
Abstract
OBJECTIVES
Children with physical disabilities (CWPD) have historically experienced inadequate and insensitive care across medical settings. A lack of comfort and knowledge about CWPD is prevalent among healthcare provider trainees. We developed a new, readily distributable educational resource about CWPD for healthcare students and conducted a study to determine its efficacy in improving their attitudes toward CWPD.
METHODS
We collaborated with a working group of stakeholders in the disability community to develop an educational resource for healthcare students. We developed nine short video clips (with a cumulative duration of 27 min) of a primary care visit using simulated participants and embedded them into a 50-min workshop. We conducted a study of the workshop's utility for volunteer healthcare students using synchronous videoconferencing. Participating students completed assessments at baseline and after the workshop. Our primary outcome measure was a change in the Attitudes to Disabled Persons—Original (ATDP-O) scale.
RESULTS
Forty-nine healthcare students participated in the training session: 29 (59%) from medicine, and 21 (41%) from physician assistant or nursing programs. The materials were easy to deliver virtually. The workshop resulted in measurable change in attitudes regarding physical disabilities, with improvement in ATDP-O scores between baseline (M = 31.2, SD = 8.9) and endpoint (M = 34.8, SD = 10.1) scores (t(49)= 3.28, P = .002, Cohen's d = 0.38).
CONCLUSION
This video-based educational resource on CWPD is readily distributable and can be delivered virtually as a workshop. The video-enhanced workshop improved healthcare students’ perceptions and attitudes toward CWPDs. All materials are available to view, download, or adapt by end-use instructors.
Keywords
Introduction
Over sixty million people in the United States have some form of disability, comprising 26% of the general population 1 ; those with serious physical disabilities impacting mobility represent half of the total. During 2008-2010, there were 2.9 million children with one or more disabilities, or 4% of all U.S. children under the age of 18. 2 Despite such high prevalence, patients with physical disabilities have historically experienced inadequate and insensitive care from physicians across medical settings, including primary care.3,4 Surveys of adult patients with disabilities have shown many are less likely to be asked about health promotion, including functional assessments, inquiries about emotional status, or screening for physical or sexual violence.5,6 Similar disparities in quality of primary care exist for children with physical disabilities (CWPD), particularly in the areas of screening, prevention, and chronic illness management. 7 There have been improvements in the primary care of CWPD using a family-centered care model, 8 but many areas of dissatisfaction persist.
Primary care physicians have demonstrated widely varying levels of comfort in treating CWPDs and report a lack of knowledge and skill as contributing factors.9,10 In turn, patients with disabilities and their families have attributed difficult healthcare experiences to providers’ unfamiliarity with their unique clinical needs.11,12 A similar lack of comfort and knowledge about patients with disabilities prevails among trainees across healthcare fields, including medical students.13,14 Female gender and direct personal experience have been shown to predict increased comfort with disability among medical students. 15 Direct clinical exposure to patients with disabilities is a modifiable factor in education that can ameliorate fear and increase positive attitudes toward improving the quality of care for this segment of the population. 16
In 2005, the Surgeon General of the United States issued a call for improved care for people with disabilities, including the development of medical school curricula to teach clinicians about best practices. 17 In response, some medical schools and residency programs have developed targeted curricula focusing on treating patients with disabilities. One noteworthy yet resource-intensive approach consists of a multi-year curriculum that incorporates clinical training and simulations. 18 Others have found that even a 30-min lecture and patient panel can increase medical student knowledge and comfort levels. 19 As recently as 2016, a Task Force on Disability Education of Medical Students was formed to provide recommendations to address the problem of insufficient medical education on the treatment of the patient with disabilities. 20
Despite these efforts, most medical school curricula still lack educational content focused on CWPD. To address this gap, we sought to (1) develop a new educational resource for healthcare students focused on CWPD that incorporates embedded videos featuring simulated participants (SPs), (2) ensure our new educational resource would be distributable to and adaptable by end-use instructors, and (3) evaluate the effect of the resource on healthcare student attitudes toward and perceptions of CWPD.
