
Abstract
Background:
The adoption of community-based medical education
Methods:
This research was designed as a qualitative (ethnographic) study that used a structured questionnaire, to obtain written statements from 120 fourth-year undergraduate medical students describing their experience during their CoBME training at BDH. The structured questionnaire in the form of an evaluation form was self-administered, consisted of only open-ended questions grouped into 4 main sections and was distributed manually (hard copy) to the participants.
Results:
Of the 120 questionnaires distributed, 84 were returned, giving a response rate of 70.0%. When asked to indicate what they liked or disliked about their CoBME training, ‘Good educators/staff’ and the ‘Poor attitude of some doctors’ were the themes that scored highly (25.1% and 19.4%) in the ‘likes’ and ‘dislikes’ category, respectively. Some of the major challenges faced during the CoBME training at BDH included: exposure to new learning environment (14.2%), clinical practice context (12.6%), and language barrier (7.2%). Participants stated that they gained knowledge of how to perform certain clinical procedures and acquired core clinical skills in the areas of formulating management and managing some medical emergencies during their training at BDH. Increasing the duration of training (25.6% coverage) was suggested as a major way to enrich students’ experience during the training at BDH.
Conclusion:
Findings by this study reveal that CoBME is a valuable pedagogical tool to enhance learning in undergraduate medical education and that more work is required to improve the quality of CoBME training in BDH. We believe that the findings by this study will inform future planning of CoBME training programmes in BDH.
Introduction
In response to the diverse changes to the practice of medicine and the reorganisation of health care systems, the curriculum of undergraduate medical education in many countries has undergone extensive revision. 1 In addition, the ongoing changes to the role of physicians and the needs of patients have generated the need to modify undergraduate medical curricula and introduce new teaching and learning strategies such as community-based medical education (CoBME).1,2
The adoption of CoBME in to the undergraduate training programme of many medical schools aligns with the SPICE (Student-centred, Problem-based, Integrated, Community-based, Electives and Systematic) model for medical curricula proposed by Harden et al.
3
According to Worley and Couper
4
CoBME can be defined as medical education that is based outside a tertiary or large secondary level hospital (and which) is focussed on the care provided to patients both before the decision to refer to a tertiary hospital and after the decision to discharge the patient from such care.
Numerous benefits of CoBME have been reported in the literature and include: promoting a more patient-orientated perspective; offering a broader range of learning opportunities for students to acquire knowledge, skills and attitudes; and providing students with the opportunity to learn about general and family medicine practice in a rural setting.5,6
To harness the numerous benefits of CoBME, the faculty of health Sciences University of the Free State (UFS) introduced CoBME into its undergraduate medical curriculum in 2015 through a collaborative community-based education (CBE) initiative titled ‘Ho-Rutana’ (teach-each-other) initiative in Springfontein (Xhariep district of the Free State). 7 As part of the CoBME programme, all fourth-year medical students were expected to spend 2 weeks in Botshabelo District Hospital (BDH) and its clinics (1 week in the district hospital, 1 week in the clinics). The purpose of the initiative was to offer students the opportunity to learn about the differences in health care delivery in rural areas and to gain an insight into primary health care (PHC) as the backbone of the South African health system. Since the inclusion of CoBME into the curriculum and the commencement of CoBME programme in BDH, no known study has evaluated the quality of the CoBME training at BDH.
Programme evaluation is a systematic method for collecting, analysing, and using information to answer basic questions about a programme, 8 and it is a valuable tool for programme managers seeking to strengthen the quality of their programmes and improve outcomes. 9 As students are the major consumers of medical education, it makes them the ideal candidate to evaluate and provide feedback on the efficacy of their own course and learning environment. 10 To evaluate the quality of the CoBME programme in BDH, we explored students’ perceptions of their experience during their clinical training at BDH. In addition, suggestions on how to enrich the educational experience of the students during the CoBME posting were investigated. We anticipated that obtaining empirical data on students’ perspectives of the CoBME programme in BDH will reveal information about the effectiveness of the programme on student learning and also help to identify problematic areas that can inform future planning and strategies to improve the programme.
