
Abstract
COVID-19 has disrupted the status quo for healthcare education. As a result, redeployed doctors and nurses are caring for patients at the end of their lives and breaking bad news with little experience or training. This article aims to understand why redeployed doctors and nurses feel unprepared to break bad news through a content analysis of their training curricula. As digital learning has come to the forefront in health care education during this time, relevant digital resources for breaking bad news training are suggested.
Are Redeployed Doctors and Nurses Prepared to Break Bad News?
Across the world, newly redeployed doctors and nurses are staffing coronavirus disease 2019 (COVID-19) wards. Many are anxious due to the uncertainly of what they face, and some staff are fearful of caring for patients at the end of their life. In addition to the challenges of providing end-of-life care in often unfamiliar environments, staff must also break bad news to patients and their next of kin, often remotely due to strict no-visiting policies. Although the ability to communicate effectively is a prerequisite for all doctors and nurses in the United Kingdom,1,2 the fear and anxiety around breaking bad news (BBN) may be unsurprising as many staff are from specialties that do not frequently care for and converse with patients at the end of their lives. Despite the fears and complexities surrounding BBN to patients and those close to them, evidence shows that it is a teachable specialist skill.3,4
Exploring Postgraduate BBN Training Requirements
To better understand why redeployed doctors and nurses feel unprepared to break bad news, the breadth and depth of BBN training must be considered. Postgraduate training, regulated by the General Medical Council (GMC) and Nursing and Midwifery Council (NMC)5,6 in the United Kingdom, comprises 9 core curricula for medicine and 2 key documents for nursing (see Table 1).
Medical curricula and nursing documents included in the analysis.
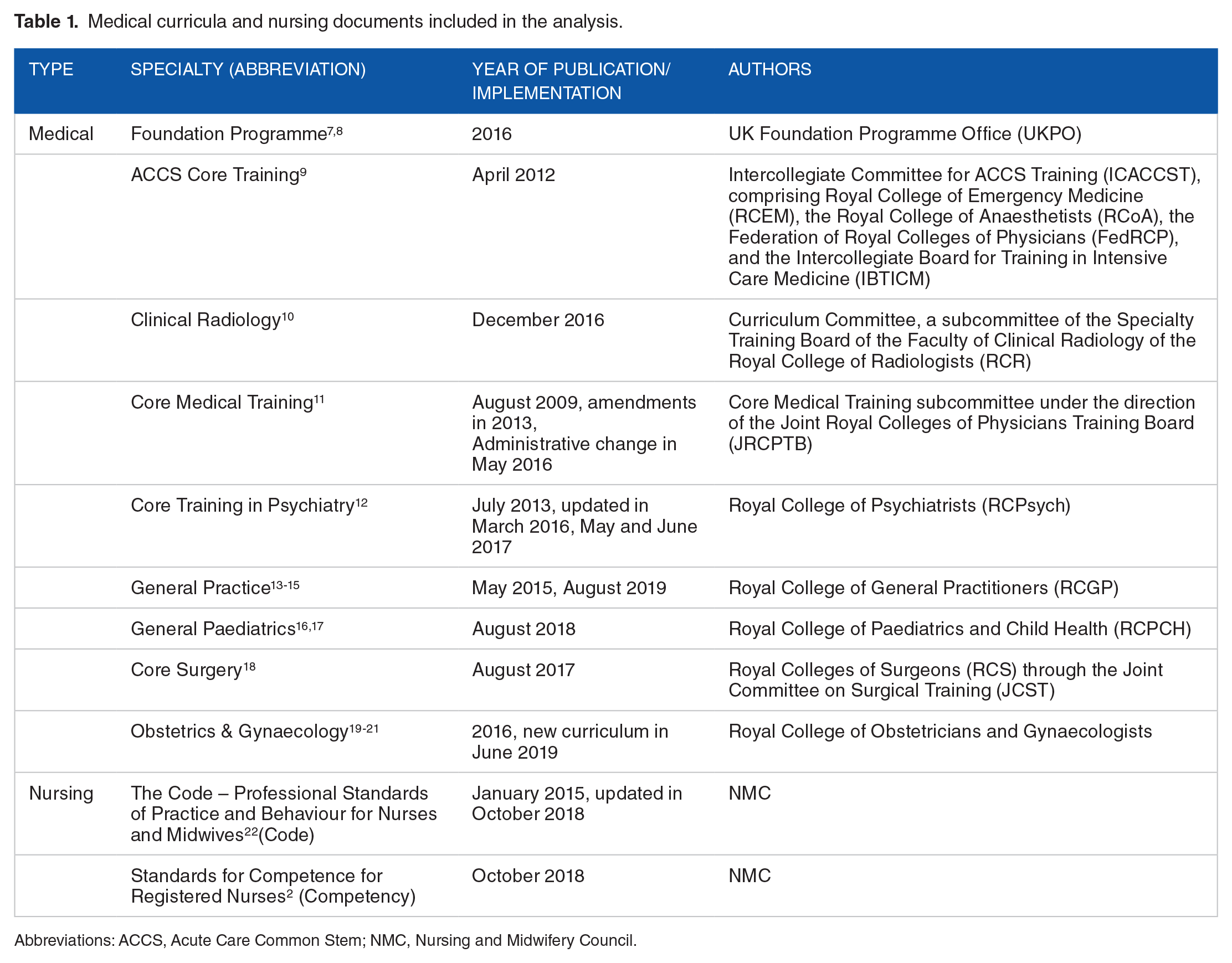
Abbreviations: ACCS, Acute Care Common Stem; NMC, Nursing and Midwifery Council.