Methods
We conducted a prospective research study with the goal of evaluating a video-enriched educational resource we created. Specifically, we evaluated whether such a resource improved learners’ perceptions and attitudes about CWPD. We conducted the study using synchronized videoconferencing in the fall of 2021. Lead investigators and data collection and analysis were based at Yale School of Medicine, in New Haven, Connecticut.
Development of the educational resource
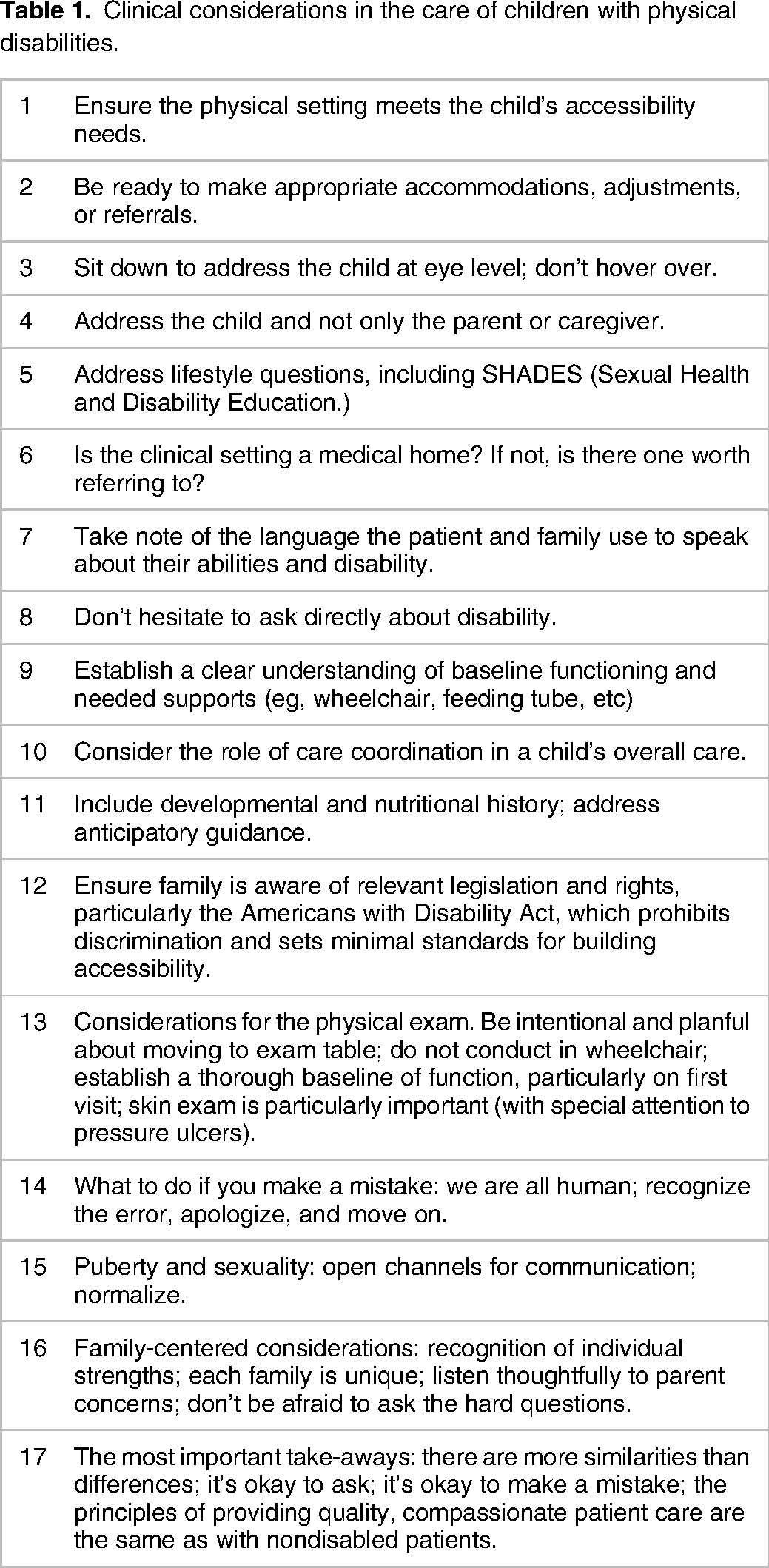
In keeping with the tenets of participatory action research (PAR) 21 and the notion of “nothing about me without me,” 22 we designed the curriculum in conjunction with a working group of multiple stakeholders in the disability community. In PAR, it is those stakeholders and community members informing the study who are its most likely beneficiaries. The group was formed by direct recruitment of members of the disability community and consisted of nine members, including six women and three men varying in age from young adult to middle age. The members came from a variety of backgrounds related to the care of patients with disabilities, including lived experience and professional expertise. Members included directors of regional disability advocacy organizations, multiple adult wheelchair users, and parents of CWPD, as well as faculty with complementary expertise in caring for CWPD, clinical skills education, and curriculum design using SPs. We conducted individual interviews with each member of the curriculum working group, asking questions such as “What do you think medical students should know about taking care of patients with disabilities?” We took extensive notes during the interviews and used them to identify important themes and learning points that could then be demonstrated in the videos or serve as topics for discussion. The key points identified are listed in Table 1 and were highlighted throughout the videos and workshop materials.
