
Abstract
Objectives:
Curriculum analysis is an essential process in exploring the validity of assumptions behind the curriculum and judging its perspectives, goals, and objectives. This study analysed the curriculum of the Internal Medicine Residency Programme at the Sudan Medical Specialisation Board, exploring the programme’s strengths, weaknesses, and areas for improvement.
Materials and Methods:
A qualitative descriptive analysis method using Harden Ten Questions framework was used, implemented through document analysis. Thematic analysis was used to categorise the findings following the Harden Ten Questions framework.
Results:
The analysis of this curriculum using Harden Ten Questions framework revealed that it is built on needs assessment, with clear objectives and contents, good organisation of the contents and a precise management process. However, there is a need to improve the areas related to training strategies, training methods, assessment methods and the learning environment.
Conclusions:
This study showed that the curriculum is built to meet the needs of the Sudanese community. The contents fit for internal medicine clinical residency and the methods of training are likely to foster long-life learning. The curriculum needs some improvement particularly in the following areas such as clinical teaching, trainee assessments, and learning environments. Harden Ten Questions framework for curricula was practical to some degree in analysing the postgraduate curriculum. However, some suggestions have been made regarding the original framework to make it more adaptable to curriculum analysis at postgraduate level. The systematic analysis is transferable to the analysis of other undergraduate or postgraduate medical curricula in Sudan.
Keywords
Introduction
In education and specifically in health profession education, the word ‘curriculum’ means ‘the statement of the intended aims and objectives, content, experiences, outcomes and processes of an educational programme, including the following; a description of the training structure, a description of expected methods of learning, teaching, feedback and supervision’. 1 According to Harden, 2 ‘a curriculum is a programme of study where the whole is greater than the sum of the individual parts’.
A curriculum analysis refers to an attempt to tease a curriculum separately into its parts. To scrutinise those parts and the way they fit together to make a whole, to identify the beliefs and ideas to which the designers were dedicated and which either explicitly or implicitly shaped the curriculum, and to examine the implications of these commitments and beliefs for the quality of the educational experience.
3
Thus, curriculum analysis as a process aims at exploring the validity of assumptions behind the curriculum and judging its perspectives, goals, and objectives. The analysis process examines the curriculum from different angles and approaches; however, its strengths and weaknesses are not always apparent to trainees, faculty, or curriculum designers. 4
This article analyses a postgraduate medical education (PGME) curriculum in Sudan. The Internal Medicine Residency Programme (IMRP) is one of the oldest programmes of the Sudan Medical Specialisation Board (SMSB); more than 400 medical specialists have already graduated, and more than 300 residents are currently enrolled. The IMRP is a 4-year speciality training (48 months’ duration) delivered to residents in Sudan at 15 accredited training centres.
The IMRP curriculum, developed in 1995, has regularly been updated and reviewed by the Curriculum Committee for Internal Medicine Training, most recently in 2017, when the needs of trainees and stakeholders were considered.
Published literature on postgraduate training in internal medicine worldwide is minimal. 5
Harden 6 Ten Questions framework, a tool used for curriculum analysis, was developed and proposed in 1986. This framework has since been used at several universities worldwide, due to its high validity and reliability.7,8 Our study aimed at analysing the curriculum of the IMRP at the SMSB, exploring its strengths and weaknesses and areas for improvement.
Materials and Methods
To analyse the IMRP curriculum, we used a qualitative descriptive approach that depended on a document analysis method. Harden Ten Questions of curriculum development (Table 1) was the tool used to conduct the analysis. Most of the analysed documents are found at https://smsb.gov.sd/ar/.