Study Context
Undergraduate medical studies at the Faculty of Health Sciences, UFS is offered as a 5-year programme structured into 3 phases and divided into 10 semesters, leading to a degree in Medicinae Baccalaureus and Chirurgiae Baccalaureus (MBChB). 11 Phase I (Semester 1) and Phase II (Semesters 2-5) (Years 1-3), are pre-clinical phases in which the content of the curriculum is arranged in system-based modules. Phase III, the clinical phase, runs from Semester 6 to Semester 10 (Years 4 and 5). 11 CoBME is offered during Semesters 7/8 (Year 4). Teaching and learning is conducted via clinic visits, bedside discussions, observation and hands-on skill performance under supervision, assignments and filling of hand-held logbook. 12 The placement also includes some after-hours work (call duty, 1 night/week during the 2 weeks placement). Assessment – at the end of the rotation – each student must hand in a signed logbook and all written assignments. Medical students (MBChB IV – Semester 7/8) do not receive separate marks for the CoBME placement. However, the marks obtained will contribute 20% to the module marks of the Family Medicine module in Semesters 9 and 10. 12
Methods
This research was designed as a qualitative (Ethnographic) study that made use of a structured evaluation form (Appendix 1) to obtain written statement from participants describing their experience during their CoBME training at BDH. 13 The structured evaluation form (ie, questionnaire) used in this study was self-administered and was distributed manually (hard copy) to participants. The form consisted of only open-ended questions grouped into 4 main sections.
Section A obtained information on what the participants liked or disliked about the CoBME programme in BDH, section B, highlighted the challenges the participants faced during the CoBME training in BDH, and in section C, participants were asked to report in their own words, what they learnt during the CoBME training at BDH. In the last section, section D, the participants were given the opportunity to provide suggestions on how students’ experiences could be enriched during the CoBME training in BDH.
This method of qualitative data collection using a questionnaire was chosen out of convenience, as it was impracticable to conduct face-to-face interviews for all of the participants and also achieve this within the specified timeframe allocated to the study, considering the logistical constraints and unique geographical context of the location of the study. In addition, our goal was to obtain extensive and diverse information from our target population, which made this strategy an ideal method to obtain rich and informative data from such a large number of respondents.
Study population
The target population included all registered fourth-year undergraduate medical students of the UFS that undertook the CoBME training in BDH during the 2017/2018 academic year. The survey population consisted of individuals who voluntarily agreed to participate in the study after reading and signing the informed consent forms. The sample consisted of 120 registered fourth-year undergraduate medical students.
Ethical considerations
Ethical approval was obtained from the Health Science Research Ethics Committee of the UFS (Ethical Clearance No.: ETOVS 08/2010).
Data collection and analysis
Prior to the official start of this study, a pilot study was conducted to test the suitability of the study’s design and methods, the chosen data collection method, and the overall structure of questionnaire. The pilot study consisted of 4 registered Year 4 MBChB students who met the criteria for the target population and voluntarily consented in filling the questionnaire. The findings of the pilot study confirmed the feasibility of the study approach (ie, adequacy of the chosen data collection method and the overall structure of the questionnaire), as the participants in the pilot study did not recommend changes to the structured questionnaire or the study design. Data obtained from the participants of the pilot study were included in the overall data of the study.
Placement supervisors who assisted in both the dissemination and collection of the evaluation forms aided data collection. Data were collected at the end of the last day of the 2 weeks CoBME training programme in BDH. Responses to the open-ended questions were read and re-read by the investigators, to familiarise themselves with the content. Content analysis was done using NVivo 12 software (QRS International Pty Ltd, Australia). Thematic analysis formed the cornerstone of the analysis, and specific attention was given to patterns and emerging themes. The 5 topmost themes with the highest percentage coverage for each category where plotted and presented as bar chart.
Results
This study achieved a response rate of 70.0%, as 84 of the initial 120 questionnaire were returned. Of the participants, 47.6% were men (n = 40) and 52.3% were women (n = 44).
