
Abstract
Background
Graduate medical education programs lack enough faculty trained in quality improvement (QI). A major barrier to increasing the number of faculty competent in QI is insufficient time to engage in training. Research is missing on the effectiveness of short faculty development workshops to teach academic faculty QI principles and promote participation and mentorship in QI projects.
Objective
The authors assessed the ability of a four-hour experiential QI workshop to increase faculty proficiency in QI principles, enhance faculty involvement in QI, and improve resident mentorship in QI.
Methods
From 2016 to 2017, the authors conducted seven QI faculty development workshops at a large academic medical center with 12 ACGME training programs. We evaluated the workshop using pre- and post-workshop surveys, as well as six- and twelve-month follow up surveys.
Results
Sixty-five faculty participated in seven workshops over 13 months. All participants completed pre- and post-workshop surveys, while 38% (n = 25) responded to the six- and twelve-month follow up surveys. Overall, the workshop significantly increased confidence to lead and mentor residents on a QI project (25% pre vs. 72% post, p < .001), increased ability to teach QI (8% pre vs. 36% post, p < .001), increased participation in planning and decision making on a QI team (32% pre vs. 50% post, p = .002), and increased the mean number of QI projects implemented (.45 pre vs. 1.24 post; p < .05).
Conclusion
A four-hour QI workshop is a quick and effective training method to develop academic faculty to teach and mentor residents in QI. The principles taught increased perceived knowledge, confidence in mentorship, and participation in QI.
Introduction
Teaching quality improvement (QI) in medical residency is now an essential part of graduate medical education (GME). GME programs are required to incorporate resident participation in QI processes and these programs are assessed based on resident involvement in QI initiatives.1,2 The Accreditation Council for Graduate Medical Education (ACGME) is focused on ensuring that residents are meaningfully involved in improving the quality of care in institutions that sponsor GME. Subsequently, GME programs must develop QI curricula to meet these requirements.
Faculty involvement will be critical for both having a successful QI curriculum and promoting resident participation in QI initiatives.3,4 This expectation that academic faculty develop proficiency in quality improvement drives a demand for faculty who are able to teach and mentor medical residents in QI projects. 5 However, GME programs often lack senior faculty whose careers have focused on quality improvement and many faculty have not had the necessary training to grow their competency in quality improvement concepts.6–11 As a result, academic departments have a shortage of faculty with the experience or knowledge to instruct and mentor medical residents in quality improvement initiatives.4,5,8,9
One strategy to raise a critical mass of trained faculty is to provide faculty development programs that introduce QI concepts and offer a framework for faculty to mentor residents in developing QI projects. 5 However, a major barrier to faculty involvement is a lack of time to engage in training.11–14 While research demonstrates that faculty development programs in quality improvement are effective, most require a considerable commitment from faculty to complete.13–20 Research is lacking on the effectiveness of shorter and less time consuming workshops to teach academic faculty in QI principles and promote participation in QI projects. Such short interventions may provide an avenue to quickly train large numbers of academic faculty to meet the demands of GME QI curricula. To test this hypothesis, we set out to answer the following research question: Can a four-hour workshop increase faculty proficiency in QI principles, increase faculty involvement in QI projects, and increase resident mentorship in QI?
Methods
Setting and Participants
Between July 2016 and May 2017, we conducted multiple rounds of a Quality Improvement Faculty Development Workshop (QIFDW) at an academic medical center that hosts 12 ACGME accredited programs. These programs train approximately 225 residents and fellows annually. Workshops were targeted to full-time academic faculty associated with each ACGME program, but due to interest from faculty at other graduate health professions education (HPE) programs within the hospital, we did not limit our workshop to only ACGME faculty. While we acknowledge that QI projects ought to be conducted in an interprofessional manner, our goal for this project was to increase faculty proficiency, involvement, and mentorship in QI. As such, we limited the participants to teaching faculty and advertised the QIFDW through the office of the director of graduate medical education.
Intervention
We developed the QIFDW as one four-hour interactive workshop and maintained a group setting of less than 10 participants. Each workshop consisted of six sessions and each session ranged in length from 30 to 45 minutes. We created workshop materials (lecture slides and a worksheet) based on the Institute for Healthcare Improvement (IHI) QI open school curriculum (Table 1). 21 The authors teaching the workshop (MP and JB) completed the online IHI open school quality improvement course to familiarize themselves with the teaching material. The cost to implement the workshop was limited to the monetary cost of printing the worksheets and the time cost to the participants.
