
Abstract
We developed a multidisciplinary curriculum to improve our residents’ proficiency with smoking cessation counseling and prescribing of nicotine replacement therapy (NRT). The curriculum included a didactic portion, informational handouts, and a panel management component during which residents did telephone outreach and clinic in-reach to address high rates of smoking among patients. Residents rated their confidence with smoking cessation counseling and clinical knowledge before and after the intervention. We also tracked the number of patients flagged in the electronic medical record as smokers, the number of patients contacted, and the number of patients who received counseling. Although we did not make statistically significant improvements in perceived confidence with prescribing NRT, we found that there is an urgent need to address smoking cessation in the primary care setting and that working with a clinical pharmacist and psychologist offered a comprehensive approach. Furthermore, by anchoring the intervention with a population health component, almost 200 patients benefited from outreach efforts.
Background
Smoking represents the largest cause of preventable deaths and diseases in the United States and disproportionately affects those seeking care in publicly funded clinics and hospitals. 1 The Accreditation Council for Graduate Medical Education requires internal medicine residents to participate in panel management. 2 To simultaneously address both needs, we created an interdisciplinary smoking cessation curriculum to be used with our internal medicine residents working within a county clinic.
Numerous prior studies document inequities in smoking behaviors, showing higher smoking rates among persons with limited formal education and those living below the poverty line. 3 In addition to low socioeconomic status (SES) being linked to higher smoking rates, data also show poorer health outcomes for those who are low SES and smoke.3,4 Similarly, there are high rates of smoking in urban African American communities, which is particularly concerning as this minority subgroup demonstrates a higher incidence of lung cancer compared with their white and Hispanic counterparts.5,6 These inequities are of particular concern to our clinic, which is embedded in a county hospital and serves a low and under-insured population in Oakland, California. For the 2016 fiscal cycle, 22.7% of the clinic’s patients were enrolled in Medicare, whereas 60.8% were enrolled in Medi-Cal, California’s Medicaid program.
Prior studies have shown that motivational interviewing (MI), when used correctly, is a powerful tool that primary care physicians can use to help their patients quit smoking. 7 Furthermore, others have shown that MI can effectively be done over the phone and that there is a dose-related effect between MI and smoking cessation. 8
We identified a need to implement higher quality smoking cessation outreach efforts in our clinic and recognized this as an opportunity to teach our residents how to effectively use MI, prescribe nicotine replacement therapy (NRT), and use adjunctive pharmacologic therapy. We assembled an interprofessional team to create a curriculum for our residents that aimed to address these needs. We identified panel management—the processes by which patients assigned to a provider, clinic, or health system are targeted for interventions to improve their health—as a powerful strategy to improve our clinic’s rates of smoking cessation.
We implemented both outreach and in-reach strategies as part of this effort. Outreach refers to the processes in which patients who do not have clinic appointments are contacted (via phone, letter, text message, etc) to proactively intervene on their health, whereas in-reach refers to the processes by which patients who have clinic visits are approached about a predefined and unrelated intervention. We gave the residents protected panel management time to contact patients on their panels who had been identified as smokers and conduct phone outreach and asked residents to do in-reach to promote smoking cessation when conducting clinic visits with their patients.
Methods
Our intervention took place between January 9, 2017 and Mach 16, 2017 in a county hospital-based internal medicine residency program’s continuity clinic. We formed an interprofessional team, which included a clinical pharmacist, physician, and psychologist, who worked together to update the preclinic didactic curriculum on smoking cessation. The updated curriculum included new information on how to prescribe NRT—defined as nicotine-containing patches, gum, inhalers, and lozenges—as well as varenicline and bupropion. We also provided learners with information about what medications are covered using common formularies (Tables 1 and 2). Residents were also given resources on how to use MI tools. Particular emphasis was placed on the use of the “readiness ruler,” which allows the patient to express how ready he or she is to quit smoking and explore factors that are barriers and motivators to behavior change. The didactic content was taught in an interprofessional fashion by a physician and pharmacist to internal medicine residents during a half-hour preclinic conference. Residents were then given lists of patients in their panels who were flagged as smokers in the electronic medical record. Residents called their patients, confirmed smoking status, and engaged them in MI. If appropriate, the residents created cessation plans including NRT, other pharmacologic agents if appropriate, and/or referrals to our behavioral health team.
