
Abstract
In total, 80% of clubfoot cases occur in low- and middle-income countries, where lack of clinical knowledge of the Ponseti method of treatment presents as a major barrier to treatment. This study aims to determine the effectiveness of an electronic learning course to teach clinicians in Tanzania Ponseti method theory. A total of 30 clinicians were recruited from clinics with high referral rates for clubfoot patients and invited to 1 of 3 training sites: Mbeya (n = 15), Zanzibar (n = 10), and Mwanza (n = 5). Baseline knowledge, measured through a pretest, was compared to performance on a posttest after e-learning course completion. Scores for Mbeya and Zanzibar participants improved from 44 ± 12.5 to 69.8 ± 16.5 (P < .0001) and 44.3 ± 14.0 to 67.9 ± 21.4 (P = .01), respectively. Our results suggest that an e-learning course may be an effective method of disseminating Ponseti method theory in Tanzania. Successful implementation requires an understanding of the device availability and technology literacy of the users.
Keywords
Introduction
Clubfoot (talipes equinovarus) is a congenital deformity affecting more than 200 000 children per year worldwide, with approximately 1 in 1000 live births being affected.1–3 Abnormal development of the tendons, muscles, and bones of the foot result in a downward (equinus) and inward pointing (varus) foot or feet at birth. Left untreated, children with clubfoot walk on the tops or sides of their feet, resulting in callous formation, potential skin and bone infections, and severe limitations in mobility, known as “neglected clubfoot.” 2 Neglected clubfoot causes lifelong disability, social isolation, and socioeconomic burden. 3
The goal of clubfoot treatment is to eliminate the foot deformity such that patients are pain-free, fully functional, and with upright feet that have good mobility and do not need to wear special shoes. 4 The Ponseti method is a low-cost, non-surgical, and effective method of treating clubfoot, and over the past decade, it has emerged as the standard of care for clubfoot treatment.2,5 In the Ponseti method, treatment begins within the first weeks of life with a series of gentle manipulations and casts. Casts are changed every 5 to 7 days, and the child’s foot usually attains a corrected position within 5 to 7 casts. Preceding the final cast, most children require a minor procedure called an Achilles tenotomy to provide full flexibility to the foot. The tenotomy can be performed under local anesthesia in an outpatient setting, and the patient can go home immediately to recover in their final cast. Following casting and the tenotomy, the corrected clubfoot is braced to prevent relapse. The feet are braced 23 h/d for the first 3 months, and, thereafter, at nighttime until the child is 4 years.
In total, 80% of clubfoot cases occur in low- and middle-income countries (LMIC), most of which do not receive treatment and therefore develop into neglected clubfoot.1,3,6 Lack of clinical knowledge of the Ponseti method presents as a major barrier to clubfoot treatment in LMIC.7–10 In many LMIC, there is no specific protocol for integration of clubfoot treatment into the medical education or health services systems. 10 Thus, clinicians in LMIC largely learn to treat clubfoot outside of their standard curriculum through weekend-long workshops led by visiting Ponseti experts, and there remains a deficit in the number of adequately trained personnel due to sporadic training opportunities.
Ponseti method training can be divided into 2 components: theory of the method and hands-on practice of the technique. Traditionally, the theory is taught as a full day of didactic lectures, and the hands-on technique is demonstrated through practice on plastic models and patients on the second training day. The existing training method requires a substantial amount of resources from international Ponseti organizations to host annual trainings in large regional hubs, making distribution of Ponseti knowledge to isolated rural clinicians difficult. To increase the number of clinicians clubfoot organizations can train, we created an electronic training (e-learning) course for Ponseti method theory. By shifting the Ponseti method theory to an e-learning course, the physical time requirements of trainers would be cut significantly, and in-person training can focus on skills acquisition of the Ponseti method technique.