Overview of the quality improvement faculty development workshop.
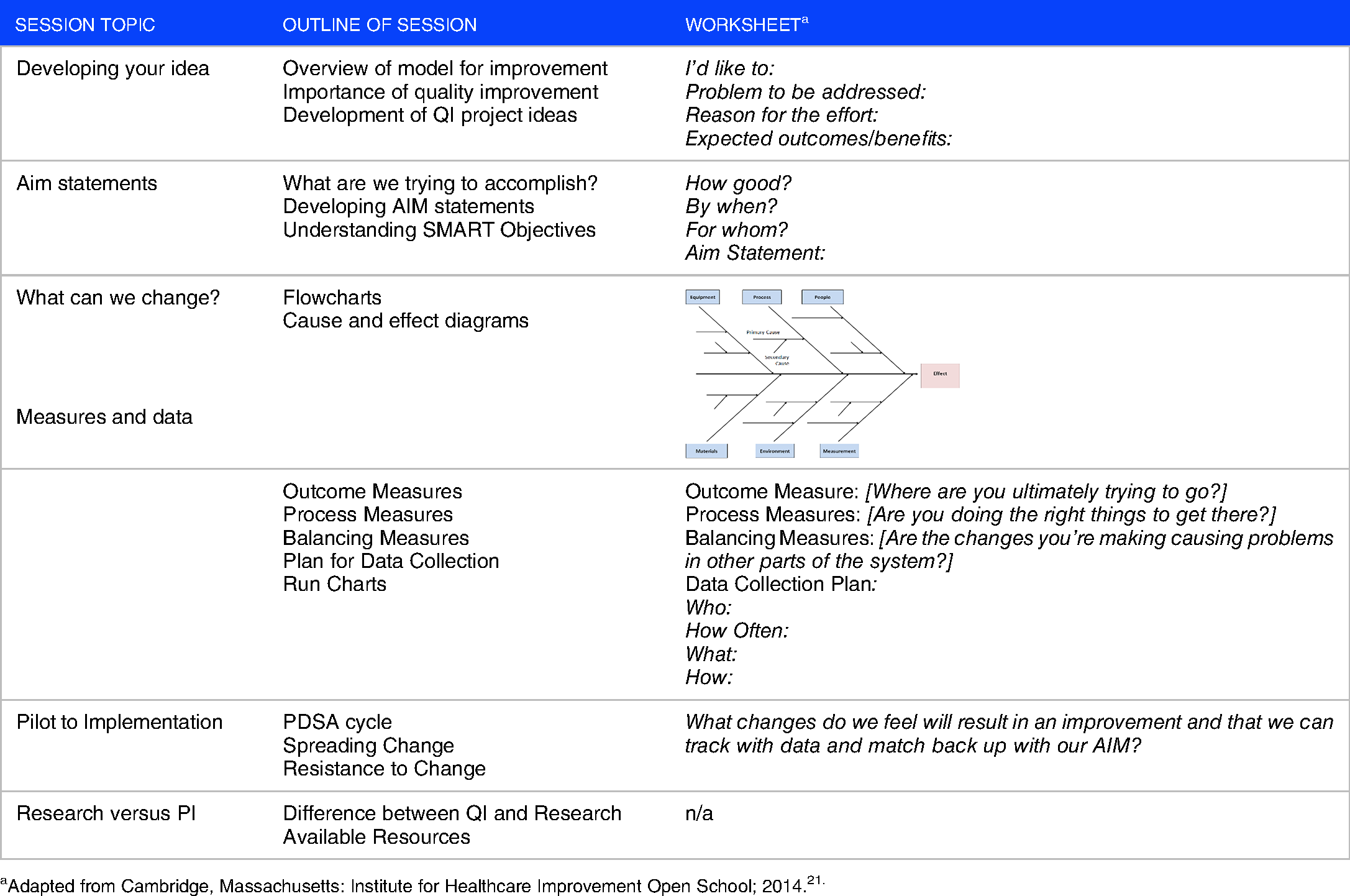
Adapted from Cambridge, Massachusetts: Institute for Healthcare Improvement Open School; 2014.21.
