
Abstract
As medical education has become increasingly globalised, universities across the world have sought to raise standards by partnering with well-established institutions and a number of different partnership models have emerged. This article describes an academic collaboration between University College London (UCL), UK, and Newgiza University (NGU), Egypt, to establish modern and innovative undergraduate medicine, dentistry, and pharmacy programmes delivered in Egypt. Academics from UCL and NGU co-developed programmes using established materials, assessments, and processes from the equivalent programmes at UCL. Dedicated project managers, regular steering group meetings, strong working relationships between project teams, and iterative curriculum and assessment development processes were important features of the success of this work. A multidisciplinary first semester included students across all 3 health care programmes. This promoted collaboration between academics at both institutions. Although UCL resources were the basis of this project, the different sociocultural, ethical, professional, and regulatory frameworks in Egypt have meant that a number of adaptations have been necessary, in both curricula and teaching content. Perhaps the most important factor underpinning the success of this project has been the mutual respect and sensitivity of academics and clinicians from both institutions.
Introduction
Although health care education has been radically professionalised in recent decades, the pace of change has varied widely, and as noted in a Lancet commission on global medical education, 1 there is still significant room for improvement in many parts of the world. Globalisation has had a profound impact on these changes. As health care workers have become more mobile, the transferability of their qualifications has become increasingly important, which in turn has led to a focus on standardisation and comparability.
A phenomenon that has emerged from this global interconnectedness is for newer universities to seek to raise their standards by partnering with well-established institutions, particularly those in the United States and United Kingdom. 2 These collaborations range from entirely franchised programmes delivered overseas through to joint degree programmes 3 to projects providing curriculum and faculty support. 4 Evaluations of such partnerships in medicine across a range of geographical regions have found that communication and cultural factors can be key barriers 5 to success. Similar findings have also been described in nursing education collaborations. 6
A literature review of educational cross-border curriculum partnerships found that the ‘copy-pasting’ of curricula from one institution to another was invariably destined for failure 7 and that a number of differences in clinical training make this particularly problematic. These include varied approaches to the clinician-patient relationship in different cultures, unique societal perspectives about traditional clinical care, and national legal and professional regulations that underpin clinical education and training. A subsequent study of 6 cross-border medical school partnerships used interviews with medical educators in the developing institutions and the ‘home’ school in Europe or North America. 8 It found broadly similar challenges arising from these partnerships, including differences in health care systems, legislation and political interference, teaching and learning environments, and collaborative working.
Reports of existing successful cross-border medical school partnerships include some noteworthy findings. For example, it has been found that personal commitment and engagement from senior leaders at the highest level is an important enabling factor 3 for the success of such projects. Challenges such as language barriers and differing ethnic traditions have led to the development of more personalised cultural competence programmes 9 and similar approaches have been used to customise ethics teaching. 10
Although reports of different relationships highlight particular benefits and challenges of their approaches, the existing literature mostly describes partnerships that involve joint degree programmes or overseas campuses, with comparatively fewer descriptions of collaborations that involve more autonomous and self-reliant new institutions being developed and supported through more collaborative and egalitarian partnerships with established overseas schools.
One example of a different type of collaboration between medical schools has emerged between institutions in Sub-Saharan Africa and those in the United States, Europe, and other high-income regions. The Medical Education Partnership Initiative (MEPI) was established in 2010 with the intention of strengthening medical education in Africa through a new approach to collaborations that overcomes the 1-sided nature of many partnerships. 11 A number of positive outcomes have been described from this project, including, notably, a strengthening of links among MEPI health science schools in Sub-Saharan Africa and the formation of a community of practice to continue the development of medical education in the region. 12
Needs Assessment
This article describes an international collaboration to establish modern and innovative undergraduate health care programmes in Egypt. The partners are from 2 countries with strong traditions in health care and health care education: the United Kingdom and Egypt. However, the UK partner, University College London (UCL), has been established for nearly 200 years, whereas the Egyptian partner, Newgiza University (NGU), is a newly formed institution, launching on a purpose-designed new campus in New Giza, Cairo.
