
Abstract
Introduction:
Understanding placebo and nocebo responses (context/meaning effects [CMEs]) is fundamental to physician agency. Specific instruction in CMEs is often lacking in medical education. Patient–practitioner interactions may challenge medical students’ understanding of biomedical causality and the nexus between this, practical ethics and professionalism across various conceptual and applied aspects of CMEs. This study compared the corpus of knowledge and phronesis related to CMEs between Australian graduate medical students and rheumatologists to gain a sophisticated understanding of this relationship to inform curriculum development.
Method:
In 2013 and 2014, the authors surveyed third-year medical students undertaking a graduate programme in an Australian medical school and Australian rheumatologists to ascertain their understanding of placebo and nocebo responses. The survey ascertained (1) the alignment of the respondents’ understanding of CMEs with accepted facts and concepts; (2) opinions on the ethical status of CMEs; and (3) responses to 2 scenarios designed to explore matters of biomedical causality, practical ethics and professionalism.
Results:
There were 88 completed surveys returned, 53 rheumatologists and 35 students. Similar proportions within each group identified CMEs, with most (n = 79/88 [89.8%]) correctly recognising a placebo (rheumatologists: 50 [94.3%], students: 29 [82.9%]) and approximately three-quarters (n = 65/88 [73.9%]) correctly recognising nocebo effects (rheumatologists: 39 [73.6%], students: 26 [74.3%]). Statistically significant differences between practitioners and students were observed in relation to the following: placebo responders and placebo responsiveness; placebos as a ‘diagnostic tool’; placebos usage in clinical practice and research, and nocebo effects.
Conclusions:
Physicians require an awareness of CMEs and the fact that they arise from and influence the effective agency of health care professionals. Curricular emphasis is needed to permit an honest assessment of the components that influence when, how and why patient outcomes arise, and how one’s agency might have neutral or negative effects but could be inclined towards positive and away from negative patient outcomes.
All aspects of medical encounters have placebogenic or nocebogenic meaning1-3 or context effects,4,5 though clinicians may not be aware of their operation within the medical encounter. The experience of illness, which encompasses contextual appraisal (from which meaning is derived), is shaped by the context around the patient when ill, and key to this is the nature of the treatment and the person delivering it. Therefore, understanding placebo and nocebo context/meaning effects and responses (which can improve or detract from one’s experience of illness) is central to a physician’s agency.
Evers et al distinguish between placebo and nocebo effects and placebo and nocebo responses: placebo and nocebo response includes all health changes that result after administration of an inactive treatment (i.e., differences in symptoms before and after treatment), thus including natural history and regression to the mean. The placebo and nocebo effect refers to the changes specifically attributable to placebo and nocebo mechanisms, including the neurobiological and psychological mechanisms of expectancies.
6
Hence, placebo effects refer to valid, measurable psychobiological events as distinct from response to placebo incorporating a genuine placebo effect in addition to the effects of natural healing, regression towards the mean, the Hawthorne effect, Will Rogers effect, and Simpson’s paradox. 7
Context and meaning effects (CMEs) arise from ‘the human interactions and contexts in which healthcare consultations take place’, 8 potentially augmenting or detracting from treatment effects, highlighting the practical importance of CMEs to physicians. Hence,
CMEs in everyday medical encounters are highly specific valid psychobiological events that can enhance or detract from treatments.
They attach to almost every form of treatment/intervention even if a ‘traditional’ placebo such as an inert tablet is not given and are highly clinically relevant to everyday medical encounters.
There is reasonable data – both quantitative and qualitative – demonstrating that an intervention to augment placebo 9 or minimise nocebo 10 responses can improve treatment outcomes and/or reduce treatment ‘side effects’.
Recognition of nocebo effects is necessary to understand why some patients may resist the initiation of or not adhere to effective treatment regimens.11-16
These concepts should be embedded the continuing education of students and current physicians.
Specific instruction in CMEs is often lacking in medical education, possibly explaining doctors’ ‘incoherent understanding of the placebo effect’. 17 Problematic nocebo effects are recognised in the historical and anthropological record. 18 Understanding one’s potential to elicit CMEs reflects phronesis – the ‘ability to navigate through conflicting demands . . . the practical wisdom necessary to translate virtue into the right action’. 19 Understanding CMEs is thus a fundamental ethical competency, 20 intrinsic to establishing a functional professional identity. 21 CMEs are ‘clinical threshold concepts’ 22 without which the patients’ variable responses to medical interventions can be inexplicable.