Ten questions to be asked when planning a course or a curriculum. 6
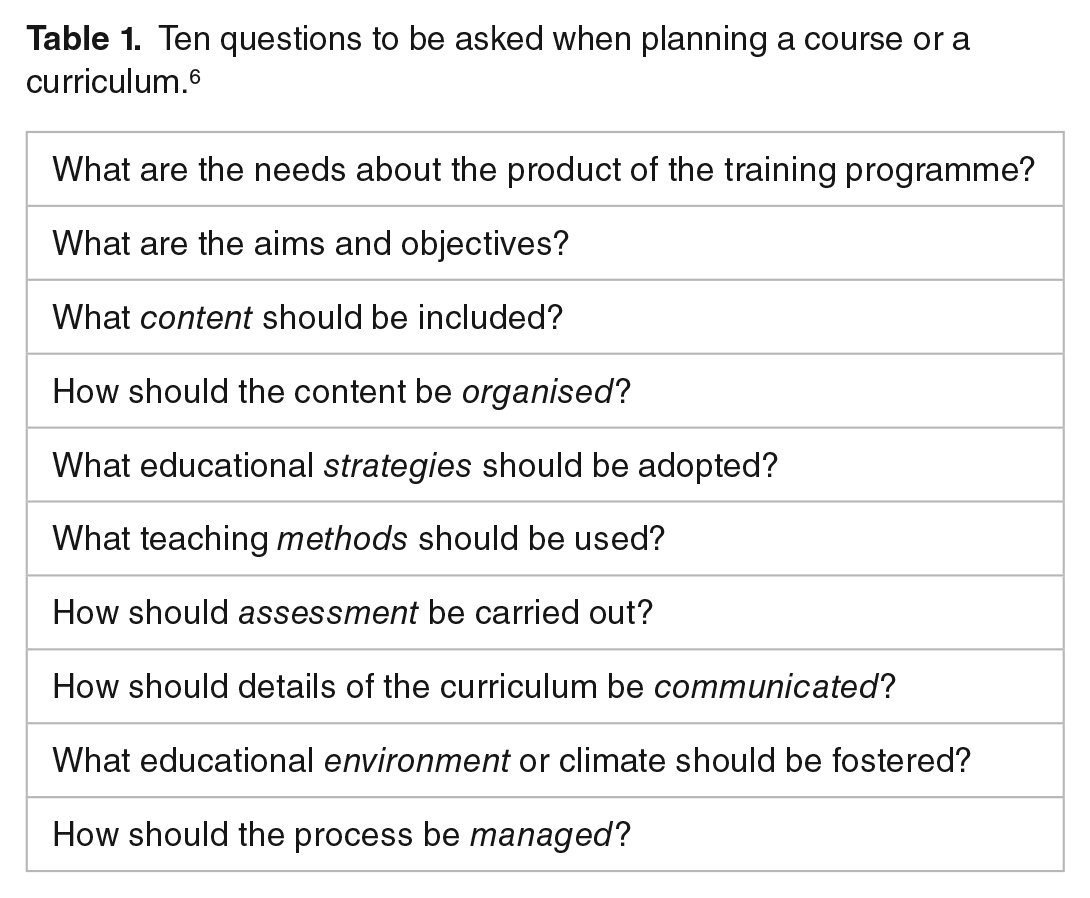
This framework concerns the needs of the products of this training curriculum or curriculum goals. Curriculum content and its organisation are also included, along with educational strategies, teaching tools, assessment tools, learning environment implementation, and curriculum management. The researchers analysed how the current programme in the SMSB responded to these questions, using a method involving a content analysis of curriculum materials and documents. Thematic analysis was used to categorise the findings of the resulting analysis. To ensure the internal validity of the obtained data, the researchers applied triangulation and multiple sources of data, including the curriculum documents, assessment policies, and training regulations.
This study was approved by the Ethical Committee at the Sudanese Federal Ministry of Health (Certificate No. 2-12-2016), and permission to conduct the study was obtained from the presidents of the SMSB.
Results
Table 2 provides a summary of the main findings of the curriculum analysis and the sources of the obtained data.
Summary of the main findings of the curriculum analysis and the sources of the obtained data.
