
Abstract
Objectives:
Hand hygiene is critical to patient safety, but low performance in terms of the quantity and quality of hand hygiene is often reported. Training-to-proficiency is common for other clinical skills, but no proficiency-based training program for hand hygiene has been reported in the literature. This study developed a proficiency-based training program to improve hand hygiene quality in line with World Health Organization (WHO) guidelines and assessed the amount of training required to reach proficiency. The training was delivered as part of a 5-day induction for students on the Physician Assistant online program.
Methods:
A total of 42 students used a simulator to objectively measure hand hygiene technique over a 5-day period. Proficiency was achieved when students demonstrated all 6 steps of the WHO technique in less than 42 seconds. The students also completed a postintervention questionnaire.
Results:
The average training episode lasted 2.5 minutes and consisted of 4.5 hand hygiene exercises. The average student completed 5 training episodes (1 per day) taking a total of 17 minutes. A total of 40% (17) of the students achieved proficiency within the 5 days. Proficiency was strongly correlated with the number of training exercises completed (r = 0.79, P < .001) and the total time spent training (r = 0.75, P < .001). Linear regression predicted that the 32 hand hygiene exercises or a total of 23-minute training were required to achieve proficiency.
Conclusions:
This is the first study to develop a train-to-proficiency program for hand hygiene quality and estimate the amount of training required. Given the importance of hand hygiene quality to preventing health care–associated infections (HAIs), medical education programs should consider using proficiency-based training in hand hygiene technique.
Keywords
Background
The World Health Organization (WHO) identifies hand hygiene as the “indicator of safety and quality of care delivered in any health-care setting.” 1 Health care–associated infections (HAIs) are a significant patient safety risk and cost to the health care system 2 and improved hand hygiene has been shown to significantly reduce the incidence of HAIs.3,4 The WHO guidelines recommend when hand hygiene should occur, ie, the “5 moments of hand hygiene” 5 and how hand hygiene should be performed, ie, the 6-step technique.3,6 This 6-step technique, shown in Figure 1, is critical to removing potentially lethal microbes from the hands.7,8