Formulary information for nicotine replacement therapy.
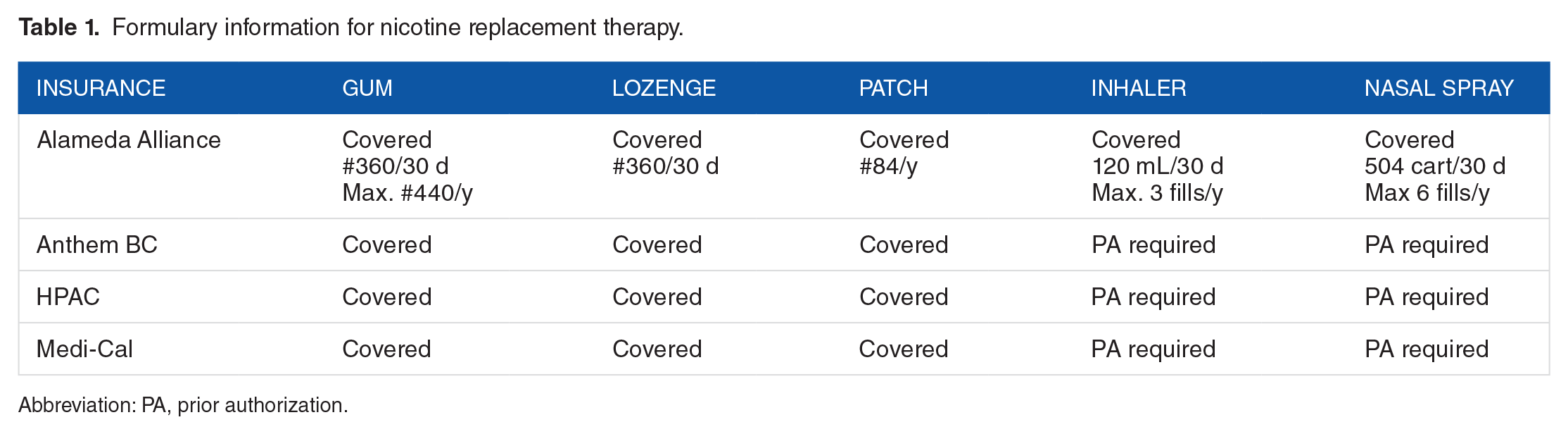
Abbreviation: PA, prior authorization.
Formulary information for varenicline and bupropion.

Abbreviation: PA, prior authorization.
Residents completed preintervention and postintervention surveys to assess their level of comfort with the activities. Surveys used entrustable professional activity language and asked residents to rate their level of comfort about prescribing NRT and MI on a scale ranging from “completely independent” (1) to “needing an attending present for the whole conversation” (4). We also collected data on the number of patients who received outreach, who were counseled about smoking cessation, whose residents were unable to contact.
Results
Residents documented conducting outreach with 194 patients, of which 153 received smoking cessation counseling, and 41 patients were unreachable. Of our 48 categorical and primary care residents, 44% (21 individuals) filled out the preintervention survey and 33% (16 individuals) completed the postintervention survey (Table 3). Independent-sample t tests were conducted to compare perceived independence and confidence about MI and NRT prescribing before and after the intervention. There was no significant difference in scores for any of our metrics (Table 4).
Survey participation.

Pretest and posttest survey data.