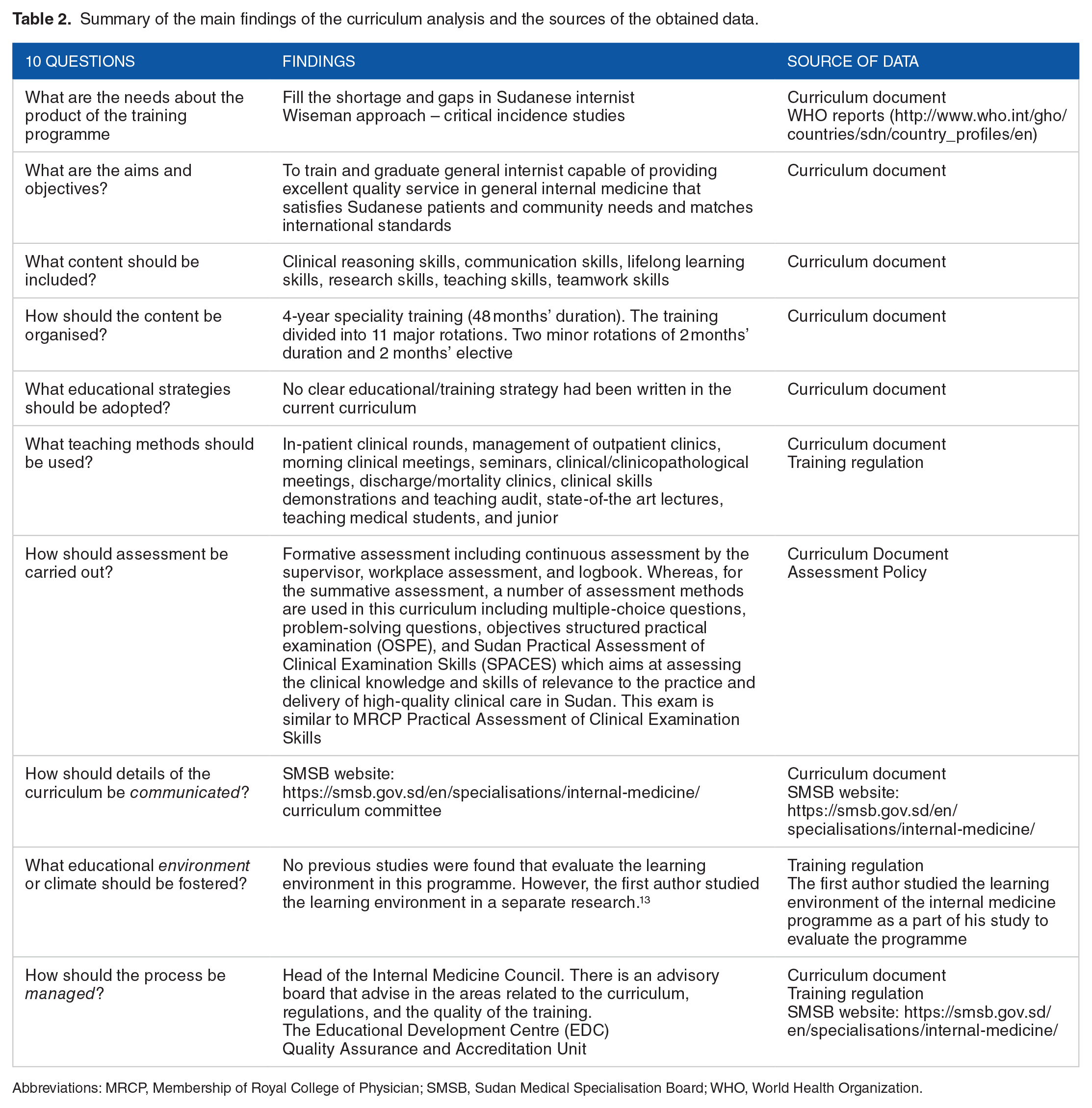
Abbreviations: MRCP, Membership of Royal College of Physician; SMSB, Sudan Medical Specialisation Board; WHO, World Health Organization.
What are the needs of the products of the IMRP?