We designed the first four sessions of our workshop by adhering to assumptions of experiential learning theory outlined by the Association for Medical Education in Europe (AMEE) guide on experiential learning. 22 These assumptions state that learning is situated, that interactions are fundamental to learning, and that learning is triggered by authentic practice-based experiences. We therefore encouraged participants to develop a quality improvement idea that was situated within their own personal experiences; and we created frequent opportunities for peer feedback and discussion as learners shared their work in each session. To facilitate the learning process, each of the first four sessions were based on the following format: a short lecture introducing the session concepts; completion of an individual worksheet (Supplement 1) to assist the participants in implementing those concepts into their own idea; 5–10 minutes during each session for self-reflection; and then 10–15 minutes for input and feedback from other workshop participants. We also modeled the interprofessional team dynamics of the process flow chart and cause and effect diagram by using one of the participant's ideas and involving all the participants to critically assess the systems that impact that project. By the end of the initial four sessions, participants had developed an aim statement, completed a critical systems analysis (utilizing a flow chart or cause and effect diagram), identified an outcome measure and several process measures, and considered a data collection plan for their own QI project.
The final two QIFDW sessions were didactic lectures on leading organizational change and describing differences between quality improvement and research. We used a personal example of a successful QI project to highlight the 8-step process for leading change described by Kotter. 23 We also invited a representative from the Department of Clinical Investigation to explain the institutional process for determining if a project is considered research or quality improvement. Lastly, we introduced personnel from within the hospital to facilitate awareness of organizational resources available to assist faculty and residents with their QI projects. These individuals included the Chief of Quality and Safety, the hospital's Performance Improvement Coordinator, representatives from Quality Services Division and Patient Safety, a representative from Information Technology Support, and a statistician. Supplement 2 contains to content of the didactic presentations.
Outcomes
Using Kirkpatrick's program evaluation framework, 24 we developed survey questions (Supplement 3) to assess participants’ reaction to the workshop, acquisition of perceived knowledge, and changes in practice (mentoring or involvement in QI). We distributed the surveys prior to the workshop, directly after the workshop, and at six- and twelve-month intervals after the workshop. We did not collect validity evidence for our survey questions.
The survey included items rated on a 5-point Likert scale and evaluated self-perceived knowledge of QI terminology and concepts, experience in QI projects, and confidence in ability to lead and mentor QI. Open-ended questions evaluated frequency of involvement in planning QI projects, frequency of mentoring QI, outcomes of QI involvement (publications or conference presentations), barriers to implementation, and top three takeaways from the workshop. The six- and twelve-month surveys mirrored the pre-workshop survey questions to facilitate comparison of participants’ knowledge, experience, mentorship, and participation in quality improvement pre- and post- workshop.
Analysis
Chi-square tests, Fisher's exact tests, and Wilcoxon rank sum tests were used to assess changes in survey responses over time. All analyses were conducted using SAS statistical software version 9.4 (SAS Institute, Cary, NC). This study protocol was reviewed by the Tripler Army Medical Center (TAMC) Institutional Review Board and assigned TAMC Protocol Number 16S22.
Results
We conducted seven Quality Improvement Faculty Development Workshops over a 13 month period. Sixty-five academic faculty attended, representing 10 ACGME accredited residencies and 3 graduate HPE programs (Table 2). All 65 participants completed a pre- and post-workshop survey. Twenty-five participants completed the six- and twelve-month follow up surveys (38.5% response rate).
Baseline characteristics of participating academic faculty (n = 65).

Includes Otolaryngology (n = 5), Urology (n = 4), General Surgery (n = 3), Vascular (n = 2), and Orthopedics (n = 1).
Includes Clinical Registered Nurse Anesthetics (n = 2 [3.1%]), Pharmacology (n = 10 [15.4%]).
Unknown (n = 3 [4.6%]).