Participants’ ‘likes’ or ‘dislikes’ of the CoBME programme in BDH
To obtain data on what participants like or dislike about the CoBME training in BDH, participants were requested to responds to the question ‘What do you like or dislike about the CoBME training at BDH?’ Content analysis of participants’ written responses gave 10 core themes for ‘likes’ and 6 core themes for ‘dislikes’, respectively. The 5 topmost themes with the highest percentage coverage for each category are presented in Figure 1. As seen in Figure 1, ‘Good educators/staff’ had the highest coverage (25.1%) in the ‘likes’ category, whereas ‘the attitude of some doctors’ had the highest coverage (19.4%) in the ‘dislikes’ category. Some excerpts from participants responses on ‘likes’ and ‘dislikes’ are presented in Table 1.

The 5 topmost themes in both ‘likes’ and ‘dislikes’ category.
Participants responses on ‘likes’ and ‘dislikes’ of the CoBME programme in BDH.

Other identified themes include: working independently (5.5%), good organisation (3.4%), learning environment (1.7%), clinical meetings/programmes (1.3%), good inter-professionalism (0.5%) – ‘likes’ category and poor teaching technique – ‘dislikes’ category.
Abbreviations: BDH, Botshabelo District Hospital; CoBME, community-based medical education.
Challenges encountered during the CoBME training in BDH
Analysis of participants’ accounts of the challenges encountered during their CoBME training in BDH yielded 11 themes. Most of the challenges reported by the participants centred on challenges faced when exposed to a new learning environment, presented under the theme new learning environment (14.2%) (Figure 2).
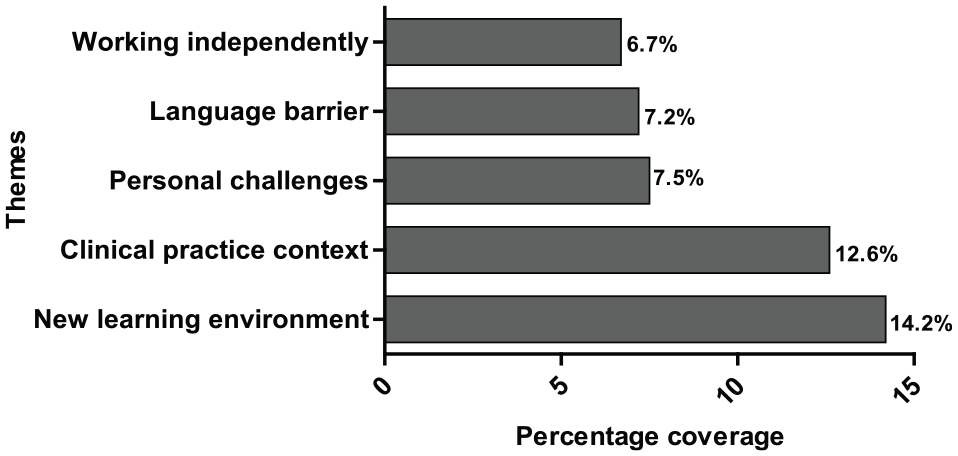
The 5 topmost challenges encountered by participants during their CoBME posting in BDH. BDH indicates Botshabelo District Hospital; CoBME, community-based medical education.
Other challenges reported by the participants are presented in Table 2 under the following themes: organisation (5.8%), group dynamics (5.2%), insufficient background medical knowledge (5.2%) (Table 2), limited hospital resources (3.2%), filling log book (3.6%), and limited time for rotations (1.4%).
Challenges encountered during the CoBME training in BDH.

Abbreviations: BDH, Botshabelo District Hospital; CoBME, community-based medical education.
What participants learnt during the CoBME training in BDH
Participants were asked to report in their own words, what they learnt during the CoBME training at BDH. Results as presented in Table 3 gave 12 themes. The highest ranked theme was ‘learning how to perform certain medical/surgical procedures (12.8%)’ (Table 3).
Knowledge gained during the CoBME training in BDH.

Abbreviations: BDH, Botshabelo District Hospital; CoBME, community-based medical education; CT, computed tomography; DM, diabetes mellitus; GP, general practitioner; HPT, hypertension; TB, tuberculosis.
