syndrome-coronavirus-2, many programs adapted to incorporate COVID-19-related content, namely the Emerging & Current Health Issues module in AL; results from student evaluations for this new module are also described in Table 2.
Discussion
This critical review represents the first formal evaluation of the AHEC Scholars' didactic curricula. Results indisputably suggest that the vast majority of students were satisfied overall, and felt that the modules were clearly outlined, easy to understand, and were not overly time-consumptive. Some students, however, sensibly argued that parts of the content may have been excessively lengthy and dense and that there were insufficient materials tailored toward healthcare professionals, including the cultural barriers of patient populations they are expected to attend to and actionable ways to advocate for a patient-centered model of care. Most modules incorporated many of the CEPH competency domains; however, public health policy, leadership, and communication were noticeably absent in several modules. 6 Strengths of this work include independent access to the complete didactic curricula from 3 states and analysis of course evaluations from a recent cohort of students. Limitations of this work include the subjectivity in determining whether CEPH competency domains were incorporated; the AL and SC course evaluation surveys were neither validated nor pilot-tested before implementation, the latter produced sparse data, both measured few outcomes, and both were susceptible to nonresponse and social desirability biases; no survey data were available from FL; and these data are largely nongeneralizable as they do not represent AHEC Scholar didactic curricula from other states.
Conclusion
It is recommended that modules be amended to include components that students felt were instructive to their learning, including links to content related to their current degree coursework or to thought-provoking online simulations, encouraging more discussions, and streamlining the course structure. It is also suggested that a committee be formed to standardize the core curricula; local programs may then supplement it with training specific to the needs of their communities. Finally, further federal and state investments are necessary since current funding levels are insufficient to meet the full scope of rural healthcare needs. 7 Strengthening the AHEC Scholars program, which already provides immersive learning experiences and tailored curricula—important factors that have been proven to encourage students to work in rural and medically underserved areas—may be the most cost-effective method to meet the burgeoning demand.1,4
Supplemental Material
sj-docx-1-mde-10.1177_23821205231175030 - Supplemental material for Review of the Area Health Education Center Scholars Didactic Curricula: A Federal Program for Students Interested in Rural Health
Supplemental material, sj-docx-1-mde-10.1177_23821205231175030 for Review of the Area Health Education Center Scholars Didactic Curricula: A Federal Program for Students Interested in Rural Health by Kartavya J Vyas in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The author would like to acknowledge the support of the Southeast Regional AHEC Scholars Learning Collaborative, particularly Anne M. Wenders of the University of South Florida AHEC program, Glenda J. Stanley of the Alabama Statewide AHEC program, and Jennifer Bailey of the South Carolina AHEC consortium. The author would also like to express his sincere appreciation for the guidance received from Dr. Julie A. Gazmararian of Emory University.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant UB6HP31680, Public Health Training Centers for $4,348,992. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.