Broadly defined, electronic learning (e-learning) is the use of the Internet, CD-ROMs, and other methods of media distribution to enhance learner knowledge and performance. 11 The concept of e-learning in medical education has been around for over 2 decades,12–15 and e-learning has since become ubiquitous among undergraduate, graduate, and continuing medical education programs, proving to be at least as effective as traditional teaching methods. 16 Success of an e-learning program depends highly on the extent to which the needs and concerns of stakeholders, including the learners and the instructors, are addressed. 11 In LMIC, such needs are well documented and include mode of access to materials, equipment, and training. 17 E-learning courses that take such needs into consideration throughout course design and implementation have achieved encouraging results in LMIC.18–22
In this article, we describe our experience using a blended learning approach to train clinicians in Tanzania to perform the Ponseti method of clubfoot treatment. Participants completed an e-learning course, developed by the authors, prior to attending a hands-on skills workshop. A pre and posttest were used to assess Ponseti method knowledge before and after the e-learning course, and a qualitative analysis, including a survey and guided interview, was used to assess the context-specific needs of the learners. We hypothesized that an e-learning course would be accessible to the participants of this study. We further hypothesized that completion of the e-learning course would improve the participants’ knowledge of Ponseti method theory.
Methods
Participants
A total of 30 clinicians (27% female) were included in this study using a convenience sampling method. Clinicians from clinics in Tanzania with high referral rates of clubfoot were invited to participate. All participants were clinicians who were involved in the care of patients with clubfoot and had not yet been trained in the Ponseti method. Clinicians included orthopedic surgeons, general practitioners, physical therapists, occupational therapists, nurses, and clinical officers (Table 1). The Institutional Review Boards (IRBs) or all participating entities have approved this study, and all participants were consented as per IRB guidelines.
Participant demographics, including gender, profession, device ownership, device type, and mode of Internet access.

E-learning Ponseti method training course
Course design
An online, modular Ponseti method training (e-learning) course was created by N.M.W. and S.D.V. in partnership with local experts in clubfoot treatment and medical education, a non-profit organization (NPO) involved in international training of clubfoot providers, and Ponseti method trainers in Tanzania. After an initial needs assessment in which the authors attended multiple international Ponseti method training courses, a prototype e-learning course was developed and beta tested. The Open edX platform was used for content creation and course delivery. Initial beta testers included local pediatric orthopedic surgeons and administrators in our partner NPO, who checked the course for accuracy of content. The course was subsequently tested in a group of 10 first-year medical students with no knowledge of clubfoot treatment who provided informal feedback on usability and ease of understanding course content. The in-country trainers then tested the course to ensure applicability to their use case and learner group. At each step, content and design were changed based on tester feedback.
Course content
The e-training course covered theory behind the Ponseti method. Course content was adapted from material found in the Clubfoot: Ponseti Management (3rd Edition) manual. 23 All course content was delivered in English. Course content was divided into several categories and subcategories, as summarized in Appendix 1. Each module had a mixture of text, figures (diagrams, images) or videos along with formative questions for the learner to test their understanding. Major categories for modules included “Diagnosis and Spectrum of Clubfoot Treatment,” “Pathoanatomy of Clubfoot,” “Pirani Scoring and Assessment,” “Ponseti Method Essentials,” “Foot Abduction Braces,” and “Common Errors.”
Pretest and posttest were included before and after the aforementioned modules, respectively. Each test comprised 23 questions, including multiple choice, true/false, fill in the blank, and drop-down menu questions. Questions with multiple components were weighted, and a total of 47 points were available. Score on the tests were scaled to fit a 0- to 100-point grading rubric.
