
Abstract
During a 1-year hospital-based residency, dental residents are required to rotate through many departments including surgery, medicine, and emergency medicine. It became apparent that there was a gap between clinical skills knowledge taught in dental school curriculum and skills required for hospital-based patient care. In response, a simulation-based intensive clinical skill “boot camp” was created. The boot camp provided an intensive, interactive 3-day session for the dental residents. During the 3 days, residents were introduced to medical knowledge and skills that were necessary for their inpatient hospital rotations but were lacking in traditional dental school curriculum. Effectiveness of the boot camp was assessed in terms of knowledge base and comfort through presession and postsession surveys. According to resident feedback, this intensive introduction for the dental residents improved their readiness for their inpatient hospital-based residency.
Introduction
Beginning in January 2007, New York State began requiring dental students to participate in a 1-year postdoctoral clinical dental residency program prior to applying for their initial licensure. 1 There are 2 possible general dentistry training programs: General Practice Residency (GPR), a hospital-based program, and Advanced Education in General Dentistry, an outpatient program. 1 The goal of the 2 programs was to expose the dental residents to a large pool of patients and give them the opportunity to learn from attending dentists and physicians. As of July 2013, Winthrop-University Hospital (WUH) accepted its first class of dental residents. The goal for WUH’s dental residency program was to gain advanced clinical experience and understanding of dental treatment plans for a culturally diverse patient population with a wide variety of medical problems. 2 During their residency, the dental residents rotate through many departments, including internal medicine, surgery, the operating room, anesthesia, and emergency medicine in addition to see patients in the dental clinical setting.
Analysis of course evaluations from the first 2 cohorts of residents revealed gaps in the student’s knowledge regarding clinical skills not covered in a traditional dental school curriculum. These clinical skills made it difficult for the dental residents to successfully navigate through all of their required rotations. In response, we created a multidisciplinary simulation-based curriculum consisting of didactic and practical sessions. The sessions were designed to help orient the residents to the inpatient hospital setting and introduce clinical skills relevant to their rotations.
To cover the vast amount of material, we developed a 3-day “boot camp” teaching a variety of topics, such as history and physical assessments, sterility techniques, note taking, clinical skills, dental emergencies, and communication and professionalism. We chose to teach it in WUH’s Simulation Center which allowed us to incorporate both high-fidelity and low-fidelity simulations. To determine whether the dental residents perceived the boot camp as relevant and helpful as part of their orientation, a survey of knowledge-based questions and comfort level was completed at the end of the 3-day course. The survey was used to assess the effectiveness of our teaching strategy and to determine whether the dental residents felt more comfortable beginning their inpatient rotations.
Methods
Curriculum design
A multidisciplinary collaboration was used to develop the boot camp curriculum which consisted of didactic and practical sessions. Using the flipped classroom model, we required the residents to complete the precourse work prior to the boot camp. The precourse work consisted of an online Electrocardiogram (EKG) review course from the American Heart Association, as well as online skill videos for medical history taking and medical emergencies in the dental office. The 3-day course was divided between hands-on skills, interactive lectures, and standardized patient scenarios (Table 1).