Suggestions on how student’s experience can be enriched during CoBME at BDH
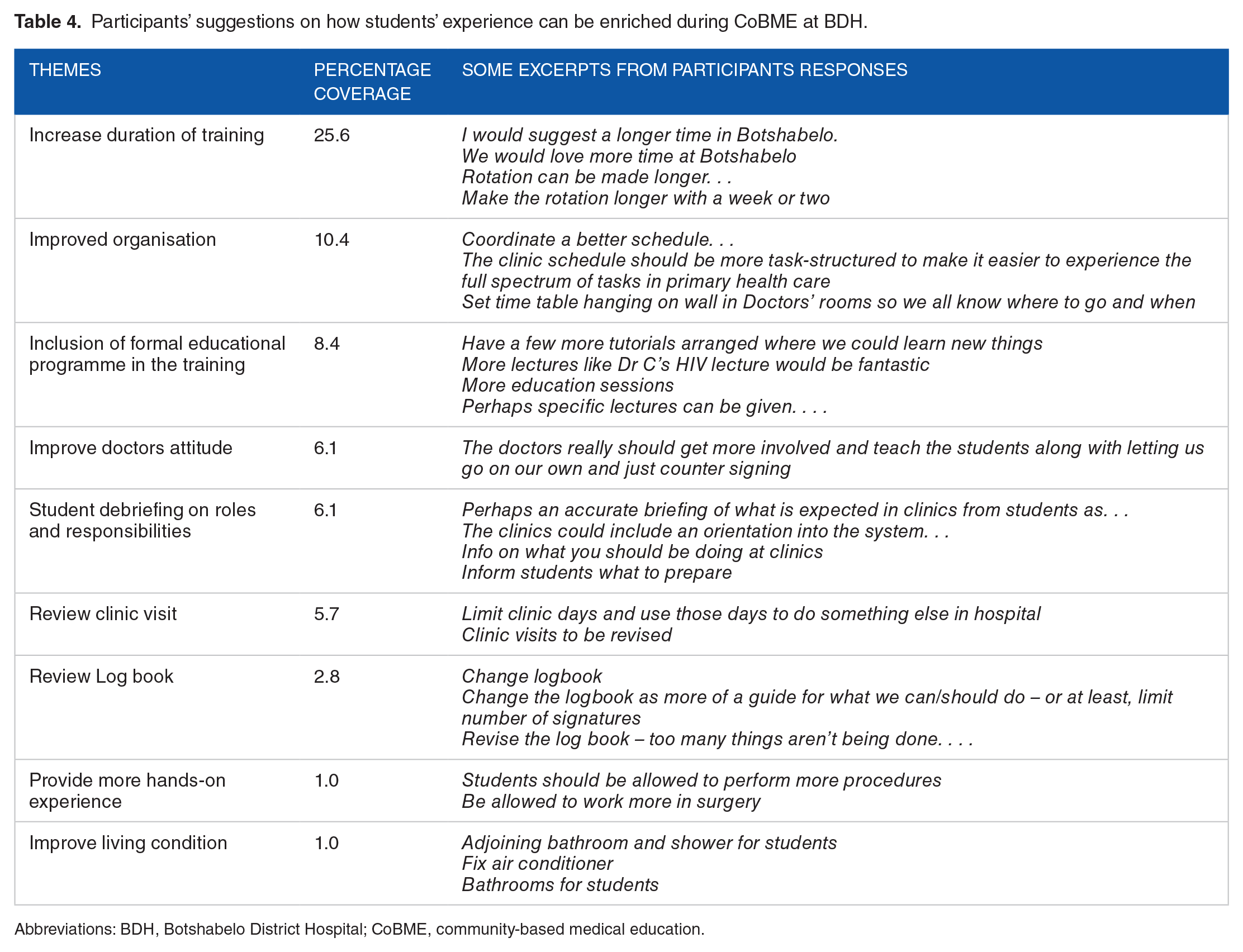
Participants’ suggestion on how to further enrich students’ experience during the CoBME at BDH was grouped into 9 major themes as presented in Table 4. Increasing the duration of CoBME training at BDH was ranked highest with 25.6% frequency. Participants also commented on the need to review the logbook and the improvement of the living conditions as ways in which students experiences can be enhanced during the CBE training. Furthermore, participants also made mention of the need for better organisation and the need to review the clinic visits (Table 4).