The post workshop and follow up surveys demonstrated that participants reacted positively to the training and had an increase in their perceived knowledge of quality improvement (Figure 1). Prior to the workshop, 38% (n = 25/65) of participants reported knowing nothing or very little about quality improvement. Six months afterwards, 92.0% (n = 23/25; p = .005) of survey respondents stated understanding the terminology and concepts. In addition, while only 8% (n = 5/65) of participants felt that they could teach quality improvement to residents before the workshop, 36% (n = 9/25) of survey respondents felt they could at both six and 12 months after the workshop (p < .001, for post compared to pre).
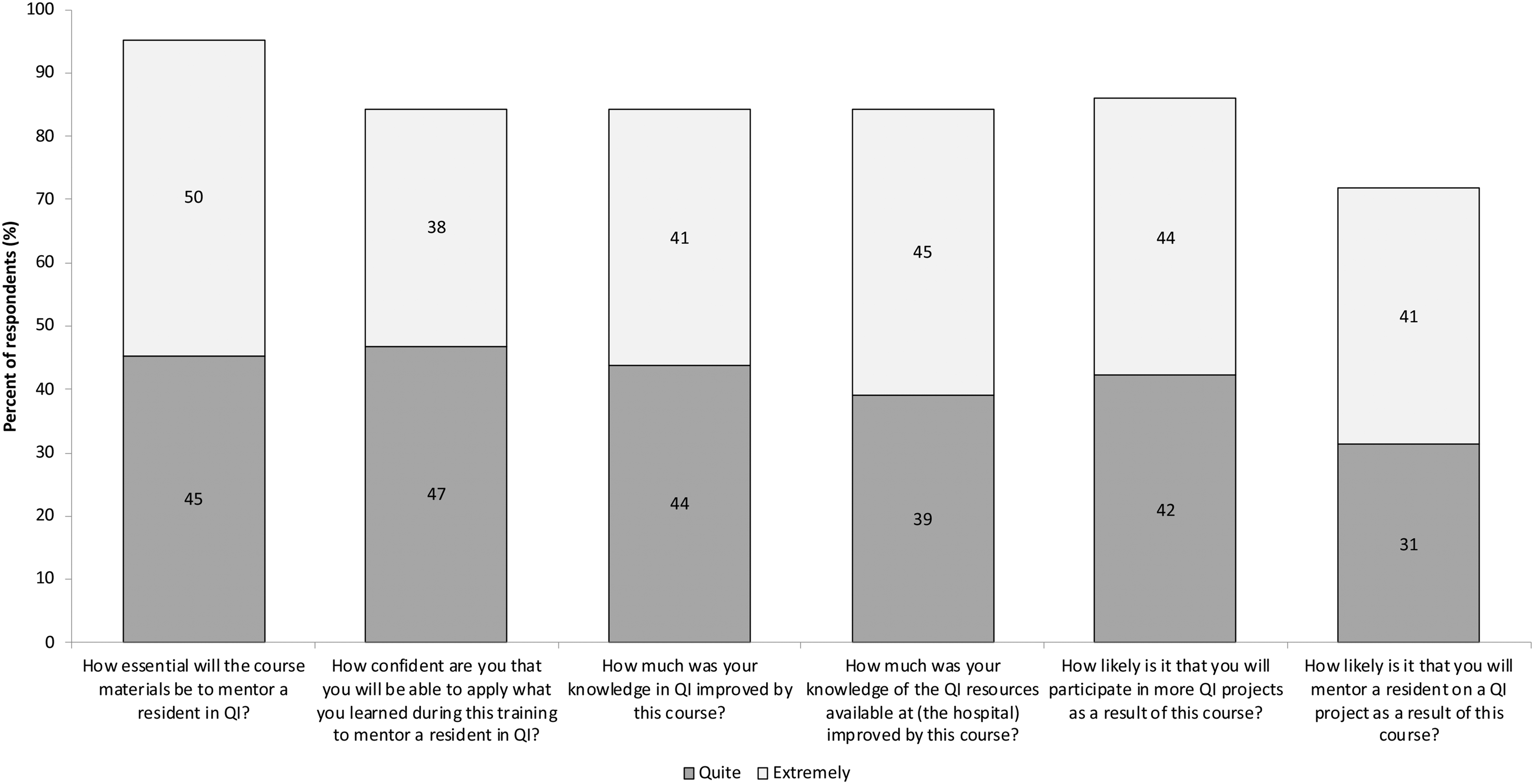
Percentage of participants who found the faculty development quality improvement workshop beneficial.