Threshold concepts are ‘conceptual gateways’22,23; medical curricula should ‘enable students to negotiate epistemological transitions, and ontological transformations’. 22
Students experience difficulties with medical education’s explicit commitment to ‘empathy, compassion, and altruism’ and its tacit commitment to ‘detachment, self-interest, and objectivity’, hence some students re-conceptualize themselves . . . as technicians . . . narrow their professional identities to an ethic of competence . . . adopting tacit values and discarding explicit professionalism . . . Others develop non-reflective professionalism, an implicit avowal that they best care for their patients by treating them as objects of technical services . . .
24
Consequentially, there may be stasis or a decline in students’ moral reasoning capacity 25 and empathy 26 over time; this is contentious27,28 and likely dependent on metrics unrelated to future workplace behaviours. Rheumatologists should be familiar with CMEs through their training, experience of the debate around placebo usage, 29 and have a nuanced understanding of CMEs 30 including non-deceptive strategies to improve outcomes and arguably reduce harms.13,31-33
Here, we describe the results of a survey of medical students from an Australian graduate medical programme and of Australian rheumatologists. The purpose of the survey was to compare the corpus of knowledge and phronesis related to CMEs between Australian students and rheumatologists because patient–practitioner interactions may challenge students’ understanding of biomedical causality and the nexus between this, practical ethics and professionalism 34 across various conceptual and applied aspects of CMEs. We wished to gain a more sophisticated understanding of this relationship to inform curriculum development in light of CMEs’ importance to the contemporary physician. 6
Methods
Subjects
Convenience samples were obtained from 2 groups: (1) commencing third-year students in the Sydney Medical Programme attending an orientation day in January 2013 who were invited through flyers at the session and a brief presentation to participate in an online survey, and (2) rheumatologists were recruited via the monthly e-newsletter of the Australian Rheumatology Association, which hosted an invitation to participate in an online survey; 1 email reminder was sent. Both participant groups accessed the study though a yes/no gate on the online Participant Information Statement. This statement informed participants that logging in and submission of the partially/fully completed survey was proof of consent.
Ethics statement
The student and rheumatologist studies were approved by the University Institutional Review Board (IRB).
Procedure
Participants in both sub-studies accessed an online SurveyMonkey™ questionnaire, we developed regarding definitional aspects of the placebo–nocebo response and their opinions regarding the nature, ethical and scientific status of CMEs via a 5-point Likert-type scale of strongly disagree to strongly agree. Scenarios relating to CMEs in the context of (1) opioid administration and (2) the effect of surgery were posed to participants.
Statistical methods
Descriptive statistics were used to analyse survey responses in both subsets. Associations between item responses and respondent demographics were explored using χ2 analyses in both subsets. Responses of agree/strongly agree and disagree/strongly disagree were aggregated into 2 loci due to small numbers. Where cell sizes permitted, and the variables were categorical, the Pearson χ2 statistic was reported. If cell sizes were small, the Fisher exact test P-value was reported. Where the variables were considered ordinal, the linear-by-linear association χ2 statistic was reported. Demographic variables included sex (men, women), age (⩽25 years, ⩾26 years), academic background (undergraduate, postgraduate), cultural identity (Australian, other), and student origin (domestic, international) for the student study. In the rheumatologist study, the variables were sex (men, women), age ranges (31-40, 41-50, 51-60, and 61-70), country of origin and ethnic identification, nature of qualifications, nature of practice (private, mixed, or public practice), and years in practice. The level of significance was set at α = 0.05 for all analyses and IBM SPSS v21.0 (IBM Corp., Armonk, NY, USA) was used to conduct all analyses.