Participants’ suggestions on how students’ experience can be enriched during CoBME at BDH.
Abbreviations: BDH, Botshabelo District Hospital; CoBME, community-based medical education.
Discussion
It has been argued that programme evaluation is an essential indicator of programme effectiveness. 14 In the education sector, evaluation is widely used to generate information for policy, planning, design, implementation, assessment of result, improvement/learning, accountability, and public communication. 15 According to Kreber et al, 14 determining students’ perceptions of staff’s teaching performance; assessing students’ learning; and inviting student ratings are some of the approaches to programme impact evaluation. In this present study, we evaluate the quality of the CoBME programme in BDH in the Free State, South Africa, by obtaining students perception on their experience during their CoBME training.
Satisfaction (and dissatisfaction) refers to the evaluation of a service and comprises cognitive, affective, and attitudinal components. 16 Higher satisfaction is associated with consumer loyalty and has positive effect. 17 Similarly, understanding students’ sources of satisfaction and dissatisfaction has been highlighted as one major way to enhance students’ learning experience. 18 Students’ satisfactions has been reported to have had a positive effect on students’ school performances, personalities, and attitudes towards learning, and dissatisfaction to have had a negative effect on students’ personalities and attitudes towards learning. 19 It can be presumed that factors that culminate into students’ satisfaction are what students ‘like’ about their programme and those that precipitate dissatisfaction are their ‘dislikes’ about the programme. Prior studies have shown a strong positive correlation between liking the instructor/teaching experience and student satisfaction.20,21 Findings in this study reveal that participants liked the ‘Good educators/staff’ they encountered during their CoBME training in BDH. Their comments reflected that the educators were friendly, knowledgeable, and enthusiastic about teaching (Table 1). This is similar to findings by O’Sullivan et al, 22 wherein first-year medical students expressed their likeness for the positive approachable attitude of their educators and the enthusiasm manifested for teaching during their community-based clinical placement. In addition, participants of that study reported valuing the personal approach of their community educators whom, they felt were friendly and made an effort to get to know them as people. 22 These attributes were associated with positive learning experiences. 22 It is therefore probable that the good attitude displayed by the educators towards student acceptance and teaching during the CoBME, led to more appreciation by students, promoted satisfaction, and generated a positive learning experience. It has been reported that good quality practical work/hands-on activities can influence students’ interest and help them develop important skills and their understanding of concepts23,24 and that schoolwork that is interesting and engaging is a source of student satisfaction. 19 Participants of this study conveyed that they liked the fact that training was practical and hands-on (Table 1). It is thus probable that some participants of this study perceived the ‘hands-on experience’ as interesting work and derived satisfaction from it.
Over the years, the use of teaching staff as role models for professional behaviour has been an informal but integral part of medical training. 25 Students’ and medical graduates’ opined that a good role model must exhibit attributes such as integrity, openness, enthusiasm, compassion, and good relationships with patients. 25 It has been reported that senior doctors who show poor attitude and unethical behaviours cause distress and resentment in students under their supervision. 25 It is then very plausible that the ‘poor attitude of some doctors/educators’ caused distress and resentment in some of the participants of this study. Thus, making them to report it as a ‘dislike’ and probably a source of dissatisfaction in the CoBME training at BDH (Figure 1 and Table 1). This finding corroborates similar findings by Beelick 19 who reports that display of poor behaviour by teachers is a major source of student dissatisfaction. In this study, poor attitudes such as lateness to work, lack of organisation, inability to work under pressure, and rudeness to student and patients were reported (Table 1). In a study aimed at obtaining students’ perceptions of the relative advantages and disadvantages of community-based and hospital-based clinical teaching, O’Sullivan et al 22 report that students identified that aspects of course organisation can influence learning experience. Good organisation of teaching and learning engender positive learning experience in contrast to a disorganised state where students are unsure what is expected of them. 22 Findings from this study reveal that poor organisation of teaching and learning exemplified by attending numerous redundant clinics, poor organisational logistics, and time constraints produced negative learning experiences during the CoBME placement and were all reported as ‘dislikes’ by the participants of this study (Table 1).
