
Abstract
As robotic surgery has become more widespread, early exposure to the robotic platform is becoming increasingly important, not only to graduate medical education, but also for medical students pursuing surgical residency. In an effort to orient students to robotic technology and decrease the learning curve for what is likely to become an integral part of residency training, we created a formal, elective robotic surgery curriculum for senior medical students. Throughout this 2-week fourth year rotation, students completed online training modules and assessment; mastered exercises on the simulator system related to the console, camera, energy, dexterity, and suturing skills; attended didactics; utilized the dual console during one-on-one simulation lab sessions with attending robotic surgery experts; and translated new skills to biotissue anastomoses as well as bedside-assisting in the operating room. During cases, students were able to have more meaningful observation experiences, recognizing the significance of various robotic approaches employed and utilization of specific instruments. Future aims of this rotation will assess student experience as it impacts readiness for surgical residency.
Background
Although varying widely, utilization of robotic surgical approaches continues to expand in numerous areas of surgery including gynecology, urology, and general surgery, along with its multitude of subspecialties. 1 Given this growth, robotic education is becoming increasingly important for training the next generation of surgeons. However, more than half of general surgery residents report not receiving any formal robotic surgery training prior to their first robotic-assisted surgical case. 2 Implementation of robotic surgery training and experience in surgical residencies remains highly variable, although resident experience with the robot continues to become more integrated into graduate medical education training. 3 The importance of robotic surgery in surgical residency is highlighted by the importance fellowship program directors are now putting on robotic experience as they evaluate fellowship applicants 4 and in the recent construct validations for programming related to fundamental skills of robotic surgery that surgical educators are currently undertaking.5,6 Because of the current emphasis on robotic surgery at the graduate medical education level, interest in undergraduate medical education exposure to robotic surgery technology has been recently highlighted and suggested as an avenue for preparing students for surgical residency and potential early exposure to robotic surgery. 7
In an effort to prepare medical students applying for surgical residency, intern year “bootcamps” are popular as senior medical student electives prior to graduation and matriculation into a surgical residency. Most of these experiences hinge on refreshing students’ knowledge of anatomy, simulation experiences, and focusing on surgical skills such as knot tying, suturing, and even laparoscopy. However, none of these senior medical student experiences described focuses on exposure to robotic surgery or robotic surgery simulation. The only reported involvement of students in robotic surgery includes a 1-time 40-minute training session for medical students in the United Kingdom 8 and a randomized trial assessing skill retention of medical students performing laparoscopic- and robot-based tasks. 9
At our institution, we have developed the first formal elective rotation and curriculum designed for training medical students in robotic surgery with the intention of orienting students to the robotic platform technology, enhancing understanding of application of robotics in surgical subspecialties, and preparing students for resident-level training in minimally invasive and robotic surgery. This 2-week curriculum we describe herein (summarized in Table 1) includes robotic simulator curriculum, inanimate/biotissue curriculum, practical robotic surgery experience in the operating room, as well as robotic training modules and didactics. Our simulation center houses a robotic training room with 24/7 swipe card access that has a dual console robot and patient cart as well as another robotic console with a virtual reality simulator dedicated to training, which facilitates student access and timely completion of the curriculum.
Two-week robotic surgery elective curriculum summary. Note that when individual students were not working on the console in the simulation lab or in didactic sessions, they were in our hospital operating rooms assisting with and engaging in robotic-assisted cases.

Robotic Training Modules and Didactics
Prior to starting the course, all enrollees were required to complete an online assessment for surgeons, residents, and fellows on the robotic surgical system as a means of formally orienting them to the robotic platform. Hands-on didactic lectures were held for students on topics including introduction to patient cart, introduction to console and simulator, robotic instruments, robotic safety, rationale and indications for various robotic-assisted procedures, and a workshop introducing the single port robotic technology. Finally, to conclude the experience, each student organized a short presentation on a robotic surgery topic of their choice to be presented to the group, with suggested topics including procedure specific overview with steps and literature review, robotic cost, robotic learning curve, or new robotic technology under development.