Results
Of the potential 293 Sydney Medical Programme students approached for the study in 2013 (245 domestic and 48 international), 11.9% (n = 35) returned a completed survey. These student participants did not differ, in terms of demographics, from the broader student cohort. Sixty-one of the 343 members of the Australian Rheumatology Association commenced the survey; 53 (86.9%) completed sufficient items to be included in rheumatologist-student comparisons. Non-completers did not differ demographically from completers. Survey completers were predominantly men (rheumatologists: 35/52 [67.3%], students: 19 [54.3%]). Most students (n = 30 [85.7%]) were under 31 years, whereas most rheumatologists were older than 40 years (41/52 [78.8%]), with 53.8% (28/52) aged between 51 and 70 years. The most common student cohort entry degree was an Undergraduate Science course (n = 21/35 [60.0]), and the majority were of domestic origin (30 [85.7%]). Almost three-quarters of the rheumatologists (n = 38/52 [73.1%]) had higher degrees and most (n = 43/53 [81.1%]) had trained in rheumatology in Australia, 5 (9.4%) in North America and 2 (3.8%) in New Zealand. One-third (n = 18/53 [34.0%]) worked solely in private practice, 39.6% 21 mixed private/hospital location, and 18.9% 10 were employed hospital practitioners. Most (n = 30/53 [56.6%]) had practised for 20 or more years.
We asked respondents about their level of agreement with a range of statements about the nature of a placebo and a nocebo (see Table 1). Similar proportions within each group identified CMEs, with most (n = 79/88 [89.8%]) correctly recognising a placebo as an inactive compound used as a control to a medicine in a clinical trial (rheumatologists: 50 [94.3%], students: 29 [82.9%]) and that surgery could also elicit placebo effects (rheumatologists: 47/53 [88.7%], students: 27/28 [96.4%]). Approximately three-quarters (n = 65/88 [73.9%]) correctly recognising nocebos as negative effects following administration of a placebo, again with no statistically significant difference between the 2 groups (rheumatologists: 39/53 [73.6%], students: 26/35 [74.3%]).
Rheumatologists’ (n = 53) and students’ (n = 35) understanding of context/meaning effects.
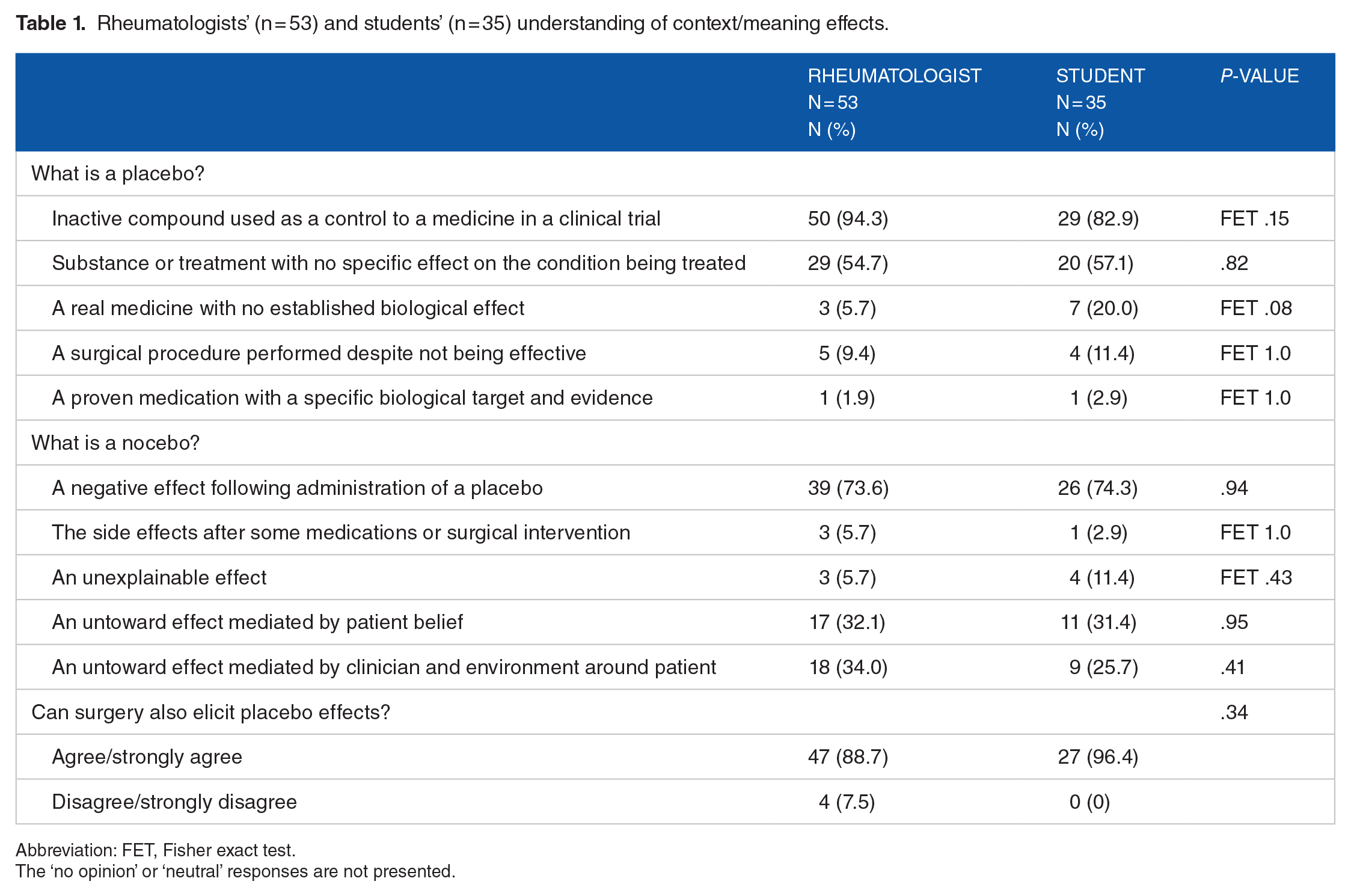
Abbreviation: FET, Fisher exact test.
The ‘no opinion’ or ‘neutral’ responses are not presented.