The participants also reported evidence of increased involvement in QI. Active participation in planning and decision making on a QI team increased from 46% (n = 30/65) in the 12 months prior to the workshop to 83% (n = 20/24) at six months after the workshop (p = .002). In addition, confidence in the ability to lead a QI project nearly tripled following the workshop (p < .001) (Figure 2).
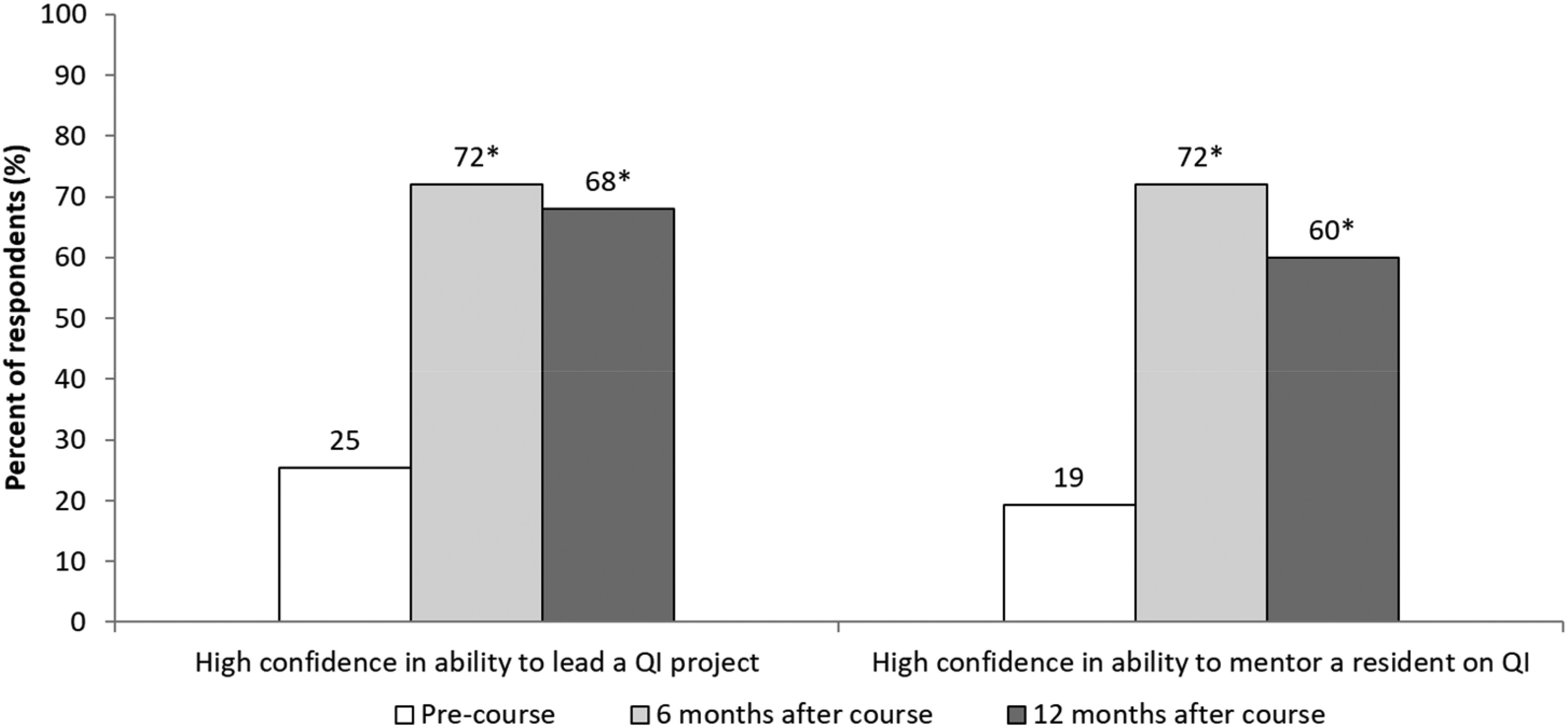
Faculty confidence to lead or mentor before and after attending the quality improvement faculty development workshop. *denotes p < .001 for comparison to pre-workshop.