Content analysis 23 of these curricula and documents reveals that BBN was referenced 56 times, with a large variation between curricula being observed (see Figure 1).

Number of breaking bad news curriculum requirements in each curriculum/document. NMC indicates Nursing and Midwifery Council.
When BBN curriculum requirements were presented, they were typically categorised as either ‘knowledge’, ‘skills’, or ‘behaviours’. Four curricula had a greater emphasis on BBN and included most curriculum requirements: Acute Care Common Stem and Core Medical Training had the most comprehensive lists of curriculum requirements (n = 39 and 38, respectively), followed by Obstetrics & Gynaecology (n = 33) and Core Surgery (n = 19). The curriculum requirements present across all 4 curricula are presented in Table 2. Unfortunately, the other documents had little or no mention of BBN (see Figure 1). The NMC documents did not mention BBN training but included broad phrasing and categories related to communication skills which left room for interpretation.
Curriculum requirements common to ACCS, CMT, O&G, and CS curricula.
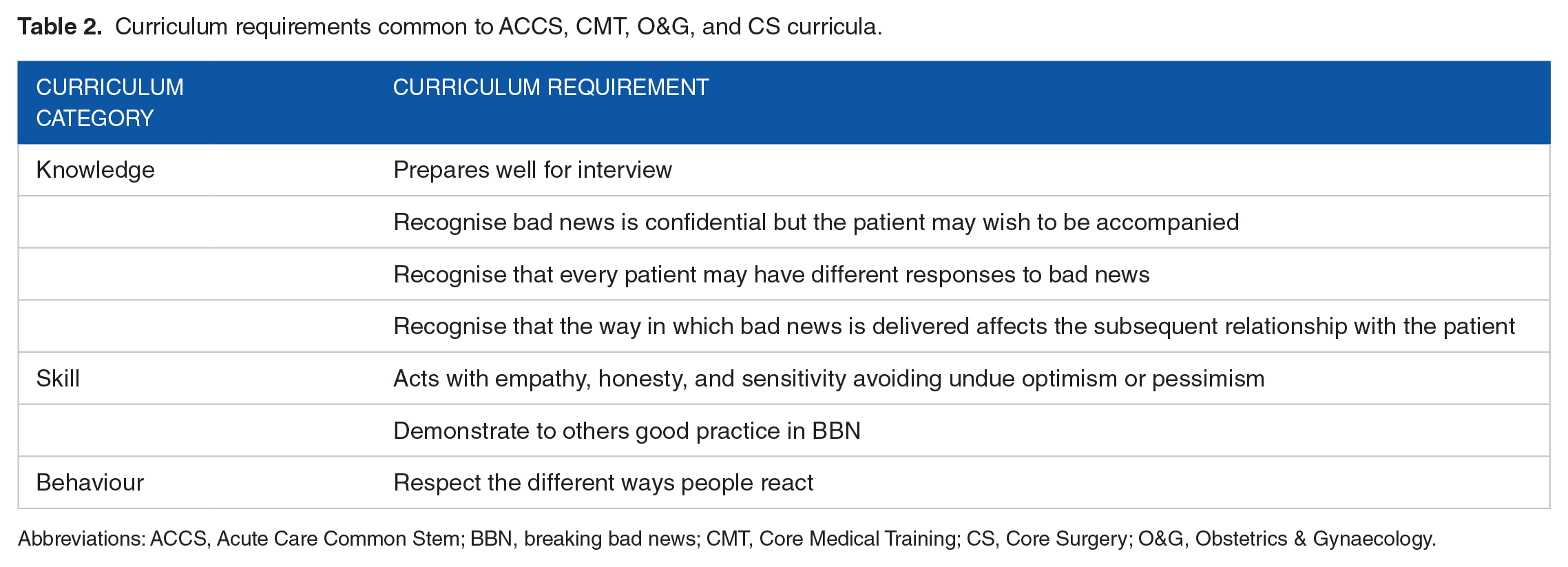
Abbreviations: ACCS, Acute Care Common Stem; BBN, breaking bad news; CMT, Core Medical Training; CS, Core Surgery; O&G, Obstetrics & Gynaecology.