When asked about the application of placebo and nocebo in practice, students were more inclined to agree that if told by a doctor that a medicine was ‘just a placebo’, they would think it was useless (rheumatologists: 14/53 [26.4%], students: 18/27 [66.7%]; P = .001; see Table 2). A larger proportion of rheumatologists disagreed with the statement that a coloured capsule containing a medication would have the same effect as a plain white tablet (rheumatologists: 36/53 [67.9%], students: 12/27 [44.4%]; P = .009). Rheumatologists were also more likely to disagree that placebos could be used as a ‘diagnostic tool’ to determine if a patient had a genuine organic disease (rheumatologists: 46/53 [86.8%], students: 18/27 [66.7%]; p = .006).
Rheumatologists’ (n = 53) and students’ (n = 35) understanding of context/meaning effects use in clinical practice.

The ‘no opinion’ response is omitted from this table.
We asked participants about identifying placebo responders and placebo responsiveness (see Table 2). Students were more likely to agree that placebos work better in anxious patients, or those who complain a lot (rheumatologists: 6/52 [11.5%], students: 8/27 [29.6%]; P = .005).
There were no significant differences in responses about beliefs regarding the ethical status of CMEs (Table 3). However, when presented with a scenario in relation to miscalculated opioid dosing, students were more disposed to agree that sub-therapeutic levels of opioid would result in inadequate pain relief (rheumatologists: 11/50 [22.0%], students: 19/27 [70.4%]; P < .001; Table 4). There were no differences in response to a surgical scenario (Table 5).
Rheumatologists’ (n = 53) and students’ (n = 35) beliefs regarding the ethical status of context/meaning effects.

The ‘no opinion’ response is omitted from this table.
Rheumatologists’ (n = 53) and students’ (n = 35) understanding of context/meaning effects relating to a scenario of miscalculated opioid under-dosing.

The ‘no opinion’ response is omitted from this table. Scenario: a hospital resident Doctor prescribes an opioid pain-relieving medicine for one of your patients. After reviewing the prescription on a ward round several hours later, you realise that the dose was miscalculated and that the patient was actually given a very small dose of opioid (much less than would be required for adequate pain relief).
Rheumatologists’ (n = 53) and students’ (n = 35) understanding of context/meaning effects relating to a surgical scenario.