The QIFDW also affected participants’ confidence and involvement in mentoring residents on QI projects (Figures 2 and 3). During the 12 months prior to the QIFDW, 32% (n = 20/62) of participants had mentored a resident in planning and developing at least one QI project. In the 6 and 12 months following the workshop, this increased to 46% (n = 11/24, p = .317) and 50.0% (n = 11/22, p = .198) respectively; while the mean number of QI projects participants implemented nearly tripled 12 months after the workshop (.45 vs. 1.24; p < .05) (Figure 3).

Faculty involvement and mentorship in quality improvement projects before and after attending the quality improvement faculty development workshop. *denotes p < .05 for comparison to 12 months before workshop.
Discussion
We developed an innovative four-hour experiential QI workshop aimed at increasing faculty proficiency in QI principles, increasing faculty involvement in QI projects, and increasing mentorship in QI. The findings of this study demonstrate that such a workshop can significantly increase faculty confidence in both leading quality improvement initiatives as well as mentoring residents through a QI project. By focusing the workshop on the experiential learning process of developing a QI project, participating faculty increased their involvement in planning, developing, and implementing QI projects over the 6 to 12 months following the QIFDW. These outcomes are comparable to those of longer faculty development training programs13,18,20 while mindful of the time commitment barrier GME programs need to overcome for faculty participation in QI training.
Many faculty development programs span in length from a few days to over a year,15–17,19,20 making faculty participation difficult. In addition, there is both a monetary cost of having faculty away from clinical care and an educational cost to having faculty away from teaching duties. Offering a condensed workshop provides a flexible format that accommodates busy clinical and teaching schedules; and often our workshop fit into pre-scheduled and dedicated residency didactic time. While we provided the workshop seven times over the thirteen months of our study, increasing the frequency of the workshops could quickly train a larger cohort of academic faculty to meet the needs of GME programs.
Many QI training programs combine didactic instruction with experiential learning 18 and we attribute the increase in participation of QI projects in our study to the experiential aspect of our workshop. By designing four of our sessions around a quality improvement idea related to each participant's own experience, participants left the workshop with a QI plan that they could take back to their academic program to enact. Since many of the faculty were also responsible to mentor residents, having this plan may have contributed to the increase in the number of QI projects implemented with their residents. In fact, one of our participants helped plan, develop, and mentor their residents in an OBGYN infection control QI project that resulted in a statistically significant decrease in rates of chorioamnionitis and significant cost savings to the hospital. 25 Very few prior studies have assessed the impact of QI training on mentoring residents. 16
We acknowledge several limitations to our study. During our data collection, we did not link the pre-survey and post-surveys and therefore were unable to follow individual participant data. Such data may have provided a richer interpretation of our results. In addition, we relied on self-reporting of knowledge retention instead of using a validated knowledge assessment (such as the QIKAT 26 ), which would provide a better marker for knowledge acquisition of QI concepts. Our survey data was also susceptible to recall bias. Including a question for participants to provide the aim of the QI project they implemented may have mitigated some of this bias by forcing participants to provide specifics on each project. This also would have allowed us to better evaluate retention of learning principles taught during the workshop and to assess the actual improvement changes from these projects. Finally, quality improvement initiatives have better clinical outcomes when performed with interprofessional teams. 27 Our workshop lacks involvement from key stakeholders and other professional disciplines.
GME programs can adapt this workshop to teach residents how to develop a QI project or to create a co-learning environment between faculty and residents. Future research efforts should explore the impact of teaching this workshop either directly to residents, to both faculty and residents, and/or within an interprofessional environment.
Conclusion
The development of faculty with the required expertise to teach and mentor residents in quality improvement will be crucial to the success of QI curricula within ACGME accredited residency programs. Implementing short faculty development workshops could effectively address the challenge of a lack of time to engage in QI training and build a cohort of academic faculty trained in QI principles, involved in QI projects, and mentoring QI to residents.
Footnotes
Acknowledgements
The authors would like to thank the members of the Tripler Army Medical Center Quality team for their introductions to our learners, their support and assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Army, Tripler Army Medical Center, Uniformed Services University of the Health Sciences, Department of Defense, or the U.S. government.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.