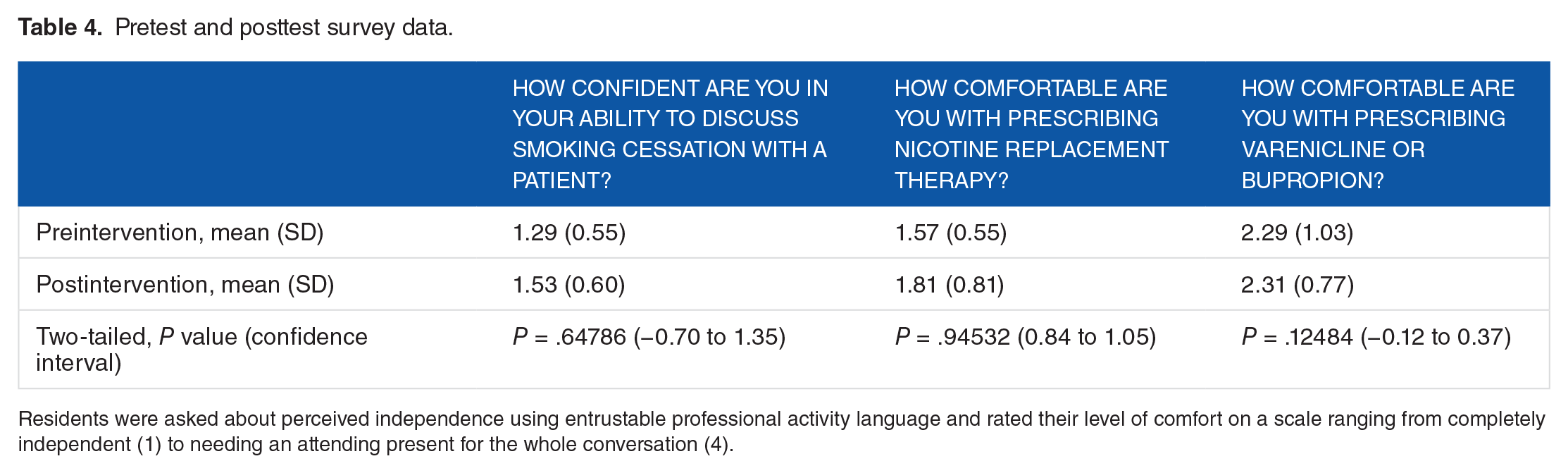
Residents were asked about perceived independence using entrustable professional activity language and rated their level of comfort on a scale ranging from completely independent (1) to needing an attending present for the whole conversation (4).
Discussion
Based on our preliminary data, many patients under the care of our residents need smoking cessation counseling. We also learned that residents need protected time to complete surveys and conduct outreach efforts to improve their patients’ rates of smoking cessation. Importantly, residents also need more formal training in the areas of MI and prescribing NRT, and using interprofessional teams containing content experts may be helpful. Although our intervention did not make a statistically significant impact in how comfortable residents felt counseling patients, prescribing NRT, or correctly prescribing varenicline or bupropion, this may be an artifact of our low survey response rate. Another limitation of our study is that, given the short length of follow-up time between intervention and data collection, we do not have data yet on the number of patients who have successfully quit smoking. Of note, however, the goal of the study was to assess feasibility of improving smoking cessation outreach efforts, which clearly were successful given the number of patients who were contacted. Factors such as limited time and provider discomfort in prescribing and getting NRT reimbursed often stymie primary care–based smoking cessation efforts. However, we learned from our pharmacy colleagues that prescribing NRT and other therapies is straightforward and is paid for by a variety of private and public payers. Despite the obvious shortcomings of our study, it should be stressed that 194 patients were contacted, and 153 received counseling about smoking cessation.
Conclusions
There is an urgent need for physicians to address smoking and related health needs. Tackling those needs may be less challenging than initially thought. By leveraging a multidisciplinary team to create a curriculum to improve our residents’ fund of knowledge around NRT prescribing and reinforced MI techniques to engage patients over the phone to create smoking cessation plans, we discovered that we could take more comprehensive, high-quality care of our patients who smoke. To make this intervention more robust, we plan on expanding our didactic session by making it longer, more interactive, and giving residents more protected time during which they will conduct supervised phone-based MI which will ensure real-time feedback regarding their communication and MI skills. We also hope to collect longitudinal data on smoking cessation rates before and after our intervention.
Footnotes
Acknowledgements
The authors thank Carima Smith, Blake Gregory, and Palav Babaria for their help with vision and implementation of the Panel Management program.
Peer review:
3 peer reviewers contributed to the peer review report. Reviewers reports totaled 531 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JKC contributed to curricular content development, manuscript creation, and data analysis; AB to literature search and manuscript editing; LL, DF, and LB to curricular content development and manuscript editing; and MA to data cleaning.
Disclosures and Ethics
As a requirement of publication, author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.