Logbooks are widely used in medical education as an evaluation tool to assess students’ progress towards objectives. 26 Numerous studies have reported on the use and value of logbook in medical education.27,28 However, some participants of this study stated that the logbook hindered student learning and might not be a true reflection of attained objectives (Table 1). According to Raghoebar-Krieger et al 26 and Patil and Lee 27 supervision and feedback and using logbooks as an interactive vehicle between students and tutors are important mechanism to foster student learning and optimise students’ use of logbooks. It is suggested that educators in the CoBME programme at BDH should make use of the aforementioned mechanism to foster meaningful learning with the use of logbooks during the CoBME training.
Although community-based teaching has many potential advantages, many important challenges also exist. 29 Findings by this study reveal that challenges faced by student during their CoBME posting in BDH were grouped under 11 themes. It has been reported that students’ perception of their learning environments impact on the way students cope in these learning environments and consequently affect their learning. 30 In this study, participants perceive their new learning environment as the utmost challenge faced during their CoBME training at BDH (14.2%) (Figure 2 and Table 2). This is in contrast to findings by O’Sullivan et al 22 who report that students perceive learning in the community to be more relaxed and easier to attain when compared with learning in the hospital/wards. It has been reported that learning in an environment with a high degree of variability of learning experiences at different community sites and with different preceptors are some of the challenges associated with learning in CoBME. 31 It is therefore possible that these are some of the realities faced by participants of this study. Some participants reported insufficient background medical knowledge as a challenge (5.2%), whereas others stated that coping with group dynamics was challenging for them (5.2%) (Table 2). Identifying insufficient background medical knowledge prior to entering the community-based placement as a challenge has been reported in the literature. 22 This has been attributed to possible passive learning experience, limited supervision, and lack of constructive feedbacks often associated with hospital-based training. 22 Therefore, it is possible that the participants in this study had encountered similar scenario during their hospital-based training. The negative challenges posed by ‘group dynamics among student’ were identified in a similar study by Cameron et al. 32 However, it was reported that students reached a better understanding when they realised that teamwork is beneficial as an important source of learning. 32 Hence, we propose that educators in the CoBME programme at BDH should enlighten student on the importance of teamwork/peer learning/team-based learning in their academic and professional career. Other reported challenges by the participants include: clinical practice context (12.6%), personal challenges (7.5%), and language barrier (7.2%) (Table 2). Although acknowledging that dealing with the numerous clinical problems that may present at primary care level (clinical context) may be challenging for students, it is expected that exposure to clinical work in these settings will help students gain a new perspective on the purpose of learning. 32 Ineffective communication or miscommunication between a health care provider and the patient can be life-threatening. 33 In a multilingual society such as South Africa (with 11 official languages), a major barrier to effective communication between a health care provider and the patient arises when both of them (ie, health care provider and patient) do not share the same first language. 34 In a study aimed at exploring communication curriculum and training at a medical school in KwaZulu-Natal, South Africa, Matthews and Van Wyk 35 reports on the perceived benefits of good communication and challenges posed by communication barriers in a medical programme. Matthews and Van Wyk 35 further opined that the incorporation of a socially accountable framework with an emphasis on language and cultural learning for the communicator role in a clinical context, into the curriculum, would contribute to a better preparation of graduates before immersion into the health system. It is therefore suggested that such framework as proposed by Matthews and colleagues be developed and incorporated into the undergraduate medical curriculum of the UFS.
