
Abstract
A community needs assessment and engagement activity was implemented in 2013 in the core preclinical curriculum as part of the doctoring course within Academic Communities at UC San Diego School of Medicine. This required educational experience included curricular learning objectives as well as goals to strengthen community service within academic communities. This activity was implemented and sustained within the academic communities with each community serving a different community of San Diego. Survey data from preclinical students from 2014 to 2017 consistently reported that the community assessment activity helped sustain or develop a service project in the academic community (67.1%-79.6% strongly agree or agree) and increased students’ knowledge of the needs in the assigned San Diego community (76.3%-80.6% strongly agree or agree). Students felt that the community assessment and engagement activity was a valuable learning experience (62.5%-77.8% strongly agree or agree). As a result of this educational intervention, 14 projects were implemented in the community. A subset of particularly interested and motivated medical students then took on leadership roles in these projects. Student-led scholarly assessment of the impact of some of these interventions resulted in 2 peer-reviewed publications thus far and 9 national presentations at the time of this publication. These assessments demonstrate not only educational impact, but health-system-level changes and meaningful change in patient outcomes.
Introduction
Learning communities (LCs) are intentionally created longitudinal groups designed to enhance students’ learning and experience.1,2 In medical education, these communities have been referred to with varying names including academic communities, houses, colleges, and societies.1,2 This educational structure has been implemented in part to address some of the fragmented traditional learning experiences in medical education. 3 In addition, LCs are part of a larger movement to decrease large lecture time in medical education and increase more interactive educational models based on adult learning. LCs facilitate a more personalized approach to teaching students how to become physicians through longitudinal relationships, role modeling, and mentoring.4–6 Students and faculty within LCs get to know each other well through small group learning experiences. This continuity and familiarity also often provides students with a safe space to speak with faculty members about any personal or professional issues that may arise. 2
Learning communities have existed in medical schools since the 1970s; however, it is only recently that they have become a common educational framework in medical education.1,2 The first national survey on LCs was conducted in 2006 and identified and described 18 LCs. 1 The most recent comprehensive national survey to describe the presence and characteristics of LCs in medical education in 2012 revealed 66 schools with LCs. 2 Subsequently, in 2014, the Liaison Committee on Medical Education (LCME) found that 72.9% (102/140) of schools assigned students to colleges or mentorship groups at some time during their education. 7 Although it is uncertain whether all of those 102 institutions integrate formal LCs, there is no doubt that this educational structure is becoming a standard part of undergraduate medical education.
Along with the growth of LCs in medical schools, there is an emerging literature on the impact of LCs in this setting. In a recent study of 28 medical schools, LCs were associated with the student perception of a more positive learning environment in the preclinical years. 8 LCs have also been associated with increased connections between students, improved student access to faculty, more comfort with clinical skills, and improved performance on third year clerkships.8–12
The most common issues addressed in LCs are medical student well-being, professionalism, career advising, mentoring, and social activities.2,13 LCs often serve a curricular function, although they may be solely extracurricular, and many institutions incorporate both curricular and extracurricular functions.1,2,13 For those medical schools that do have a curricular component to their LCs, it is common to teach clinical skills through the LCs.1,2,13 Although some LCs report addressing underserved medicine and service learning as part of their LCs, most of these are through voluntary involvement or are extracurricular. 2
In 2008, the LCME 14 implemented a requirement for medical schools to offer service-learning opportunities in the Standards for Accreditation of Medical Education Programs Leading to the MD Degree. Standard 6.6 states that “The faculty of a medical school ensure that the medical education program provides sufficient opportunities for, encourages, and supports medical student participation in service-learning and community service activities.” 14
Although there is often overlap or confusion with community service, service learning is a structured educational pedagogy that includes education, service, and reflection.15–18 Using the national data from the 2014-2015 Association of American Medical Colleges Curriculum Inventory (CI), it is observed that only 15% of schools (19/126) reported service learning in the curriculum. 16
Although 42% (22/53) of reporting LCs recently endorsed addressing service learning within LCs, the same number also endorsed addressing underserved or community medicine within LCs. 2 This indicates that there may not have been a separation of those institutions that performed solely community service from those performing a formal service-learning curriculum that includes not only service but also didactic and reflection components. The authors were unaware of any medical schools who had implemented formal service-learning pedagogy as a core component of the LC curriculum until attending the Learning Communities Institute (LCI) national conference in 2012. 19
At that conference, the University of Cincinnati presented as part of a small table discussion that each LC had been required to conduct a formal community assessment and service-learning activity as a core curricular component of their LCs. 19 Members of UC San Diego (UCSD) School of Medicine (SOM) Academic Communities (ACs) participated in this discussion and brought the idea back to our home institution. ACs were implemented as part of a larger preclinical curricular reform at UCSD SOM in 2010 and has been described previously.20–22 These communities serve both a curricular and an extracurricular function. Extracurricular functions since the inception of ACs at our institution have included advising, mentoring, community service, and student well-being. The curricular components include the longitudinal course taught within the AC structure including the preclinical doctoring course (called Practice of Medicine) and the third year Primary Care Core Clerkship, as well as the fourth year capstone course (called Principles to Practice). Each class of approximately 125 to 134 students is divided into 6 communities of approximately 20 to 22 students each year. Each class community is then further subdivided into 3 groups of 6 to 8 students for the longitudinal small group core course work. Although service-learning and community service was already a strength at UCSD SOM, with the UCSD Student-Run Free Clinic Project, student organizations, and AC-related service, none of these opportunities were required. Prior to the implementation of this project, there was not a place in the core curriculum for service learning nor a community assessment and engagement curriculum for all medical students.