Egypt has a long and proud tradition of excellence in health care, dating back to 2500
Newgiza University was established as a nonprofit private university established by Presidential Decree in April 2010. The founding faculties of this university are in Health Sciences. The stated vision of the NGU leadership is to establish programmes that inspire and educate a new generation of clinicians to move away from those structures and practices of traditional universities in the region that limit effective learning, and, instead planning to reduce class sizes, to focus on innovation and leadership and move away from a focus on didactic and theoretical teaching towards a more patient-centred and practice-focused model of education.
University College London is a leading global university based in the heart of London and consistently ranked as one of the world’s best universities. Founded in 1826 in the liberal tradition, it was the first university in England to welcome students of any class, religion, and the first to welcome women on equal terms with men. Health care education programmes are integrated, patient-focused, and aim to equip graduates to thrive in a constantly changing clinical landscape.
In 2016, NGU entered into an academic collaboration with UCL to access expertise and resources to support them in the development and delivery of their undergraduate medicine, pharmacy, and dental programmes. Senior faculty and staff from the UCL Medical, Dental, and Pharmacy Schools have been working with their NGU colleagues in strategic planning and organisation of the new programmes; setting up an appropriate infrastructure and education governance structure; developing curricula and learning resources; faculty and senior staff recruitment; faculty development; and education quality assurance.
Intervention
The activity in this collaboration falls into 3 overlapping phases. Phase 1 involved the necessary preparation and ground work to identify the necessary steps to establish the 3 undergraduate programmes. Phase 2 involved co-developing and embedding high-quality education and assessments for these programmes with NGU colleagues. Phase 3, which is currently underway, involves the ongoing development of the programmes and the Health Sciences School. These phases are underpinned by a contractual arrangement between the 2 institutions that takes the shape of work packages, which set the parameters and arrangements for each aspect of the collaboration.
Newgiza University launched its Medicine and Dentistry programmes in September 2016 and its Pharmacy programme in September 2017. Sharing a purpose-built campus, clinical facilities, and a cross-faculty Introductory Semester, the aims of the programmes are to produce distinctive NGU graduates who are scientifically literate, research-informed, patient-centred, and socially responsible professionals who can serve the health needs of individuals and communities both in Egypt and beyond. The overarching pedagogical principles of the 3 programmes, listed in Table 1, guide all decisions, development, and evaluation.
Educational approach in the new NGU programmes.

Abbreviation: IT, information technology; NGU, Newgiza University.
Outcomes
A key aspect of the collaboration has been the close working between academic and professional services staff at the 2 institutions. This has been maintained through regular face-to-face and virtual meetings to work on all aspects of the new programmes, from curriculum and learning materials to assessment and progression decisions. A steering group with key individuals from both institutions meets regularly to provide oversight of the new programmes and drive the collaboration forward. Importantly, both teams have project managers, who facilitate the operational elements of the work and are, for the most part, the single point of contact between the teams.
The interdisciplinary approach of this project has been an important feature of its success. Schools of Medicine, Dentistry, and Pharmacy from UCL have come together to support the new programmes at NGU, which has led to a strong interdisciplinary focus in the NGU health sciences faculty and NGU emergent programmes. This is demonstrated most notably in the joint Introductory Semester, a newly designed 18-week module that introduces students from all 3 disciplines to higher education learning in health care, with a focus on both academic and professional skills. The semester is built on a different theme for each 2-week block, anchored by a case study that is relevant to learning in all 3 disciplines and explored in small groups containing students from all 3 programmes. Faculty members from both institutions co-developed materials to ensure their relevance to all 3 disciplines; teachers are drawn from all 3 NGU faculties.