Gomes and Golino 36 report that students’ self-reported perceptions on their academic processes are a type of metacognition: academic metacognitive knowledge. Performing a self-reflection on their own learning empowers learners and leads to students gaining increasing control over their learning. 37 In this study, participants were requested to do a self-reflection and give a self-reported perception in their own words, what they learnt during the CoBME training. Data presented in Table 3 suggest that participants responses can be discussed under 12 themes. According to Habbick and Leeder, 6 one of the major benefits of CoBME is to offer students a broader range of learning opportunities to acquire knowledge, skills, and attitudes. Similarly, participants of this study stated that they gained knowledge of how to perform certain clinical procedures and acquired core clinical skills in the areas of formulating management and managing some medical emergencies during their CoBME training at BDH (Table 3). In addition, promoting a more patient–orientated perspective and deepening the knowledge of the range of health and illness issues and the working of the health and social services have been reported as benefits of CoBME. 6 Hence, participants of this study reported gaining knowledge in the area of patient care, management of common disease, and operations of the the primary health care system (Table 3). Furthermore, participants reported gaining knowledge on the role of a general practitioner and family medicine practice (Table 3). This corroborates prior reports by Worley and Couper 4 which suggests that students can learn about general and family medicine during CoBME training. Finally, participants’ suggestions on how to further enrich students’ experience during the CoBME training at BDH revealed 9 core themes (Table 4). Increasing the duration of training had the highest percentage coverage (25.6%) suggesting that most of the statements given by the participants fall under this theme and that most of them advocate for increasing the duration of training at BDH. Other suggestions given include: improved organisation (10.4%), inclusion of formal educational programme in the training (8.4%), and improving doctors’ attitude (6.1%) (Table 4).
Study Limitation
Despite the valuable insights gained from this initiative, a limitation of this study is that it was conducted in a single setting. As a result, the outcomes of the study cannot be directly transferred or translated to experiences in other settings, ie, generalisability of the study. However, the instrument (Appendix 1) used to obtain data in our study can be utilised (subject to the needed modifications) as a simple tool to evaluate learning pogrammes in other settings in similar environments.
Conclusion
At present, CoBME is recognised as an important method available in medical education to foster medical knowledge and skills needed by medical graduates in the community. Programme evaluation is a valuable tool used by programme managers to strengthen the quality of their programmes and improve outcomes. 9 Obtaining students’ perception of learning, staffs’ teaching performance and programme appraisal are considered as approaches to programme impact evaluation. Findings from this study reveal that CoBME is a valuable pedagogical tool to enhance learning in undergraduate medical education. Participants of this study acknowledged the broader range of learning opportunities to acquire knowledge, skills and attitudes presented by CoBME at BDH. Students identified that they learned core clinical skills in delivering primary health care during their CoBME placement at BDH. Furthermore, this present study also identified that there is an urgent need for revising the operational, planning and logistics aspects of CoBME at BDH in order to address students’ dislikes and challenges faced during their CoBME training. It is our assumption that the findings from this study will inform future planning of the CoBME training programme in BDH.
Recommendations
Based on our experience and the findings from our study, we would recommend the following points to curricular developers and educators who are also engaged in improving the quality of CoBME programmes in resource-limited environments:
A planned orientation or student briefing programme should be presented on the first day of the CoBME training – this programme should include talks on the new learning environment, the different aspect of the CoBME training at BDH, working ethics, what is expected of the student/staff and a hospital tour.
Educators/supervising physicians should be encouraged to attend courses in leadership and management in medical education as part of staff development.
Formal teaching in the form mini-lectures/tutorials on relevant topics should be included as part of the CoBME training for the student.
Logbooks (preferably electronic) should be made more interactive to foster student learning and optimise students’ use of logbooks – logbooks can be designed to mirror the activities of the teaching and learning of the CoBME training. This should include bedside teaching, tutorials, and teaching at the clinics.
Educators/supervising physicians should constantly be trained on the effective use of logbooks.
Educators/supervising physician should make the clinic visit more engaging and academic in nature rather than monotonous – academic discussions should be held on presenting cases and management protocol.
Organisational logistics can be improved by making sure that all staff are constantly reminded of their roles and responsibilities.
Footnotes
Appendix 1
Acknowledgements
The researchers wish to thank all the year 4 MBChB students who participated in this study.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
MB conceptualised and supervised the execution of the study. AA collated and analysed the data and wrote the article. MB, AA, JB, and JOB reviewed the article. AA and JOB critically reviewed and provided final approval of the article.