Clinical considerations in the care of children with physical disabilities.
The educational resource includes video clips that depict a detailed, model primary care visit conducted by one of the coauthors (EN), a pediatrician experienced in treating CWPD. We chose a primary care setting as it provides an opportunity to demonstrate proper screening and prevention behaviors in the outpatient setting, as provision of care in these areas of care is often lacking for patients with disabilities.
The patient and parent in the video depictions are hired professional actors familiar with working in medical settings. We followed accepted best practices for SPs, 23 taking particular care to abide by the additional practical, legal, and ethical considerations for working with underage actors. 24 The actors were recruited from a local community acting group.
The video-based component consists of nine clips, ranging from 50 s to 5 min in length, for a cumulative duration of 27 min. We also created an additional video clip featuring an interview with a disability advocate and one of the coauthors, who uses a wheelchair. The different components and their respective lengths are described in Table 2. A slide deck contains suggestions of important points to highlight and discussion questions in the “Notes” section of each corresponding slide. A facilitator guide provides variations to conduct the session. Both the slide deck and the facilitator guide can be accessed as Supplemental materials through this link: https://doi.org/10.6084/m9.figshare.13635107.v2.
Video clip guide for child with physical disability educational resource.

Study design and participants
Participants were healthcare students enrolled in the Yale School of Medicine, Yale School of Nursing, and the Yale Physician Associate online program. We recruited volunteer learners via emails sent to members of relevant medical student interest groups, as well as to the students in the nursing school and online physician assistant programs. We had no additional inclusion or exclusion criteria.
Participation was voluntary, responses were anonymous, and individual survey results were not accessible to faculty responsible for any course evaluations. Before joining the educational session, which was an optional enrichment activity, participants provided written informed consent electronically. We did not collect personally identifying information that could compromise anonymity. The study was approved by the Yale School of Medicine Human Investigations Committee (Protocol # 2000028161).
Measures
Participants completed the Disability Attitudes in Health Care (DAHS) 25 at baseline to ensure our sample was consistent with published norms for healthcare students. The DAHS is a 17-item instrument used to measure baseline attitudes unrelated to curricular content and has good internal consistency (Cronbach α = .74).
Participants also completed the Attitudes to Disabled Persons—Original (ATDP-O) 26 scale at baseline and endpoint to assess change in attitudes following the workshop. The ATDP-O is a widely used instrument shown to have good internal consistency (Cronbach α = 0.91) and sensitivity to change. The ATDP-O has 20 items, for which respondents indicate how strongly they agree or disagree with statements about individuals with disabilities; some of the items are reverse-coded to prevent response acquiescence bias.
Finally, we asked learners to provide the first three words or short phrases “that come to mind when hearing ‘child on a wheelchair.'”