This article will describe the process to design, implement, and assess the outcomes of a community assessment and community engagement service-learning educational component in the core curriculum as part of the doctoring course within LCs at UCSD SOM.
To the authors’ knowledge, this is the first publication describing community assessment and service learning as a core curricular component of LCs in medical education.
Methods
On return from the LCI national conference in 2012, a subcommittee of the doctoring course was formed to determine the structure, timing, and placement of this activity in the course. The committee was composed of doctoring Course Co-Directors, Academic Community Directors, and the Assistant Dean for Diversity and Community Partnerships. Over the summer of 2013, this team met several times and determined that these curricular components would consist of an introductory 50-minute lecture for all second year medical students on community assessment. The learning objectives for this activity were introduced in the lecture and are listed in Table 1. The students then broke into their 6 ACs of approximately 20 to 22 students per AC for small group sessions. During the 2-hour small group session, students learned about their assigned community and prepared for a visit to that community. During the third component of this activity, students then visited their community and met with stakeholders on site. Students and community members and leaders discussed community strengths and potential needs. Students were instructed to reflect on their session and prepare a final presentation for the final small group session. The final session conducted during dedicated class time is used for students to present their reflections, proposed course of action, and how they would like to measure outcomes. Students then implement their proposed service-learning project during non-class room time. Further involvement in the community service project is elective.
Learning objectives for University of California San Diego School of Medicine community assessment service-learning educational activity as part of academic communities.

In 2014, we developed a 10-item online survey to assess student perception of the educational value of this activity. The survey included identifying information (as student or faculty and which AC the participant belonged to) as well as 5-point Likert-type scale items, where 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. Three free text response boxes for comments included what participants found most valuable, least valuable, and what suggestions they have for next year’s community engagement. This survey was distributed to students electronically during the last required session of the community assessment or community engagement activity from 2014 to 2017.
The mean and SD of the 5-point Likert-type scale items were calculated each year. The percentages of those who agreed and strongly agreed were calculated. A formal assessment of free text responses was not conducted for this study. However, free text responses along with informal feedback from students revealed a strong preference to move the activity from second year into the first quarter of the first year of medical school to provide students with more time for longitudinal involvement. Therefore, this activity was conducted as a core part of the required second year curriculum in 2013 and 2014. Then, in response to student feedback, the curriculum was not only delivered to second year students in 2015, but also simultaneously delivered to first year students during a transitional year so that it could subsequently be delivered sustainably for all first year classes without skipping a class. It has remained in the first year curriculum since that time. An additional change over time includes that the initial community assessments were conducted based on a geographic area of San Diego and was later slightly modified to focus not only on a geographic area but to include specifically focusing on certain schools in those areas (largely high schools in underserved areas, but not exclusively).
We recorded the service projects implemented as a result of this educational intervention and the scholarly activity that resulted from those programs.
Results
The survey response rate was 85% (121/143) in 2014, 56% (159/285) in 2015 (the year in which both first and second year students participated in this activity), 77% (117/152) in 2016, and 68% (92/136) in 2017.