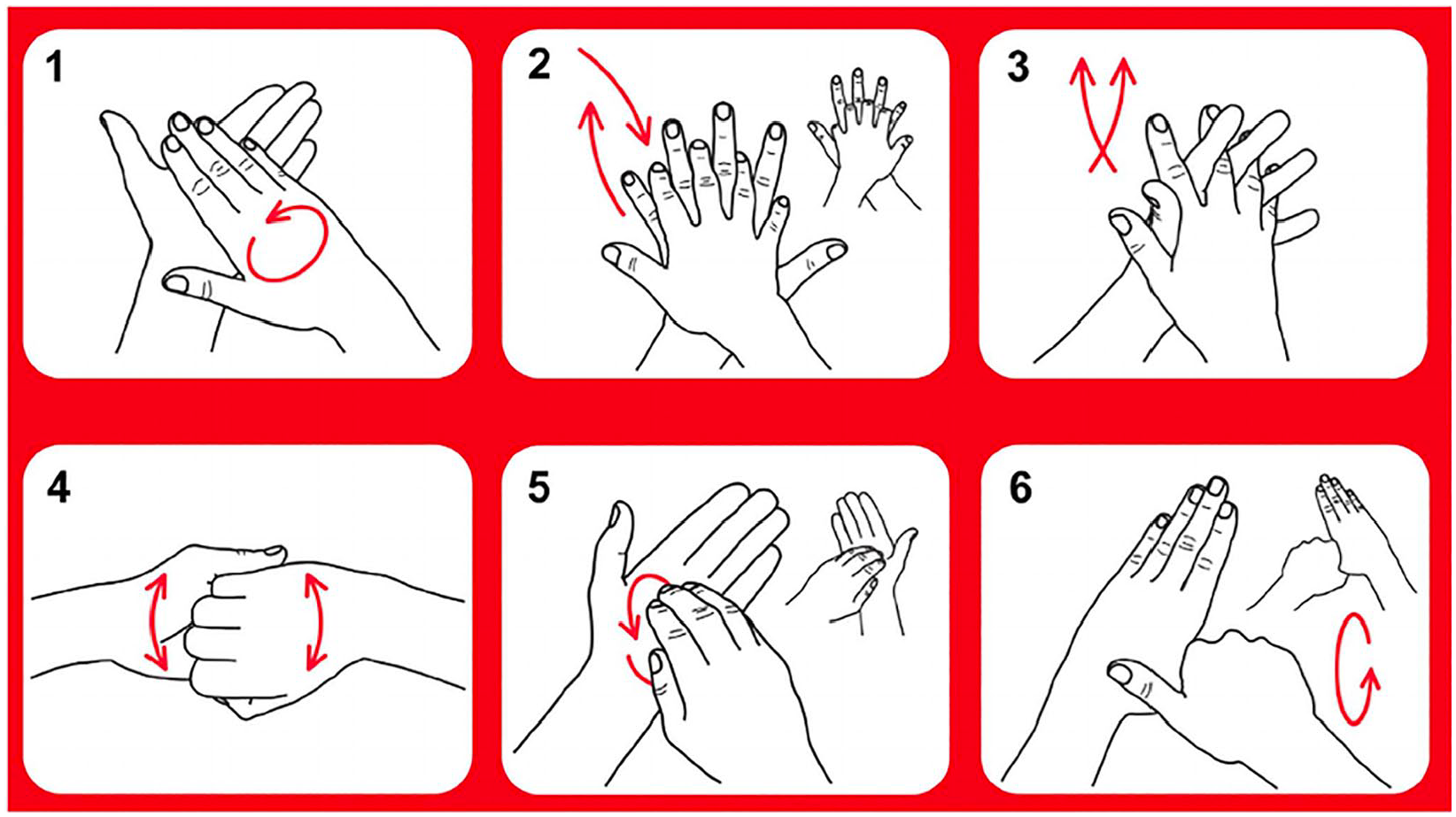
The 6 steps of the WHO hand hygiene technique. WHO indicates World Health Organization.
Despite the clinical importance of hand hygiene quality, use of the WHO technique has been reported to be as low as 8.5% in clinical practice. 9 The consequence is that health care workers’ (HCWs) hands are frequently contaminated with microbes that cause HAIs,10,11 even after practicing hand hygiene, albeit with poor technique.9,12 One major factor that contributes to poor quality hand hygiene is that hand hygiene is taught as mainly as conceptual knowledge rather than as a psychomotor skill such as other basic clinical skills, eg, suturing or catheter insertion.
Within medical education programs, infection control and surgical scrub are taught but clinical hand hygiene is typically not part of the curriculum. On clinical rotations, students are provided with a one-off induction sessions on hand hygiene but with few subsequent opportunities to practice hand hygiene with feedback. Classes sometimes use a UV fluorescent tracer to teach “coverage” of the hands, but Reilly et al 7 have shown that “coverage” is not correlated with a reduction in the microbial load on hands and therefore it does not have the construct validity to assess the quality of hand hygiene. This can give false confidence to learners that they can achieve hand asepsis using poor technique. In common with many basic clinical skills, the WHO technique is a psychomotor skill. These are taught in skills labs under the guidance of experts who provide feedback and provide multiple opportunities for repeated practice until learners reach proficiency. With these gaps in hand hygiene pedagogy, there should be little surprise that there is persistent underperformance during clinical practice.
We have known since the time of Morse code operators that repeated training is required to develop even simple skills and that practice without feedback limits a student’s ability to learn. Ericsson’s work on Deliberate Practice13,14 identifies that the key components for skills development are as follows:
A task with a well-defined goal;
Learners who are motivated to improve performance;
Access to immediate performance feedback on practice;
Access to ample opportunities for repetition and gradual performance improvement.
It is clear that traditional hand hygiene training does not meet Ericsson’s criteria.