Course delivery
The course was tested in Tanzania through a 3-site implementation. For Sites I and II, all learners accessed the course simultaneously at the same physical location. For Site III, learners accessed the course from separate locations at their convenience. At Site I, a 3G-enabled tablet was provided for users to access the course. At Site II, users accessed the course using their own devices on the hospital’s wireless Internet (Wi-Fi) connection. At Site III, users were neither provided a device nor Internet to access the course. The course could be accessed via laptop, tablet, or smartphone as long as Internet connection was available. In each site, participants completed the e-learning course along with a pretest and posttest to assess improvement. Access to course content, web browser, and study materials were restricted during administration of the pre and posttests at Sites I and II and for administration of the posttest in Site III. After completion of the posttest, participants were surveyed for qualitative feedback on their experience with the course. Completion of the e-learning course was followed by a hands-on skills training led by local Ponseti experts, including I.H.N., R.N., and E.S.K. Thus, this course provided asynchronous, individual, blended e-learning, which could be conducted at the same place or distributed. 11
Training sites
This study used a convenience sample based on availability of clinicians that met inclusion criteria at each of three different sites. All previously untrained providers involved in the treatment of clubfoot, as identified by in-country partners, were invited to participate in the training. Regional differences in population and medical provider density led to differences in sample sizes between participant groups. Assuming a sampling ratio of 0.5 (50% of available providers were identified, invited to, and completed the training), a sample size of 8 was retroactively calculated using mean test scores to achieve a power of 0.8 with a type I error rate of 0.05. 24
Site I—Mbeya
Participants (n = 15; 2 female) included 2 orthopedic surgeons, 7 physical therapists, 2 occupational therapists, and 4 clinical officers. They completed the course simultaneously as a group in a regional hospital conference room as day 1 of a 2-day training. All participants were provided 3G-enabled tablets to complete the course. The pretest was conducted prior to accessing the course content, and the posttest was conducted on day 1 immediately after completion of the online course. Day 2 of the training consisted of a skills training on models and patients, taught by local experts.
Site II—Zanzibar
Participants (n = 10; 3 female) included 2 orthopedic surgeons and 8 physical therapists. All participants completed the course simultaneously as a group in a regional hospital conference room as day 1 of a 2-day training. Participants were asked to bring their own device and used the hospital’s Internet to access the course. In total, 9 out of 10 participants used their own device, and 1 participant used a device provided by the hospital. A total of 5 participants used smartphones, 4 used laptops, and 1 used a tablet. The pretest was conducted prior to accessing the course, and the posttest was conducted day 1 immediately after completion of the online course. Again, the second day of training consisted of skills training on models and patients, taught by local experts.
Site III—Mwanza
Participants (n = 5; 3 female) included 1 general practitioner, 2 physical therapists, and 2 nurses. Due to greater prevalence of previously trained clinicians in Mwanza, less participants were eligible for the study at this site. Participants were given access to the course and asked to complete the pretest and coursework over a 2-week period prior to attending a 1-day hands-on training. To complete the course, 4 participants used a laptop, and 1 participant used a tablet. The devices were owned by the learner (n = 2), the hospital (n = 2), or a colleague (n = 1). A total of 3 participants used hospital Wi-Fi, 1 used 3G SIM data, and 1 used an Internet cafe. All participants completed the posttest in person at the beginning of the 1-day skills training in a regional hospital conference room.
Learner communication
Learners at Sites I and II completed the e-learning course in person and could communicate with other learners and trainers directly. Learners at Site III discussed the e-learning course content with trainers in person after completion of their posttest, which was given prior to their skills training day. Learners at all sites had access to an online forum through the course platform. Trainers received instructions on how to monitor for and respond to questions posted through the forum.
Qualitative feedback
Upon completion of the posttest, participants were asked to fill out a survey and participate in a focus group discussion. The survey and discussion allowed participants to provide qualitative feedback on their experience with this course. Topics discussed included course content, usability, challenges faced, and general opinions on e-learning.
Statistical analysis
A 2-tailed paired t-test was used to compare pretest and posttest performance for each study site. One-way analysis of variance (ANOVA) was calculated with StatPlus to compare both the average pretest scores and posttest scores among the 3 sites.
Results
Test scores
In Site I, performance from the pretest to the posttest improved significantly from 44.0 ± 12.5 to 69.8 ± 16.5 (P < .0001; Figure 1). In Site II, average performance improved significantly from 44.3 ± 14.0 on the pretest to 67.9 ± 21.4 on the posttest (P = .01; Figure 2). In Site III, there was no significant difference in average pretest and posttest scores (77.4 ± 19.6 vs 77.8 ± 9.6; P = .97; Figure 3). The average pretest scores varied significantly between the 3 study groups (P = .0004), but the average posttest scores did not vary significantly (P = .60).