This curriculum was developed to address the shortage of Sudanese physicians. 9 The total number of physicians in Sudan per 1000 population, according to World Health Organization (WHO) statistics, was 3.05 in 2014. 10 The SMSB adopted a multifaceted approach to exploring problem identification and needs assessment. The need assessment was performed using Wiseman approach together with critical incidence studies and an analysis of existing internal medicine curricula taught in Khartoum and Gezira University; the purpose was to identify built-in curriculum objectives and contents.
What are the aims and objectives of IMRP?
This curriculum aims to train and graduate general internists capable of providing excellent quality service in general internal medicine, which satisfies Sudanese patients and community needs and matches international standards. The SMSB internal medicine curriculum learning objectives are centralised around trainees being up to date; managing common communicable diseases; effectively communicating with their patients; planning, conducting, and writing up research directed towards local health needs; recognising the role of teamwork; teaching and training undergraduates; and upgrading their skills using new and advanced technologies. 11 The curriculum objectives are shown in Table 3.
The SMSB curriculum learning objectives.

What content should be included?
The current IMRP curriculum is built on 6 domains: (1) clinical reasoning skills, (2) communication skills, (3) lifelong learning skills, (4) research skills, (5) teaching skills, and (6) teamwork skills.
There are fundamental training courses for all residents in this curriculum, including cardiopulmonary resuscitation/advanced life support, medical professionalism and medical ethics, communication skills, and research methodology.
How should the content be organised?
The current curriculum is taught in 4 years (48 months). The training is divided into 11 major 4-month rotations and 2 minor 2-month rotations, with 2 one-month electives. The major rotations include general internal medicine, and the minor rotations include cardiology respiratory medicine, gastroenterology, neurology, and nephrology. Two electives are chosen from among haematology/oncology, emergency medicine, dermatology, rheumatology, radiology, and psychiatry.
After completion of training, with a minimum of 36 months training occurring in Sudan, and after obtaining satisfactory confidential reports from supervisors and obtaining approval of the dissertation (thesis) 4 months before the final exam, the residents are eligible to sit for the final exam of the programme.
What educational strategies should be adopted?
No clear educational/training strategy had been identified in the written curriculum. However, through analysing the curriculum and its objectives, we were able to describe its guiding principles: the application of adult learning principles, experiential learning, and social cognitivism as a guide for training strategies.
The IMRP curriculum is delivered through a variety of learning experiences. Through practice, residents learn clinical skills appropriate to their level of training and position within the department. This includes learning with peers, work-based experiential learning, and independent self-directed learning.
What teaching methods should be used?
A broad range of opportunities for learning and learning methods are included in this curriculum, including in-patient clinical rounds, management of outpatient clinics, morning clinical meetings, seminars, clinical/clinicopathological meetings, discharge/mortality clinics, clinical skills demonstrations and teaching audits, lectures on the state of the art, teaching medical students and junior colleagues, journal clubs, case presentations, and self-directed learning.
How should the assessment be carried out?
A wide range of methods are used in this curriculum, broadly categorised as either summative (assessment of learning) or formative (assessment for learning); both categories are used for student assessments. Summative assessment methods include multiple-choice questions, problem-solving questions, objective-structured practical examinations (OSPE), and the Sudan Practical Assessment of Clinical Examination Skills (SPACES), which aims at assessing clinical knowledge and skills relevant to the practice and delivery of high-quality clinical care in Sudan. The format of this exam is similar to that of the Membership of Royal College of Physician (MRCP) Practical Assessment of Clinical Examination Skills, 12 but it is contextualised for practice in Sudan. Formative assessment includes continuous assessment by a supervisor, workplace assessment, and logbooks.
How should the curriculum details be communicated?
The current curriculum details are communicated on the SMSB website (https://smsb.gov.sd/ar/). The curriculum booklet includes details of the curriculum objectives for the 11 rotations, their contents, entry requirements, training and assessment methods, and learning resources. The Curriculum Committee is responsible for communicating any changes in curriculum to trainers and residents. The Curriculum Committee has also prepared a detailed logbook used in this training to ensure that the curriculum objectives are met.