Individual programme teams identified areas of existing policy and curriculum that are specific to UCL’s regulatory and sociocultural setting and therefore not suitable for use at NGU. Here, new materials are co-designed by the teams. This may involve producing new materials de novo or more frequently, for the NGU team to edit existing UCL materials followed by one or more further exchanges until a functional version is created. This iterative approach allows teams to draw on each other’s skills and expertise, as well as recognise the rationale for decisions, thus allowing both teams to develop capacity and the newly composed NGU faculty to develop self-sufficiency beyond the collaboration.
Given the size and complexity of establishing new health care faculties and programmes, this collaboration faces a number of challenges (Table 2). Some of these are practical in nature, others pedagogical. The time and geographical differences between the 2 institutions requires team members to be flexible and tolerant in their working days. Although both institutions use English for all policy and teaching documents, Arabic is nonetheless the official language in Egypt and therefore some policy materials and conversations have required translations. Geopolitical unrest and security threats in Egypt have had to be taken into consideration when UK visitors have travelled to the NGU site, with risk management and information packs being used for all travellers. Finally, currency fluctuations between the British and Egyptian pound have meant that financial payments between the 2 institutions have had to be appropriately calibrated.
Challenges and solutions of collaborating institutions.
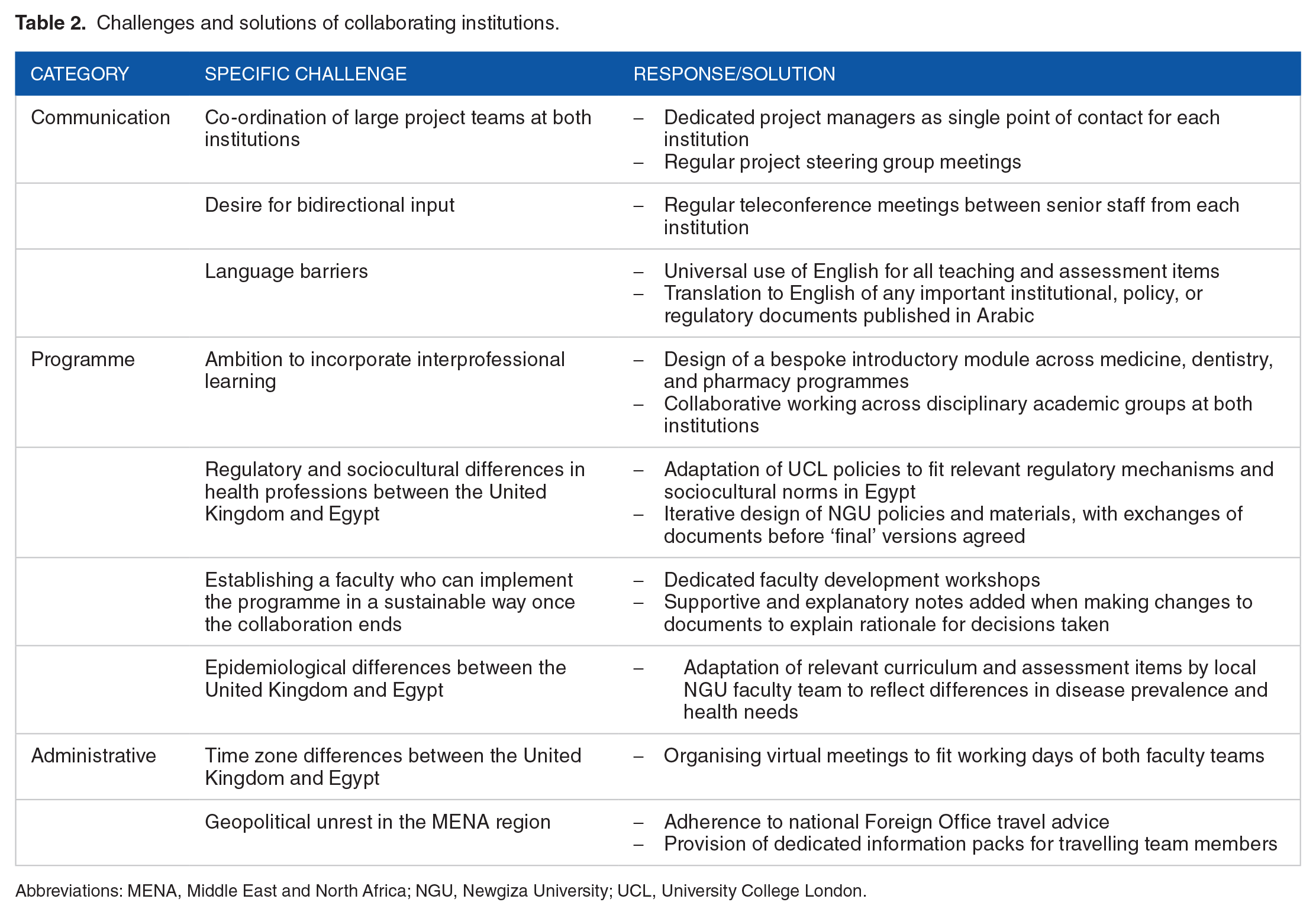
Abbreviations: MENA, Middle East and North Africa; NGU, Newgiza University; UCL, University College London.