Data collection and statistical analysis
We conducted the workshop during the COVID-19 pandemic, delivering content virtually through the video-conferencing platform Zoom (San Jose, CA). Participating students were given 10 min before and after the workshop to complete the study surveys. Responses were collected securely using Qualtrics (Provo, UT). We analyzed data using SPSS Version 25 (Armonk, NY). We calculated the mean score and standard deviation for each item of the ATDP-O. We then compared the ATDP-O composite change score using a paired t-test and Cohen's d for effect size. We used word cloud generator software (wordclouds.com; Zygomatic Inc., Vianen, the Netherlands) to visually depict participants’ word choices before and after the workshop. We manually coded the words into three emotional valence categories.27,28 Word clouds are commonly used in education research, as they can complement activities by visualizing underlying themes identified by learners. 29
Results
Forty-nine healthcare students completed the survey: 29 (59%) from medicine, and 21 (41%) from physician assistant or nursing programs. Twenty-nine participants (59%) had been previously involved in the care of a CWPD; 23 (47%) had a friend or relative who is a CWPD or a parent of a CWPD; and 5 (10%) reported a physical disability themselves.
Baseline scores on the DAHS did not differ from published norms: M = 67.2, SD = 3.9 versus M = 66.5 (single sample t = 1.25, ns). ATDP-O scores improved between baseline (M = 31.2, SD = 8.9) and endpoint (M = 34.8, SD = 10.1), with a mean difference = 3.6 [95% confidence interval = 1.4-5.8]. The paired t-test of baseline and endpoint showed a significant change (t(49)= 3.28, P = .002, Cohen's d = .38). Table 3 summarizes item-level scores before and after the intervention.
Change on the attitudes to disabled persons original (ATDP-O) scale 26 after workshop (n = 49).

Note: Higher values indicate more positive/less stigmatized attitudes; asterisks (*) denote reverse scoring.
Figure 1 provides a visual rendering of all words written by learners before and after the workshop. Words are weighted by frequency and highlighted in colors, each of three representing a different emotional valence: red, negative; blue, positive; white, neutral.

Word clouds based on the prompt “provide the first three words or short phrases that come to mind when hearing ‘child on a wheelchair’.” Panel A: before didactic intervention; Panel B: after. n = 147 words for each panel; words with four or more occurrences: four with negative valence in panel A (challenging, disability, different, difficult); nine with positive valence in panel B (able, accommodations, compassion, empathy, normal, person, resilient, strong, support), and two with neutral valence (denoted in white: accessibly, mobility) across panels.
Discussion
We developed, through collaboration with multiple stakeholders in the disability community, a novel video-enriched curriculum for healthcare students on the treatment of CWPD. Our curriculum can be delivered virtually and improved students' attitudes about caring for CWPD.
Participation in the virtual workshop resulted in healthcare students’ positive shifts in attitudes. The improvement was statistically significant, with a medium effect size of 0.38. Students also exhibited a shift in views, moving from approaching CWPDs as “different” and “challenging” to seeing them as “normal” and “resilient,” indicating a reduction in stigmatized views. Learners gained a sense that the interpersonal approach to patients with physical disabilities need not differ greatly. Indeed, such an insight is by design at the crux of the workshop; namely, that the treatment of patients with disabilities should at its core be interpersonally the same as that for able-bodied patients, while recognizing and maintaining respect for inherent differences. This message was felt by the members of our curriculum working group, who considered this “normalizing” as perhaps the most important lesson to impart to healthcare students. At the same time, they identified considerations unique to the care of CWPD, compiled as key points which we highlighted in the workshop and include in the supplementary teaching materials.
Our materials focus on the experience of a single child who uses a wheelchair during an outpatient clinic visit. Even as this workshop enhanced healthcare students’ attitudes toward CWPD, we consider this a first step in the development of a curriculum that properly prepares students to provide quality, compassionate care for patients with all forms of disabilities. Our work is aligned with the transformative potential of “disability-conscious medical education, training, and practice,” 30 which draws on insights from intersectional disability justice activism. However, we do not address the many other forms of disability, including cognitive or emotional. A natural next step will be to develop additional curated materials that focus on the treatment of patients with cognitive or emotional disabilities, as well as those with concurrent physical and cognitive disabilities. We recognize the disability community is broad and varied, and that the materials developed for this study represent only a start at improving medical education efforts designed to increase the quality and sensitivity of healthcare delivered to patients with physical disabilities. We intend to develop materials that address other types of disability, particularly combined physical and cognitive.