What educational environment or climate should be fostered?
Taha et al 13 studied the learning environment of this programme using postgraduate hospital educational environment measure (PHEEM). They identified areas of strength and weakness in the educational environment of the curriculum. One strength was the collaboration between the residents and doctors and a sense of belonging to a team. However, significant problems had been identified in the learning environment in this curriculum including the absence of a contract of employment that provides information about hours of work, absence of an informative inductive programme and training manual, and lack of good supervision at all times. 14
How should the process be managed?
This programme is managed by the Internal Medicine Council, responsible for the distribution of the residents and for monitoring the training sites. It comprises (1) a chairman, (2) a reporter, (3) a director of the Training Committee, (4) a director of the Exam Committee, and (5) a director of the Curriculum Committee. The entire training process is managed by the academic affairs secretary and the head of the council. An advisory board advises in areas related to the curriculum, regulations, and the quality of the training.
The Educational Development Centre (EDC) at the SMSB prepares the curriculum with the involvement of content experts, ensuring that the curriculum is created according to the standards. The Quality Assurance and Accreditation Unit in the EDC accredits the training as well as the trainers, based on the endorsed guidelines and checklists.
The Training Committee also approves proposals and their implementation as well as the basic courses. The Curriculum Committee communicates any changes or updates to the curriculum to trainers and residents. The structure of this programme is illustrated in Figure 1.

Structure of the Internal Medicine Residency Programme. SMSB indicates Sudan Medical Specialisation Board.
Discussion
A curriculum analysis is vital in providing high-quality evidential feedback to curriculum designers, implementers, trainees, and medical teachers. Although Harden Ten Questions framework, used to analyse this curriculum, is relevant for undergraduate, postgraduate, and continuing professional development programmes, most studies which have used this framework took place at the undergraduate level, both for entire curricula and at course levels.7,8 To our knowledge, ours is the first study to use the framework to analyse a postgraduate curriculum.
The current analysis revealed that in design, the IMRP curriculum is objective-based. Curriculum designers following this model aim for 4 objectives: (1) reaching agreement on general aims and specific objectives for the curriculum contents, (2) constructing the contents to achieve these objectives, (3) defining the curriculum in practice by testing its capacity to achieve the objectives, and (4) communicating the curriculum to teachers.
But recent worldwide trends in PGME are moving towards the adoption of a competency-based medical education (CBME) curriculum, 15 through which trainees are exposed to certain competencies. The CBME is an approach meant to ensure that graduates develop the competencies required to fulfil their patients’ needs. It de-emphasises time-based training and promises greater accountability, flexibility, and learner centeredness. 16
The curriculum objectives and contents were accordingly analysed. We found that when compared with other curricula and international frameworks, 4 the following domains should be included in the current curriculum: the behavioural and social sciences, community medicine, epidemiology, global health, hygiene, medical anthropology, medical psychology, medical sociology, public health and social medicine, other managerial skills in practice (for example, determining priorities or the cost-effectiveness of health care and a knowledge of referral systems), as well as complementary medicine, including unorthodox, traditional, or alternative practices. 17
The present analysis showed that clinical rounds were the main training methods in this curriculum. Clinical rounds are considered excellent opportunities to learn clinical and communications skills. Useful recommendations for improving the value of this learning method include pre-clinical and post-clinical round sessions, which provide learning opportunities through discussing management and diagnostics options and receiving feedback. 18