From an academic perspective, the different sociocultural, ethical, and professional frameworks of the countries prove challenging when considering material co-development. The integrated nature of the programme means that even basic science learning includes a clinical focus. However, the different epidemiological burdens and health system structures of the 2 countries mean that the use of any existing UCL materials requires careful review to ensure authenticity.
More significantly, though, modern health care curricula include modules in communication skills, ethics and law, professionalism, and social and behavioural sciences. In all of these subjects, typically housed within the aforementioned vertical module structure, the teams work closely to ensure that subject content and pedagogical methods are culturally relevant to the Egyptian context. One area of notable challenge is the subject of professionalism. Whereas in the United Kingdom, the General Medical Council (GMC), General Dental Council (GDC), and General Pharmaceutical Council (GPhC) provide clearly published professional regulations and codes for health care students and professionals, the guidance in Egypt is less accessible, meaning that mirroring UK course materials with equivalent content proves especially challenging.
The approach in this project has undoubtedly been one underpinned by mutual respect and equality, and a recognition of the individual expertise and perspectives of all those involved. However, the differences in experience of the 2 institutions and the fact that the UCL team is financially remunerated for their involvement in the project have inevitably impacted the dynamic of the collaboration. Although the input has been bidirectional, the fundamental starting point for most project work has been to use the UCL approach, albeit in a modified way. Furthermore, individual academic and administrative staff from both teams have considerable experience, both in their current and past roles and institutions. Teams involved in introducing new ways of working are therefore sensitive to the previous experiences of individuals and are careful to provide appropriate justifications to explain the rationale behind new approaches. All team members have had to be vigilant around language, practices, and priorities. Although the core teams on each side quickly developed a shared understanding of this, wider connected teams can find this more challenging.
Conclusions
The academic collaboration between UCL and NGU has been stimulating, demanding, enlightening, constructive, and extremely satisfying for faculty members at both institutions. It has demonstrated the unique features of international collaborations and the enrichment that they bring to both partners, who are prompted to reflect on the important parallels and pluralities of the practice of medicine in different parts of the world. Academics from both institutions sought to build curricula that maximised on elements of the robust and well-established programme in London and yet recognised the important cultural distinctions of practice in Egypt. This endeavour proved to be illuminating for all involved.
With health care workforce shortages across most of the world, medical education is set to proliferate exponentially in the decades ahead and with the greater focus on quality that has emerged in recent years, cross-border partnerships look set to grow. The experiences of the academic collaboration between UCL and NGU can help other institutions plan how to maximise these partnerships and create a highly capable and enriched generation of health care professionals. In reflecting on the early experiences of this academic collaboration, we hope that others who are engaged, or planning to engage, in such partnerships can build on the strengths of our project and find ways to avoid and mitigate the challenges that we are facing.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are currently engaged in the UCL-NGU academic collaboration outlined in this paper.
Author Contributions
All authors contributed to the devising, drafting, and editing of this manuscript.