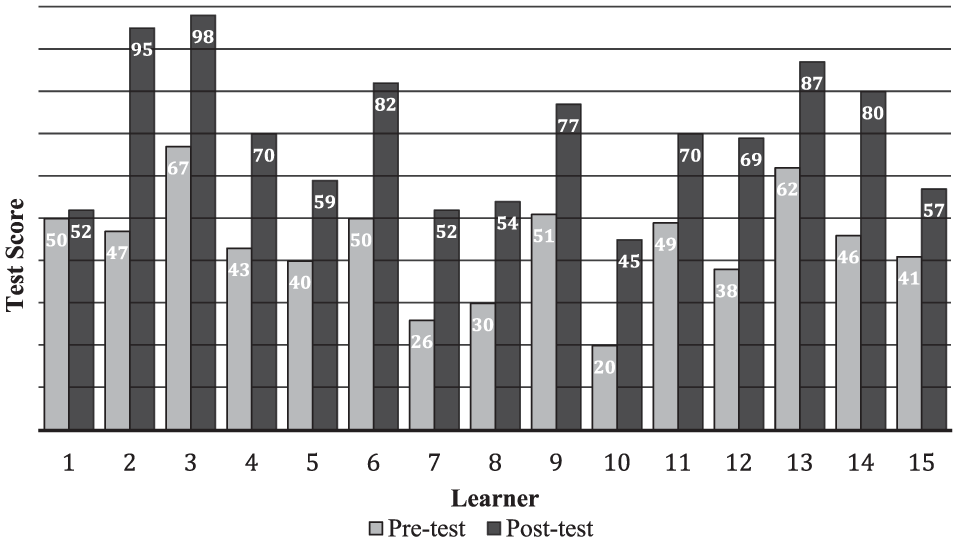
Site I—Mbeya: learner scores on pre and posttest assessments of Ponseti theory. Participants (n = 15; 2 female) included 2 orthopedic surgeons, 7 physical therapists, 2 occupational therapists, and 4 clinical officers. The pretest was conducted on-site prior to accessing the e-learning course, which was administered synchronously on-site. Learners used 3G-enabled tablets provided by the authors to access course content. The posttest was conducted immediately after completion of the e-learning course.

Site II—Zanzibar: learner scores on pre and posttest assessments of Ponseti theory. Participants (n = 10; 3 female) included 2 orthopedic surgeons and 8 physical therapists. The pretest was conducted on-site prior to accessing the e-learning course, which was administered synchronously on-site. Learners used their own devices to access course content. All participants used hospital Wi-Fi to access the Internet. The posttest was conducted immediately after completion of the e-learning course.

Site III—Mwanza: learner scores on pre and posttest assessments of Ponseti theory. Participants (n = 5; 3 female) included 1 general practitioner, 2 physical therapists, and 2 nurses. The pretest was conducted prior to accessing the e-learning course, asynchronously and off-site over the course of 2 weeks. Participants had simultaneous access to the pretest and the course content. Learners were asked to use their own devices and Internet connection. The posttest was conducted on-site and synchronously after completion of the e-learning course and prior to the start of the hands-on training.
Qualitative feedback
Participants reported that the course was “very clear, easy to navigate, and straight to the point.” The greatest strength reported was that the course was time efficient and could be completed at the user/participant’s own pace. Participants found the formative questions throughout the modules helpful in providing review and additional practice.
Participants reported certain limitations of the course. They did not think the videos embedded in some of the modules were practical due to connectivity limitations. Moreover, videos require a lot of data transfer and are thus more expensive when using a mobile device. In Site III, the main challenges reported with completing this training were Internet access and time. Participants in this group—as well as those from the other 2 sites—stated that the hospital Internet was sufficient to complete the course. However, Internet connection at home or elsewhere in their region was highly variable and generally poor. In addition, the participants in Site III reported that busy work days made it difficult for them to find the time to complete the course.