This analysis emphasises the disparity in BBN curriculum requirements across the core specialties. Although 4 curricula were exemplary in listing curriculum requirements, the lack of emphasis on the Foundation Programme and NMC documents was concerning, even without the added pressures caused by COVID-19, as studies have shown that almost 80% of newly qualified junior doctors had initiated BBN with their patients, and more than 90% had experience of patients initiating conversations. 24
How to Support Redeployed Doctors and Nurses to Effectively Break Bad News Who Are Lacking Training?
The disparity in the BBN curriculum requirements across specialties now presents a pressing challenge in health care settings where doctors and nurses have been redeployed to COVID-19 wards, often working outside of their comfort zone. Many would argue that the best BBN training is through experience and practice, but in the COVID-19 era, this luxury is not afforded to redeployed staff. Therefore, interventions to support these staff are needed, and many are already available, especially in the digital space.
Some organisations may already have infrastructure in place to support their staff. For example, as part of the ‘Transforming End of Life Care in Acute Hospitals’ programme, the Transforming End of Life Care (TEOLC) team at University College London Hospitals NHS Foundation Trust was set up in 2014. During the COVID-19 pandemic, the team have played a key part in training and supporting redeployed staff across the Trust, especially on having compassionate conversations with patients and those important to them on treatment escalation planning, advance care planning, and end-of-life care. To engage with growing numbers of staff, an extensive teaching programme based on the SPIKES 6-step protocol 25 and the 4 points of agreement for a consultation (context, issues, story, and plan) 26 has been provided through lectures, Q&A sessions, webinars, and videoconferences.
For the purposes or social distancing and safety, digital learning has come to the forefront. These modes of learning may already feel familiar to learners, as the integration, acceptance, and use of digital technologies in education has increased rapidly in the last decade 27 and altered the way we learn and think.28,29 Digital learning is frequently used in workplaces and for continued professional development, 27 ,29-31 and as most doctors and nurses own smartphones, mobile applications (apps) can be used for reference and training. 30
Useful Digital Resources in the Current Crisis and Beyond
There are a number of digital learning resources readily available for BBN training (Table 3). Many of the resources are related to end-of-life care. However, some resources have been recently updated specifically to aid those having difficult conversations related to COVID-19.
Useful digital resources for breaking bad news training.

Abbreviations: COVID-19, coronavirus disease 2019.
Conclusions
Coronavirus disease 2019 has disrupted the status quo for health care education and, in turn, BBN training. It has also revealed the lack of BBN training in our clinical workforce. Many face-to-face courses, which were a common and effective form of BBN training, 3 have been cancelled for social distancing. Educators, such as the TEOLC team, have had to respond to the challenge of developing and delivering alternative methods of training at a previously unseen pace. Digital learning has come to the forefront in health care education during this time, as it facilitates remote learning and is readily accessible in the clinical setting. Digital technology opens up a wealth of resources; websites and apps are available for reference and training, and modern digital devices can facilitate videoconferences for learning and for communication between patients, those important to them, and health care staff.
These resources may not replace the BBN training that is gained through practice and experience, but they can act as a helpful adjunct, especially for those who are not regularly using these skills in their practice. However, the development and deployment of learning resources in place of traditional teaching methods must not go unchecked; further research is needed to better understand their potential.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors are supported by the NIHR Imperial Biomedical Research Centre.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have contributed to the content of this commentary. They have revised it critically for important intellectual content and approved the final submitted version. They agree to be accountable for all aspects of the work.