Training-to-proficiency for medical technical skills15,16 has been shown to produce better results both in terms of skill level and retention.17-19 Although there are some variations due to task complexity, the literature also shows improved learning outcomes when training is distributed over multiple days with sleep intervals to consolidate the psychomotor patterns rather than so-called “massed training” which is short and intense. 20
This study developed a training-to-proficiency program for hand hygiene following the deliberate practice framework. We also measured how many training sessions were required to achieve proficiency. To address issues of implementation practicality, hand hygiene training was delivered within the context of a 5-day Yale Physician Assistant induction program. In line with the literature on duration and intensity, training was delivered as repeated short training sessions evenly spaced out over the 5 days, but students could complete additional self-directed training sessions at any time.
To deliver this program, a teacher could have provided one-on-one instruction and feedback to the students. This approach would have been labor intensive and critically it would have prevented subsequent self-directed learning. Taking example from skills training using surgical simulators, 21 we sought a hand hygiene training simulator that could measure speed and proficiency. We identified a simulator, originally developed by one of the authors, that uses video cameras and artificial intelligence to deliver hand hygiene training. This simulator has been validated in a number of studies22,23 which demonstrated that it constructs validity to measure hand hygiene technique and provides real-time feedback on a par with a human instructor.
Method
This study used a simulator shown in Figure 2, SureWash GO (Glanta, Ireland), to provide training and assess hand hygiene. The study measured the number of exercises and the duration of training required for students to achieve proficiency in the WHO hand hygiene technique. Proficiency was defined as an ability of learners to demonstrate accurately each of the 6 steps of the WHO hand hygiene technique from memory in less than 42 seconds. The 42 seconds upper limit was chosen as it allows 7 seconds per step. A longer time frame does not confer any microbiological advantage as alcohol gel can achieve asepsis in 15 to 20 seconds when good quality technique is used. 24
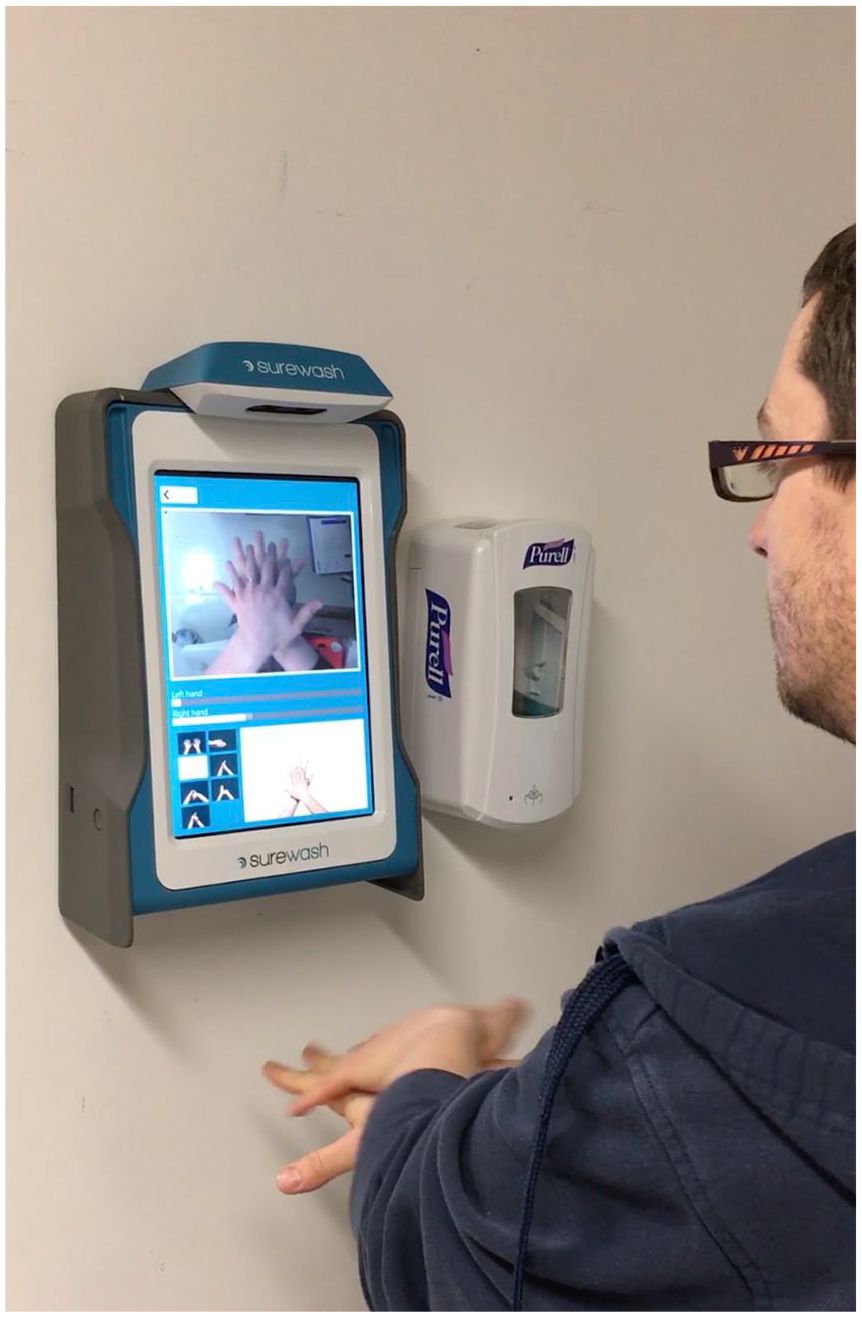
The SureWash GO simulator. The camera at the top of the unit measures the hand gestures and the feedback is provided via the screen.