Educational outcomes
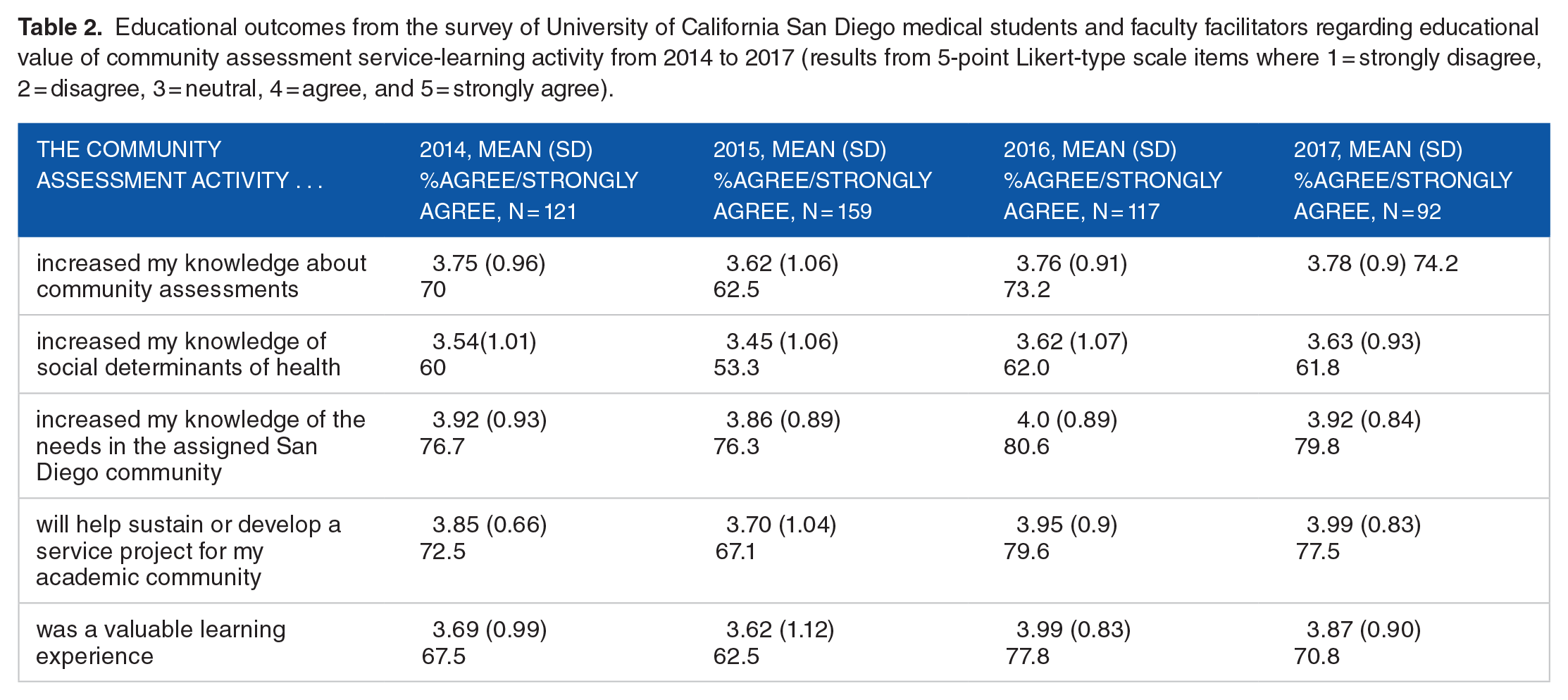
Students and faculty felt that this educational activity increased their knowledge of the San Diego community, helped sustain service projects, increased their knowledge, increased their knowledge of social determinants of health, and was a valuable educational experience (Table 2). The survey item with the highest mean on the 5-point Likert-type scale was “The community assessment activity increased my knowledge of the needs in the assigned San Diego community” with a mean ranging from 3.86 (SD = 0.89) to 4.0 (SD = 0.89), with 76.3% to 80.6% of participants agreeing or strongly agreeing with this statement throughout the study period. The second highest means were seen on the survey item “The community assessment activity will help sustain or develop a service project for my academic community” with the mean ranging from 3.70 (SD = 1.04) to 3.99 (SD = 0.83), with 67.1% to 79.6% of students agreeing or strongly agreeing with this statement. Most students (62.5% to 77.8%) felt that this was a valuable educational activity, with the mean ranging from 3.62 (SD = 1.12) to 3.99 (SD = 0.83).
Educational outcomes from the survey of University of California San Diego medical students and faculty facilitators regarding educational value of community assessment service-learning activity from 2014 to 2017 (results from 5-point Likert-type scale items where 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree).
Service outcomes
Each AC identified meaningful service-learning-related opportunities and 14 projects were implemented (Table 3). These projects included 1-time activities such as serving meals to the underserved, educational events, sports physicals, and screening of an Academy Award winning documentary film with the subject of the movie present to facilitate discussions about her experience with homelessness in San Diego. In addition, medical students created recurring activities such as fundraising, health education activities, and flu shot clinics. Students also created and implemented longitudinal activities including advising, and mentorship programs as well as hot spotting programs for high utilizers of the health care system.
Service outcomes from community service projects related to community assessment service-learning activity at University of California San Diego School of Medicine from 2014 to 2017.

Abbreviation: UCSD, University of California San Diego.