We recognize the importance of direct student exposure to, and engagement with patients with disabilities, given that “only when healthcare providers, educators, and students are routinely and meaningfully exposed to the perspectives of people with disabilities can they develop a consistent proficiency in diagnosing and treating ableism, in their profession generally, as well as in their own practice.” 31 After the didactic and collection of endpoint measures, we had an additional, 30-min, unstructured discussion with a panel of individuals with living experience with physical disability: two adults on wheelchairs and the parents of a child with physical disabilities. Since our goal was to evaluate the new didactic materials, we excluded the panel component from our pre/post-outcome measures. However, we encourage incorporating, whenever possible, a patient and/or parent panel as a synergistic complement to the videotaped materials embedded in the workshop. For situations in which access to suitable volunteer panelists or disability advocates is not feasible, instructors can use the filmed discussion about one of the co-author's experiences navigating the healthcare system as a person who uses a wheelchair. This 9-min video addendum is available as part of the supplementary online materials.
The video clips present multiple springboards for rich discussion, including aspects of the model visit that do not completely reflect best practices. One such point is how the guardrail on the side of the patient's bed was not raised during the physical exam to maximize patient safety. Another is that while the physician in the video is a model for interacting with a child with a physical disability, even as an expert there were instances in which she assumed the patient would be unable to perform a task before asking, such as during discussion of transfer to the exam table, when the physician asked how best to assist before confirming if any assistance was in fact needed.
This initial study represents the first step in establishing the effectiveness of our curriculum. To assess the long-term effects and clinical implications of our curriculum, we intend to expand our efforts and reach all students by incorporating the workshop into our programs’ routine clinical rotation in pediatrics. As the workshop becomes formally integrated into the medical school curriculum, we will be able to measure the sustainability of effects, and ultimately behavioral change.
Limitations
We recognize several limitations. First, participating students voluntarily attended the workshop outside of classroom time and may represent a biased sample. Students with greater interest in the subject matter might have been more likely to attend, have more knowledge and less stigmatized views at baseline, and report higher satisfaction. However, despite this likely bias in sampling, we documented short-term improvements in attitudes after participation in the workshop.
Second, we acknowledge that one of our two professional actors was an able-bodied child, a shortcoming we made explicit at the end of the workshop (and in the addendum interview). We were not able to recruit a CWPD to serve as an SP, but are committed to doing so in future iterations, following guidelines for “authentic representation” set forth in an influential white paper advocating for the employment in television of actors with disabilities. 32
Third, we filmed the workshop during the COVID-19 pandemic. To ensure safety, all participants wore face masks. Masks veiled facial expressions and constrained nonverbal communication. At the same time, they provided a “time stamp” to the pandemic years during which these enduring materials were produced.
Fourth, we measured outcomes upon completion of the workshop, alerting to immediate recall bias and results that may or may not have lasting effects. Fifth, we did not include a qualitative component of the participants’ or panelists’ views, which would have been complementary toward a mixed methods design. Fifth, we did not use power analysis to prospectively calculate a suitable sample size. Finally, we did not include a control group, which could have helped determine the unique pedagogic contribution of the video component.
Conclusion
CWPDs have historically experienced inadequate and insensitive health care and many students in the health professions feel lacking of comfort with treating this important segment of the population. We sought to improve a gap in medical education by developing a video-enriched educational resource focused on the treatment of CWPDs. In our preliminary study, the workshop was easily delivered virtually and results in a change in healthcare students’ attitudes toward CWPD. To ensure the educational resource is readily distributable and adaptable for end-use instructors, we have made all didactic materials available to view or download for free. We next plan to integrate this workshop into the routine clinical curriculum in pediatrics at our institution, continue to develop additional materials on other forms of disability, and to incorporate patients’ and families’ perspectives.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
This study was supported by the Riva Ariella Ritvo Endowment at the Yale School of Medicine and by grant R25 MH077823 (Research Education for Future Physician-Scientists in Child Psychiatry) from the National Institute of Mental Health.