Hand Hygiene technique instruction was divided into 6 levels of increasing complexity. The first level, Tutorial, broke the instruction into 6 separate steps of the WHO protocol via video instruction. Students imitated the video in view of the camera and received real-time on-screen feedback about their speed and accuracy for each step. During the Tutorial level, students could take as long as they wanted to complete the steps. In the subsequent levels 1 to 5, the steps were integrated into a smooth flow of gestures and there was a reduction in both the amount of instruction and the time allowed to demonstrate technique. At the final level, level 5, students were required to demonstrate from memory the 6 steps of the WHO hand hygiene technique in less than 42 seconds.
Results
Over the induction week, 42 students did a total of 795 hand hygiene training exercises on simulator. A training exercise is defined as one attempt at completing the WHO hand hygiene technique. On completion of each exercise, students got a score (% completeness and time taken) and this score drove some good-natured competition between the students. The number of training sessions, their duration, and the scores achieved were recorded for each student.
The average training episode consisted of 4.5 hand hygiene exercises and lasted 2 minutes 30 seconds. The average student did 5 training episodes, 1 per day, completed 20 hand hygiene exercises giving a total of 17-minute training. During the 5-day program, the students completed 12 hours and 27 minutes of individualized instruction in hand hygiene.
Detailed information was available on the different steps of hand hygiene technique that students found difficult. Figure 3 shows the overall pass rates for the different steps of hand hygiene and it is clear that fingertips and thumbs were the most challenging steps to learn.

The overall pass rates for each of the steps of the WHO protocol, showing that students took longer to learn the fingertip and thumb technique than the other steps. WHO indicates World Health Organization.
Not all students achieved the same level of proficiency by the end of the week. All students passed the tutorial level, but there was a drop off rate as the week progressed. The amount of hand hygiene training completed and the proficiency demonstrated by the students are summarized in Table 1.
The detailed results in hand hygiene proficiency achieved and the relationships with training time and the number of training sessions, 42 subjects, Yale, 2018.

Spearman rank Correlation between proficiency and number of sessions: r(40) = 0.79, P < .001. Spearman rank Correlation between proficiency and total training time: r(40) = 0.75, P < .001.
Table 1 shows a very strong correlation between the number training sessions and the proficiency level demonstrated. The average time and number of training sessions are shown in Table 1, but there was some variation in the time taken. The data from the 17 students who passed level 5 were used to build a linear regression model that can be used to predict the training needed by a typical student to demonstrate proficiency. This model showed that 23 minutes total of training time or 32 hand hygiene exercises, distributed over 5 days, was needed to demonstrate proficiency.