Simulator Curriculum
The first week of the curriculum was centered around student performance on the virtual simulator system (Intuitive Surgical and 3D Systems) in our simulation lab. Each day, students focused on a different fundamental aspect of robotic surgery training. Keeping in mind that very few of the simulation skills are truly mutually exclusive of one another, the curriculum was divided into days individually focusing on console orientation, camera manipulation, energy device use, dexterity, and suturing. The curriculum was mastery-based, with students instructed to repeat each assigned activity until graded at >90% with no critical errors committed. As students worked through each assigned activity, the number of attempts to successfully complete the task, time spent on the task, the number of times they achieved >90% scores, and the total number of critical errors committed during the exercise were recorded in order to elicit feedback from course preceptors and track progress. Specific daily simulator assignments are outlined in Table 1.
Graduating from Virtual Simulator and Engaging with the Patient Cart
During the second week, students were challenged to apply their experience gained on the virtual simulator and in the operating room by setting up the patient cart for inanimate suturing. Students were assigned individual one-on-one sessions with faculty with robotic expertise to practice docking the robot and inserting instruments, as well as several suturing and knot-tying drills.
Later in the second week, student experiences culminated with high-fidelity biotissue training models (LifeLike Biotissue, London, Ontario) simulating reconstruction steps for a pancreaticoduodenectomy (Figure 1). 10 Three different biotissue sessions were held with each enrollee and a hepatobiliary surgical oncologist—1 for students to perform the gastrojejunostomy anastomosis, another for the hepaticojejunostomy, and the final for the pancreaticojejunostomy. Each anastomosis was constructed as though it were native human tissue using single- and double-layer techniques that incorporate simple interrupted sutures, running suturing techniques with V-Loc suture (Covidien LP, subsidiary of Medtronic. Dublin, Ireland), and Connell stiches.
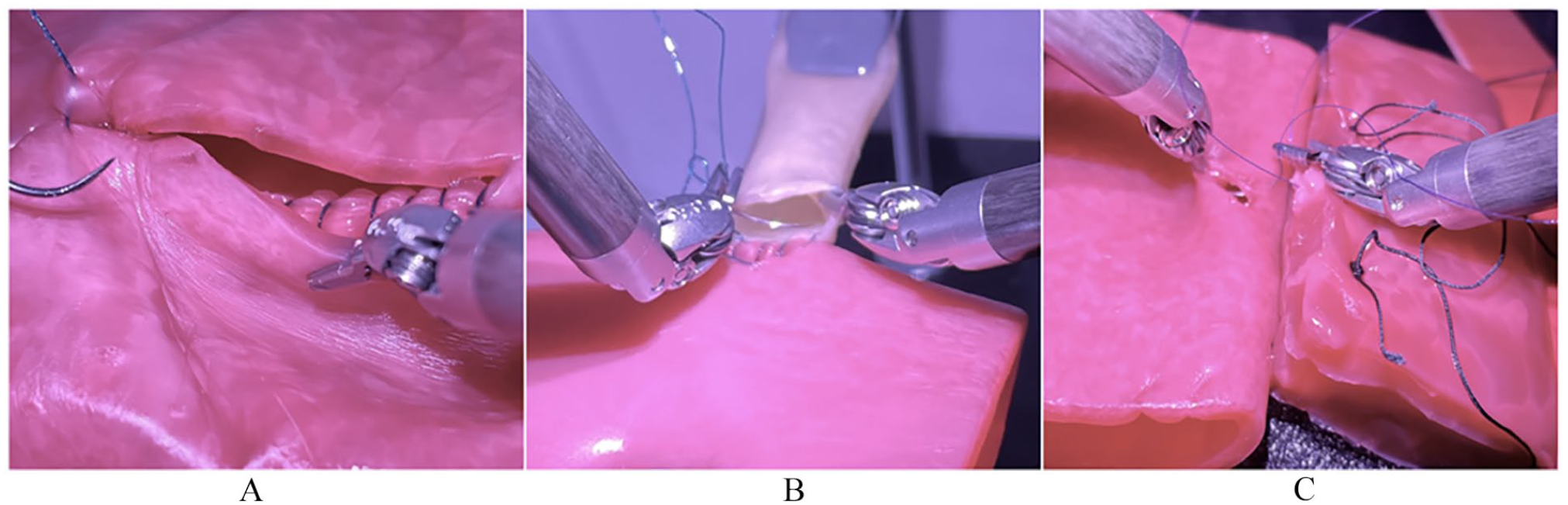
Representative images of biotissue models students utilized in creation of gastrojejunal (A), hepaticojejunal (B), and pancreaticojejunal (C) anastomoses to simulate a pancreaticoduodenectomy reconstruction.