Involvement of ambulatory training and primary health care training is also recommended to meet international requirements for internist competencies. 19 Recent trends emerging in PGME also should be considered in this curriculum, including the use of new learning technologies, such as simulation-based education and e-learning. One e-learning advantage for this programme may also include an online discussion forum, which can provide great opportunities to share clinical cases, ethical dilemma scenarios, and radiological images. Recent studies have also demonstrated the significance of small group learning, interprofessional training, and problem-based learning in residency training. 20
There are 15 accredited training centres for this programme, almost all teaching hospitals and specialised centres. Recent recommendations have outlined that training for internal medicine residents should not take place only in hospitals but should also include ambulatory training and training in primary health care. 21
Comparing the admission criteria in this curriculum with those of other curricula revealed similarities between admission to this curriculum and other curricula in the region, including in Egypt and Jordan,22,23 and worldwide, including the United Kingdom, Germany, the Netherlands, Australia, and Ireland.24,25 These programmes rely only on an entrance exam, differing from programmes in Saudi Arabia, the United States, and Canada, in which the matching system is used to admit residents.21,26
The present analysis revealed that most assessment tools used in this curriculum are related to summative assessment; these include multiple-choice questions, problem-solving questions, objectives structured practical examination (OSPE), and SPACES. These findings contrast with recent trends in PGME, aiming to move towards the weight of formative assessment compared to summative assessment. Another study showed that residents must become comfortable seeking formative assessment/feedback, and trainers must offer it frequently. 27 Meanwhile, a typical end-of-rotation exam after 4 years of training, as used in this curriculum, is not conducted in close time–based proximity to the actual educational experience, so it cannot succeed in providing immediate, direct feedback to the learner. Therefore, it is crucial to emphasise the use of formative assessment and of progress tests for this programme after each year of the training rotation. Researchers in the United States have demonstrated that progress testing for PGME assessment is unique and promising and should be used for residency programmes. 28
Including other assessment tools is also suggested for this curriculum including direct observation of procedural skills (DOPS), case-based discussion (CbD), mini-clinical evaluation exercise (mini-CEX), and multisource feedback (MSF). 29
The current IMRP curriculum needs to be transformed to a competency-based curriculum. This could be achieved by designing and adopting a national competency framework for the development of these competencies and developing specific measures and units to guarantee the achievement of these objectives. Several countries worldwide have already adopted competency frameworks for undergraduate and postgraduate curricula.30-34
There are some limitations to this analysis. It focused on the planned curriculum and depended mainly on existing documents. It was also conducted for only one programme. Further in-depth evaluation including quantitative and qualitative methods is recommended.
Conclusions
This study showed that the curriculum is built to meet the needs of the Sudanese community. The contents fit for internal medicine clinical residency and the methods of training are likely to foster long-life learning. The curriculum needs some improvement particularly in the following areas: clinical teaching, trainee assessments, and learning environments.
The systematic, critical approach in this article is transferable to the analysis of other undergraduate or postgraduate medical curricula in Sudan. This could be a useful guide for medical faculty involved in the design, development, and improvement of any medical curriculum.
Harden Ten Questions framework for curricula was practical to some degree in analysing the postgraduate curriculum. However, some suggestions have been made regarding the original framework to make it more adaptable to curriculum analysis at postgraduate level.
The suggested modifications to the Harden Ten Questions framework
Harden Ten Questions framework is a valid framework used in analysing postgraduate curricula. However, to make it more relevant to current PGME, we recommend some adjustments to comply with recent advances worldwide. We suggest the following:
Adding 2 questions: (1) What are the entrustable professional activities and developmental milestones of this curriculum? and (2) How should the training staff be trained to implement this curriculum?
Modify the second question in the Harden original Ten Questions framework to What is the competency framework to be followed?
Modify the third question to What content should be included in each year of the residency programme? (Figure 2).