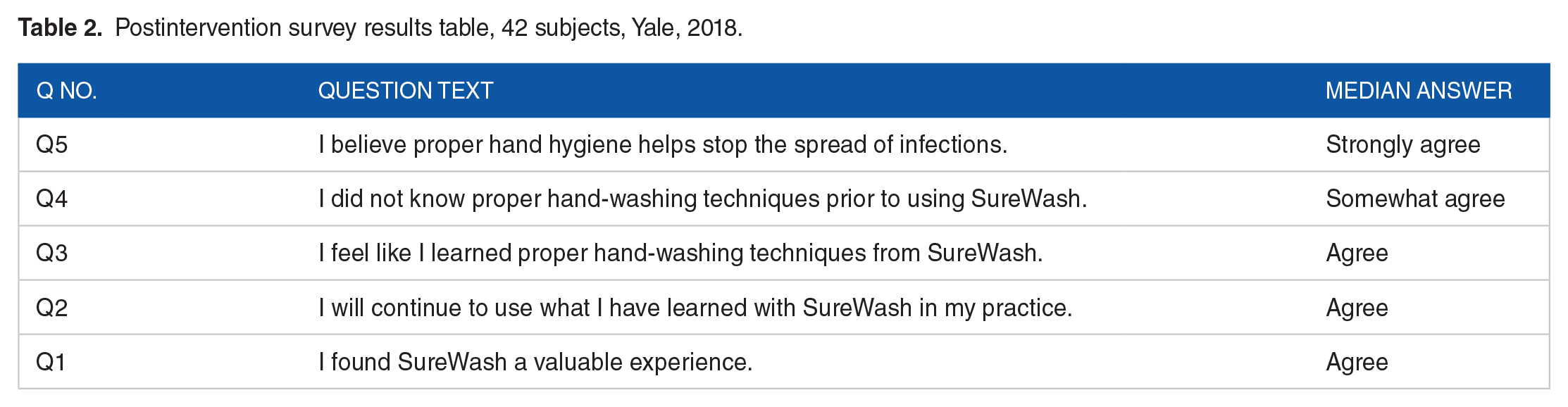
The students were also surveyed for their level of knowledge on hand hygiene before the training, their learning experience, and their intentions for applying what they learned (Table 2).
Postintervention survey results table, 42 subjects, Yale, 2018.
Conclusions
Our research reports on the first study to develop and evaluate a train-to-proficiency program for hand hygiene quality within a clinical education program. A strong correlation was shown between proficiency and the number of training exercises (r = 0.79, P < .001), and the total time spent training (r = 0.75, P < .001). Linear regression predicted that the average student took 32 hand hygiene exercises with feedback, delivered over 5 days, to achieve proficiency.
The primary limitations of our study are its scale (42 subjects) and its short duration, 5 days, which prevented us from determining the amount of practice required to train all students to proficiency. We did not assess the impact of different levels of manual dexterity, sex, or prior experience with hand hygiene. However, the results demonstrate that it takes multiple training sessions for learners to reach proficiency. This contrasts with the current training methods where a single hand hygiene class is provided. Our research results suggest that current approaches place an unrealistic expectation on HCWs to follow the WHO guidelines and that greater opportunities to practice with feedback should be provided. This could be achieved by the use of simulator or in lower resource settings via multiple peer-coaching sessions.
Our study has suggested that it takes 32 hand hygiene training sessions to achieve proficiency. However, given the results of studies comparing massed versus distributed training, spreading the sessions over more days is likely to reduce the total number of sessions required. Further study is required with a larger cohort and a longer duration to get a more accurate assessment. To improve the quality of hand hygiene in clinical practice, training programs should consider adding proficiency-based training to give HCWs the opportunity to learn microbiologically effective hand hygiene.
Footnotes
Acknowledgements
The authors would like to thank the students on the Yale Physician Assistant online program for their participation. We would also like to thank Physician Assistant Online Program faculty Stephanie Neary, Janie McDaniel and Associate Director, Jacqui Comshaw along with SureWash staff Sam Green and Jonathan Ruttle. The authors also acknowledge the loan of the simulator from Quinnipiac University.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding to support open access to this publication was provided by SureWash.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MS, JVR & GL jointly conceived and designed the study. ML and JVR ran the data capture for the study. GL performed the data analysis and jointly with ML drafted the main body of the paper. JVR provided editorial oversight on the drafts and analysis.