Practical Exposure to Robotic Surgery in the Operating Room
An important aspect of the rotation experience when students were not directly working on the console was engaging in robot-assisted cases in the operating room. Students engaged from numerous perspectives including observers, bedside assistants, and by sitting at the dual console when available. Students had access to a video library of edited robotic procedures and were encouraged to review operative steps and approaches in detail prior to case participation. Students had the opportunity to position the patient cart to the bedside, to set up and break down cases, exchange instruments, and assist with procedures at the bedside. These experiences were important reinforcements of the online training modules and didactics, as well as valuable opportunities for observing ergonomics of the robot, effective utilization of instruments, experience with optimal port placement, and understanding how surgeons employ different instruments and techniques during operations. Students were encouraged to join cases in numerous surgical subspecialties that they were not exposed to during their third-year surgical clerkship including bariatric surgery, surgical oncology, thoracic surgery, cardiac surgery, urology, otolaryngology, and gynecology.
Value Proposition for Early Exposure to Robotic Surgery in Medical School
The current landscape of graduate medical education has yet to widely integrate robotic surgery into training curriculum in a comprehensive manner. As applications for robot-assisted surgical management continue to broaden and become more pervasive, we anticipate that robotic surgery will eventually be embraced and integrated into graduate medical education as laparoscopy has, with likely development of an analogous certification such as a fundamentals of robotic surgery skills certification. We expect that robotic surgery will likely become an integral part of surgical training, and early exposure to this technology and platform of surgical care will benefit senior medical students pursuing surgical specialties.
Currently, of those medical students who do have exposure to robotic surgery during surgical rotations, evidence indicates that students do not find that experience or environment to be effective or motivating in terms of promoting medical student education. 11 This has led to a call for incorporating legitimate medical student roles in the operating room during these cases in order to create a better learning experience for students. 11 We believe the curriculum we have developed provides students with adequate training to accomplish this aim.
This early exposure to robotic surgery provides our students with skills that will serve them well as soon-to-be surgical residents and has afforded them an unparalleled level of proficiency on the robot as they embark on their dedicated surgical training (Figure 2). The hours spent on the simulator and serving legitimate roles in the operating room will jumpstart their training so that they are further along on the robot learning curve from the outset. At the time of matriculation into their residency program and graduation, and upon successful completion of this rotation, each student is provided with a letter from the course preceptor outlining the extensive experience the student had during this rotation, including time spent on the simulator, simulator modules completed, online training modules completed, and details of each case the students were involved in and what their role(s) was/were during each case. This letter will serve as evidence of each students’ experience so that they are able to become credentialed at their training site(s) and become more involved in robot-assisted cases from the outset of their residency training.

Organized summary of experiences during rotation to promote robotic proficiency for senior medical students as they matriculate into surgical residency.
Future efforts will aim to quantify and assess students’ experiences in order to better understand how this educational opportunity impacts medical students’ perspectives of their education and their preparedness for surgical residency. Additionally, future iterations of this rotation will aim to expand didactics from other surgical subspecialists on the role of the robot in their specialty and provide more robust and diverse biotissue-based experiences.
Conclusion
Here we describe the first reported robotic surgery rotation curriculum developed specifically for senior medical students in an attempt to enhance their understanding of the robotic-assisted platform and develop their skills to jumpstart their learning curve for training in surgical residency.
Footnotes
Acknowledgements
The authors would like to thank the leadership and staff of the West Virginia University David and Jo Ann Shaw Center for Simulation Training and Education for Patient Safety (STEPS), and particularly Russell Doerr, for the support of this course.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institutes of Health under award number 5U54GM104942-04 (B.A.B.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
All authors have met criteria for authorship and ethical adherence. Data pertaining to this manuscript has not been previously published in a peer-reviewed journal or any other format.
Author Contributions
Study concept and design: CLM, ALV, JWM, MEH, AAT, CRS, BAB. Drafting of the manuscript: CLM, ALV, BAB. Critical revision of the manuscript: CLM, ALV, JWM, MEH, AAT, CRS, BAB.