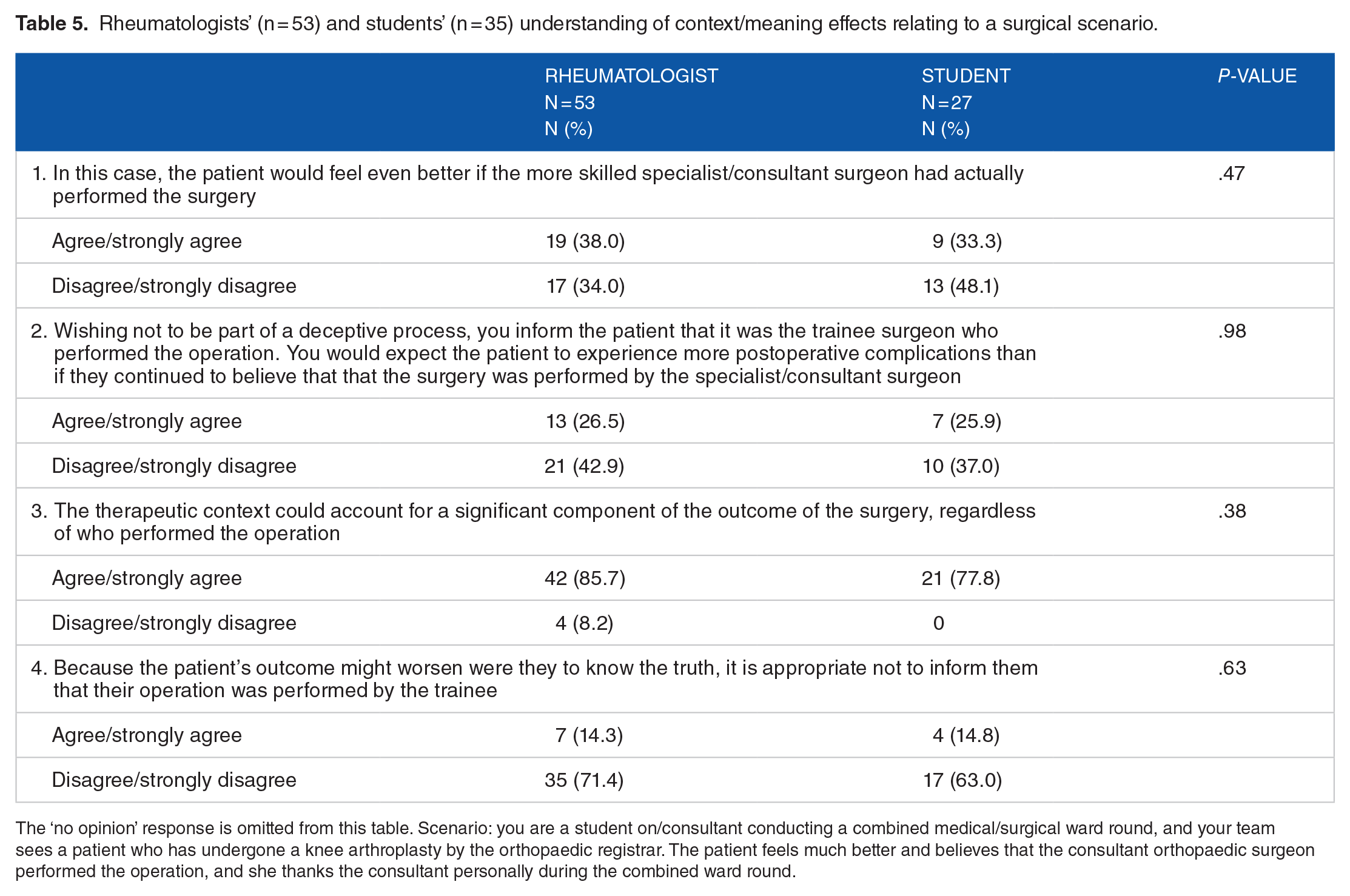
The ‘no opinion’ response is omitted from this table. Scenario: you are a student on/consultant conducting a combined medical/surgical ward round, and your team sees a patient who has undergone a knee arthroplasty by the orthopaedic registrar. The patient feels much better and believes that the consultant orthopaedic surgeon performed the operation, and she thanks the consultant personally during the combined ward round.
Discussion
This study compared the state of knowledge regarding selected aspects of CMEs in a group of graduate medical students with community and academic rheumatologists. The premise was that rheumatologists would represent an exemplar group of physicians providing longitudinal person centric care and appreciate aspects of physician agency that would generate CMEs.