A total of 28 participants reported no prior experience with online trainings. After this training, 100% of participants responded that they “felt comfortable with online trainings” and stated that they would be willing to take an online training for a different clinical skill in the future. Most participants felt that the depth of the training was appropriate for their level of understanding. Furthermore, all participants reported feeling prepared for the hands-on training.
Discussion
Here, we describe our experience in implementing an electronic learning course for clinicians of various medical professions and diverse training backgrounds to teach the theory of the Ponseti method of clubfoot treatment. Participants at different sites either had both device and Internet provided, only Internet provided, or neither provided to complete the e-learning. All participants were able to access and complete the e-learning course. Most participants’ knowledge of the Ponseti method theory, as measured via performance on pre and posttraining assessments, increased after completing the e-learning modules.
In Sites I and II, the average posttest scores were significantly higher than the pretest scores, with all but one participant improving their score. The one participant that did not improve reported English literacy and computer literacy as notable barriers to navigating the course. Site III pretest scores were significantly higher than those in Site I or II. However, Site III posttest scores were not significantly different than those in Site I or II. One explanation for these results is that participants were instructed to take the pretest prior to completing the course, but they had access to course content and no time restriction while taking the pretest off-site. In contrast, they completed their posttest on-site with access to course modules blocked. Notably, there were misspellings of many words on the posttest that were spelled correctly on the pretest. Therefore, it is likely that the participants in Site III accessed course content or external resources while they completed the pretest. Given that posttest scores were similar between all groups, the posttest scores from Site III learners are likely the more accurate depiction of the learner’s knowledge.
E-learning: promising clinical education tool in low- and middle-income countries
The results from the 3 sites in Tanzania suggest that an e-learning course is a promising educational tool for teaching clinicians from varied educational backgrounds the theory behind the Ponseti method of clubfoot treatment. Given the shortage of clinicians trained in the Ponseti method in low- and middle-income countries, the local Ponseti method experts must divide their time between treating children with clubfoot and training other clinicians. By providing a standardized online course for the Ponseti method theory, learners may be taught standards of care without necessitating the time and physical presence of an expert. Learners may then attend a regional hands-on skills training day to learn the physical manipulation techniques under the guidance of an expert. This model allows for overall decreased time spent for training and increased flexibility in location of trainings.
Another strength of this educational tool is providing the learner flexibility to complete the course at their own time and pace. This is particularly helpful in settings where learners have varying levels of medical education, ranging from orthopedic surgeons to clinical officers, and varying levels of English proficiency.
Barriers to E-learning in low- and middle-income countries
The primary challenge with using an online training course in our setting was Internet connectivity. Although it is possible to circumvent this limitation through 3G-enabled tablets and hospital Internet access, Internet connectivity remains a barrier to learners who plan to take this course at home. In this study, 93% of learners reported personal ownership of a smartphone, and teaching learners how to access the course through their phone may be a viable strategy in the future. The 3 groups had drastically variable Internet connectivity, with Zanzibar having very reliable Internet and Mwanza having relatively poor Internet access. These differences are highly region specific and thus must be accounted for at each location. Registering for the e-learning course for distance learners was made possible through an in-country liaison that was briefly trained in technical support and interface troubleshooting.
Study limitations
A major limitation of this study was the small sample size, which limited our analysis. The clinician density and availability of providers who met the inclusion criteria varied widely between sites. At the completion of this study, every identified clinician actively working in Tanzanian clinics with high clubfoot referral rates at each site was either previously trained or included in this study. Future studies may expand to broader catchment sites either in more clinician dense areas of Tanzania or in other LMIC.