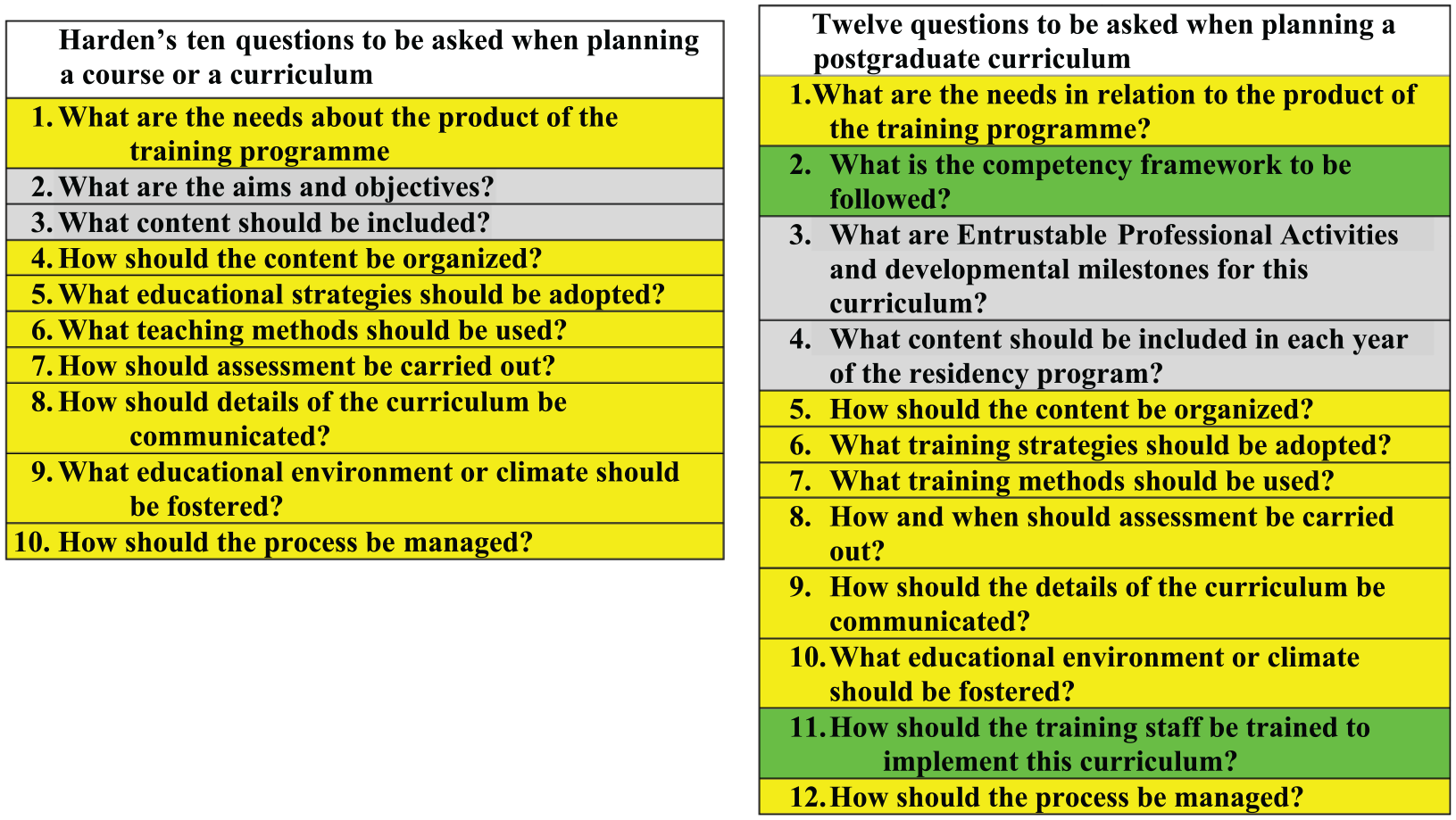
The original Harden Ten Questions framework (in the left side) and the suggested modification (in the right side).
The systematic and critical approach to curriculum analysis described in this study is transferable to the curriculum analysis of other undergraduate or postgraduate medical curricula in Sudan and the surrounding region. This could be a useful guide for medical faculty involved in the design, development, and improvement of any medical curriculum.
Footnotes
Acknowledgements
This work would not have been possible without the support of the administration of the SMSB and the council of the Internal Medicine Programme. We are especially indebted to the Educational Development Centre in the SMSB, who provided us with support for this review.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MHT and MEA designed the study, conducted the analysis of the curriculum, analyzed the data, and wrote the manuscript. YA, contributed to the qualitative analysis and provided critical revision of the article. All the authors finally approved of the last version of the manuscript to be published