For students to derive the most benefit from their clinical immersion experience, an understanding of the general ‘subjectivity and constructedness’ 35 of medical knowledge is necessary. Subjectivity and constructedness is most evident in CMEs. This study is novel because there are few studies relating to medical students’ understanding of placebo effects as distinct from being experimental subjects 36 or voicing pure attitudes and opinions. 37 To our knowledge, there has been no systematic assessment of medical students’ knowledge of CMEs contrasted to that of experienced clinicians with the aim of informing curricula.
The ethical acceptability and prevalence of placebo usage has been assessed in nurses, 38 interns, 39 physicians,40,41 rheumatologists, 41 psychiatrists, 17 and GPs/family physicians,42-49 with several inter-group comparisons.17,38,40,41,44 However, interpretation of these and other studies is problematic due to a lack of uniform definition of the term ‘placebo’ and how this term was understood by study participants. 50
Likewise, there is scant literature pertaining to practitioners’ assumptions regarding the frequency, nature, and extent of CMEs and their contribution to treatment outcomes. The net therapeutic effect of any intervention is the sum of the specific effect of the intervention in question, natural bodily healing, regression to the mean, the Hawthorne effect, ‘Will Rogers phenomenon’, 51 Simpson’s paradox, 52 and the true extent of the placebo effect. 7 It has been posited that the majority of any measurable response in osteoarthritis is a consequence of context effects. 53
In this comparison, the conceptual knowledge of CMEs was similar between students and rheumatologists, though knowledge of the contextual effect of placebo is was surprisingly less broad than for nocebos. Both groups identified that in routine practice placebo effects occur commonly and that placebo effects may occur in addition to pharmacologic effects with medication.
Both groups identified that CMEs may be modulated by the information given to patients. Both groups disagreed with the proposition that either placebo or nocebo effects occurred and were predictable in certain people. Whether or not placebo and nocebo susceptibility/sensitivity will be a focus of ‘precision medicine’, a number of candidate genes that affect neurotransmitters have been identified.54,55 Polymorphism in the enzymatic activity of COMT rs4680 in the prefrontal cortex relates to placebo analgesia. 56 Hall et al 57 posit a neuropharmacologic genetic network – the ‘placebome’ – which may explain the additive effect of placebo to an active drug, among other observations. The participants’ response – disagreement – was congruent with the literature.
Placebos were identified as an active intervention – not tantamount to doing nothing – and it was appreciated that placebos can potentially cause harmful effects, yet both groups’ responses indicated ambivalence in relation to the concept of placebos as unethical or deceptive. However, this ambivalence appeared to be dispelled when equipoise existed; if a placebo was non-inferior to a supposed therapeutic agent, many respondents felt placebo use was justifiable. Likewise, where a placebo could be employed to minimise harms from administering an active medication, respondents from both groups felt it was ethically justifiable. Regardless of participants’ clinical experience, generally there is a notion of ambivalence about placebo administration unless the context is made very specific.
There were trends, but no true statistical differences between groups’ understanding that placebos are often given in clinical practice outside of the context of trials which may reflect experienced clinicians’ greater familiarity with this practice. It may be that students had insufficient clinical experience to recognise this phenomenon and hence there is merit in building knowledge that can be shaped by future clinical experience. Yet, there were some statistically significant differences between the 2 groups of respondents.
Placebo responders
More rheumatologists disagreed with the proposition that placebos ‘work better in anxious patients’. In contrast to the responses of either group, neuromapping techniques have identified multiple ‘top-down’ regulatory pathways affected by emotion that influence placebo responses.54,58,59 However, there is difficulty in correlating neural mapping with the somewhat variable prediction studies. When considering personality traits, placebo responders appear to have greater trait optimism, suggestibility, empathy and neuroticism whereas trait pessimism, anxiety and catastrophisation are more common in persons exhibiting nocebo effects. 60
Although these findings are of interest and potential clinical relevance, it is not possible at present to reliably predict placebo responsiveness on the basis of any one psychological trait.61-64 It is possible either that that experienced clinicians appreciate that a single psychological variable is unlikely to be a key mediator of placebo-responsiveness and do not characterise patients on the basis of anxiety per se; alternatively, they may be unaware of this.