The findings of this study were potentially confounded by a number of factors. In this convenience sampling method of the 3 sites, groups were not controlled for demographics. Therefore, since all clinicians involved in clubfoot care who had not yet been trained in the Ponseti method were eligible to participate, group demographics varied widely from orthopedic surgeons to clinical officers. Without a control sample at each site, comparisons between the groups are limited. However, almost all participants improved their scores from pretest to posttest, highlighting the benefit of the course to clubfoot clinicians of all educational levels. A limitation specific to Site III was the inability to control access to modules and resources during the pretest. In Sites I and II, participants completed testing at the same time synchronously under observation of the training staff with restricted access to modules and other resources. As the participants in Site III completed their pretest asynchronously without supervision, we were unable to restrict use of external resources. However, their posttest scores—completed synchronously under supervision—were comparable with the other sites. Recent technical developments on our course platform will allow restrictions on access to the modules and question time limits for future iterations.
Translating knowledge to practice
An essential component in implementing and sustaining an educational tool of this nature in a low-resource setting is the local partnership. Our team included the design and development group at our home institution, administrators from our partner NPO, and local Tanzanian training coordinators and Ponseti method experts. This infrastructure was essential in developing a setting-appropriate product, connecting with target users, and implementing its use in country. Furthermore, the ecosystem in-place has allowed for continued development and delivery of this e-learning course past its initial implementation described here.
Although this study demonstrated that e-learning was a viable alternative to traditional classroom lectures for acquisition of clinical knowledge, further studies should expand on the findings reported here to assess knowledge retention, clinical skill competency, and translation of this knowledge to patient outcomes.
Conclusions
In conclusion, the use of an online training course for Ponseti method theory in Tanzania seems promising. Although Internet connectivity, device ownership, and English literacy were variable in our participant population, all participants were able to complete the course. Similar challenges have been reported by other e-learning trainings in LMIC and should not be a cause to avoid e-learning in such settings.18–22 Acquisition of technical skills required to perform the manipulations of the Ponseti method should still be achieved through clinical practice, which may be possibly obtained through blended learning. This model suggests that e-learning may serve as a prerequisite for an in-person training or hands-on skill session. Long-term efficacy of the training needs to be evaluated through repeat assessments as well as markers of proper care from patient records of the clinicians who underwent this training. This model of e-learning preparation prior to hands-on skills practice is promising not just for clubfoot, but for other skills-based learning topics in the future.
Footnotes
Appendix 1: Course Outline
Outline of the course material in sequential order. Included in parenthesis is the type of content found within each subcategory.
Acknowledgements
Mentorship for the development and implementation of the online training was provided by the Stanford d.school course Design for Extreme Affordability and the Social Entrepreneurship Laboratory jointly supported by the Stanford Graduate School of Business and the Stanford School of Engineering. The authors would like to acknowledge Jenna Leonardo and Seth Trudeau for their contributions to the needs assessment and development of the course content. The authors would also like to acknowledge the development teams at Raccoon Gang and Open edX, as well as Feroze Naina for their contributions to the development of the course platform. Finally, the authors would like to acknowledge the Global Clubfoot Initiative, CURE International, the Tanzania Clubfoot Care Organization, and Miraclefeet for their support throughout the design and testing of the e-training.
Funding:
Funding for authors SDV and NMW was provided by Social Entrepreneurship Laboratory Fellowships jointly supported by the Stanford Graduate School of Business and the Stanford School of Engineering. The funding body was not involved in the study design, data collection, analysis, interpretation, or manuscript preparation.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SDV and NMW conceived and designed the experiments. SDV, NMW, and SS analyzed the data. SDV and NMW wrote the first draft of the manuscript. SDV, NMW, IHN, RN, ESK, and SS contributed to the writing of the manuscript. SDV, NMW, IHN, RN, ESK, and SS agree with manuscript results and conclusions. SDV, NMW, IHN, and SS jointly developed the structure and arguments for the paper. SDV, NMW, IHN, RN, ESK, and SS made critical revisions and approved final version. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
This article is unique and not under consideration or published in any other publication. The Institutional Review Boards (IRB) or all participating entities have approved this study, and all participants were consented as per IRB guidelines. The authors have read and confirmed their agreement with the journal authorship and conflict of interest criteria. The authors have no conflicts of interest or disclosures to report.