One of the most impactful activities to come out of the service-learning projects embedded in our LCs was the identification by medical students that San Diego had the lowest Supplemental and Nutritional Assistance Program (SNAP) enrollment rates of any large city in the country. They reached out to San Diego Hunger Coalition and Feeding San Diego and created a partnership that allowed for San Diego County to pilot then fully implement a same-day enrollment SNAP project for high-risk populations (such as people experiencing homelessness and mixed documentation status families). 23 This partnership also resulted in a long-term collaboration between these organizations and our Student-Run Free Clinic Projects, where Feeding San Diego now provides a food pantry that allows us to provide nutritious food to all of our patients during their clinic visits.24,25 This also led to a student-initiated randomized controlled trial in patients with diabetes documenting that food pantry services on site at free clinics resulted in not only decreased household level food insecurity, but also decreased depression, diabetes distress, increased fruit and vegetable intake, and improved glycemic control. 26
Scholarly activity outcomes
Medical students have collaborated with faculty and pre-medical student volunteers to conduct a systematic investigation of the impact of some of these projects that include not only educational impact but also health-system-level impact and patient outcomes. At the time, at least 11 scholarly activity products have been created as a direct result of this educational intervention and its subsequent service-learning initiatives, including 2 publications in peer-reviewed journals and 9 national presentations.
Discussion
Learning communities have been traditionally focused on student wellness, professionalism, clinical skills, advising, and mentoring.1,2 This study demonstrates that LCs can also be used to implement meaningful service learning as part of the core curriculum. Specifically, at UCSD SOM, we were able to implement a community assessment and subsequent community engagement activity that led was sustained over the course of several years.
Integrating service learning as part of the core curriculum within LCs was well received by the students and faculty. Most participants felt that this was a valuable educational experience, with 63% to 78% agreeing or strongly agreeing with this statement over the course of this study. Notably, the survey item with the highest mean score on the 5-point Likert-type scale demonstrated that participants felt this increased their knowledge of the San Diego community. This service-learning project was specifically designed to get students off the university campus, which is in a very affluent area of San Diego, into other areas of the community which they are unlikely to visit during their time in San Diego. The survey item with the second highest mean score documents that participants felt this activity helped sustain a service project implemented by their predecessors. If this educational component was elective, it is possible that it would not be sustained at the same level year after year.
There have been many national presentations and publications in peer-reviewed journals as a result of this work.24–33 Several graduation awards have been given to students who have implemented service projects during this educational activity and continued to expand the project, take ownership, lead, and study outcomes. This includes awards given for outstanding community service projects and outstanding scientific research.
We would like to acknowledge that it is not common for service-learning projects to evolve into activities that change county policies, provide hundreds of thousands of dollars of food donated to patients in free clinics, nor that they result in randomized controlled trials, graduation awards, or multiple peer-reviewed published articles. However, this study is an example of what is possible when medical students are encouraged to explore their community, speak with stakeholders, and assess what they may contribute to make a difference.
Our students recite the Hippocratic Oath as we welcome them to medical school during the white coat ceremony. The first line of the revised Geneva version states, “As a member of the profession of medicine, I solemnly pledge to dedicate my life in the service of humanity.” 34 The placement of this service activity in the first quarter of the first year of medical school allows them the opportunity to explore what service in medicine may mean to them. Preclinical students are often immersed in text books, lectures, and examinations for much of their first years in medicine. This activity is a part of the broader emphasis we hope to provide regarding the noble history and traditions of medicine that embrace and value service to others.
This study has several limitations. It was conducted at 1 institution; therefore, the results may not be generalizable. However, it was conducted and facilitated by several different lead faculty members over the course of multiple academic years, with different cohorts of students. Each community assessment or engagement focused on many different projects and evolved over time as the community needs changed. When working with communities, it may be important to address the concern of ethical issues of limited involvement and minimal impact as medical students are somewhat constrained in what they can contribute due to time and resources. This is an opportunity to integrate education about social determinants of health, structural violence, racism, classism, and bias. However, this can also be a very sensitive issue and needs to be addressed with thought. In addition, any medical school class will have students with very different levels of interest in this type of activity as students have mixed interest, background, and political beliefs.
Future directions for this project would be to find ways not only to sustain these projects but also to increase meaningful longitudinal projects as well as further assessment of impact on students as well as community members. In addition, we would encourage other medical schools to consider implementing structured service learning in their LCs.
In summary, service learning can be integrated into LCs within the core undergraduate medical education curriculum and result in meaningful education as well as meaningful service to the community.
Footnotes
Acknowledgements
The authors would like to thank the Dean’s office as well as the many staff, students, faculty and community members who make this work possible.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michelle Johnson was supported by NIH grant 1-R25 AT006574-04: Changing the culture of medical education through reflection and feedback.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors played key roles in the community engagement activity over multiple years. MJ collected and analyzed survey data and SS wrote the initial draft of the manuscript. All authors reviewed and revised the manuscript and approved the final version.