Placebo response as a ‘diagnostic tool’
Historical viewpoints characterising placebo diagnostic injections as tools to detect ‘malingering’ 65 are in all circumstances ‘unethical’,64,66 and placebo responsiveness cannot differentiate disease from non-disease. 64 However, most rheumatologists disagreed with this proposition, in comparison with 66.7% of students. The concept of a ‘trial of therapy’ should be discouraged on the basis that organic (and often serious) disease may improve with a placebo. There is an inconsistency between a belief in placebo as a diagnostic tool and the appreciation that ‘organic’ disease can respond to placebo.
CMEs in clinical practice
We explored participants’ beliefs relating to the effect of CMEs in clinical practice, recognising that there are no ‘correct’ responses to such questions. It is not possible to make valid inferences from the participants’ responses over and above noting a general alignment with the responses with prior studies where it has been established that therapies are employed in a context, dose or manner where it can have no biological effect, 50 and therapeutic outcomes are principally driven by patient expectations. 49 Many patients endorse interventions with a potential benefit and low risk of harm; patients recognise that the context of the medical encounter and physician agency may drive the effect, 67 particularly in older patients. Parents support placebos for children ‘when the targeted condition was psychological in nature or considered minor’ and support placebo use guidelines. 68 A public discourse has emerged around open (non-deceptive) placebo usage 29 in dose-extension pragmatic randomised trials. 69 Motivational interviewing (MI) is essentially a technique of persuasion, 70 and assessment of placebo responses deriving from MI may be a productive research area. 71
Nocebo effects
In this study, there were no significant differences between students’ and rheumatologists’ understanding of or beliefs around nocebo effects. Nocebo effects are exceedingly common,11-13,72 and consequentially, often dissuading initiation and continuance of effective therapies. 13 Nocebo effects can be generated from inaccurate information and hearsay from non-qualified (and qualified) persons,13,14 through social contagion 73 and expectations, 72 and can be countered. 74 This study focussed less on nocebo effects reflecting the time of its design. Exploring whether reported complications of therapy are non-pharmacologic nocebo effects may reduce inappropriate terminations of therapy if the explanation of the effect is made by a trusted placebogenic rather than nocebogenic health care professional.
Limitations
This is a single institution student study with small convenience sample sizes, due in part to a wish to avoid student ‘survey fatigue’. 75 Although the orientation session was ‘compulsory’, only about 40% of the year cohort attended as expected. 76 As no formal attendance record was made, it was not possible to distinguish responses from attendees and non-attendees. A proposed follow-up student study was not undertaken due to low initial recruitment numbers. In the rheumatologist study, 1 post-invitation reminder was sent to avoid the possibility of coercion. Both survey response rates were comparable with those noted by Aitken et al, 77 ranging between 7.5% and 13.2% depending on location, noting that a survey’s topic ‘may be part of the problem’ in the sense that in 2013-2014, and placebo and nocebo effects were considered less deserving of participation in comparison with other more prominent issues and the ‘survey invitation may have languished at the bottom of many in-trays’. 77
Conclusions
Placebo and nocebo effects (CMEs) derive from human interactions in clinical encounters. Grasping that CMEs occur is a threshold concept in the understanding of the variance in patient responses to therapy. Students and physicians need to be aware when they and the medical encounter may generate CMEs. In this study, a number of these aspects are variably appreciated.
It has been proposed that ‘health-care professionals should be trained to maximise placebo effects and minimise nocebo effects’. 6 However, it is uncontroversial to propose that minimally all health care professionals must first have an awareness of CMEs given their ubiquity and influence on the outcomes of health care encounters. Curricular emphasis is needed to permit an honest assessment of the components that influence when, how and why patient outcomes arise, and how one’s agency might have neutral or negative effects but could be inclined towards positive and away from negative patient outcomes.
Footnotes
Acknowledgements
The authors thank the two anonymous reviewers of this paper for their constructive analysis and helpful criticism.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MHA was responsible for the development of the research question, design and concept of the work. GL was responsible for biostatistical input. DF was responsible for content expertise relating to context medical effects and IK for clinical ethics expertise. All authors contributed to the interpretation of the data, its discussion, reviewed and agreed to the final version of the paper.