Three-day course outline.
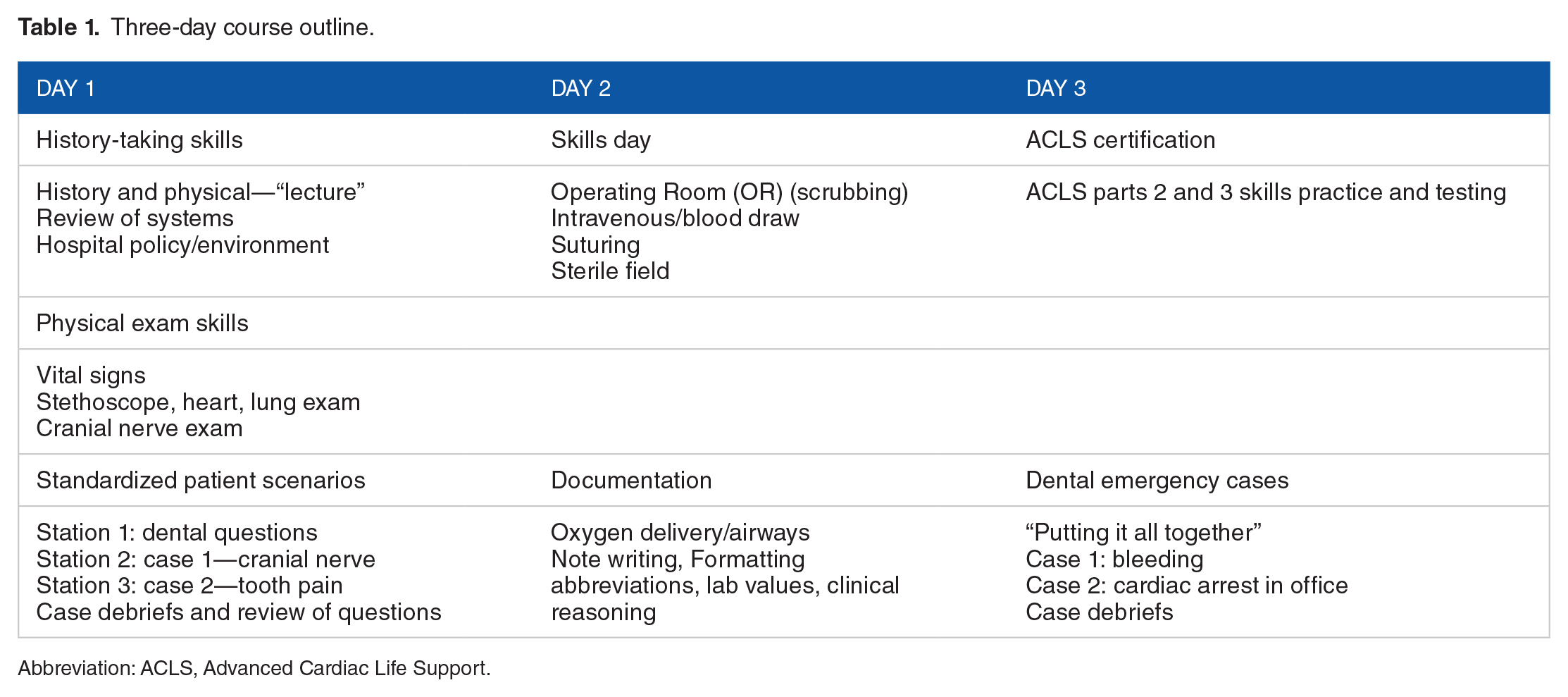
Abbreviation: ACLS, Advanced Cardiac Life Support.
The first day began with a discussion of the precourse videos and then proceeded to a didactic session on the elements of a history and physical, including discussion of the review of systems. Physical exam skills, including taking of vital signs, blood pressures, heart, and lung exams, were then discussed and practiced. A detailed review of the cranial nerves was also presented and practiced. The second part of the first day consisted of reviewing history and physical exam videos and discussing them. The dental residents “graded” the videos for completeness of the history and physicals. The dental residents also had the opportunity to practice history and physicals on standardized patients. The 2 standardized patient scenarios were based on patients seen by previous dental residents doing consults within the hospital. The objective of the case was for the residents to practice history and physicals with feedback provided by the standardized patients. After the cases, a group debriefing occurred to discuss each case from a medical perspective and to allow the residents to reflect on their experience.
The second day of the program was a skills day to learn scrubbing techniques for the operating room, general sterile and suturing techniques for facial trauma, and blood draws for their medicine rotations. Consult note writing, laboratory values, and medical abbreviations were also covered on the second day. During the final day of the program, the residents obtained their Advanced Cardiac Life Support (ACLS) certification and practiced using the high-fidelity mannequin for cases requiring them to use their ACLS knowledge.
Cases
A 75-year-old man with a past medical history of hypertension, hyperlipedemia, and coronary artery disease who presented to the emergency department with an acute onset of left hemiparesis of upper and lower extremities as well as dystharia. The patient was also 6 days after tooth extraction. While in the emergency department, the patient was diagnosed with an acute stroke and given tissue plasminogen activator (tPA). Approximately 2 hours after tPA was given, blood was noticed around patient’s mouth, and 6 hours later, patient was continuously bleeding from the mouth. The on-call dental resident was consulted by the neurological intensive care unit physician assistant to evaluate the patient.
A 50-year-old man with a past medical history of elevated cholesterol, hypothyroidism, and noninsulin-dependent diabetes mellitus who presented to the emergency department with complaint of right facial swelling and pain for 2 days. The standardized patient was complaining of throbbing in the right maxilla that radiated to his forehead.
A 60-year-old man with a past medical history of hypertension and diabetes presented to the dental office for a cavity filling. The patient becomes unresponsive while in the dental chair and goes into cardiac arrest.
After each scenario, a debriefing occurred to discuss the medical knowledge, actions taken, and the dental residents’ personal reactions to the cases.
Survey
Presession and postsession surveys were used to assess the effectiveness of the boot camp sessions. The goal of the survey was to determine whether the students improved their fundamental knowledge of basic medical issues and their comfort levels with certain clinical skills. Using a Likert scale, the residents were assessed for their confidence levels in patient history taking, stethoscope use, assessing lung sounds, laboratory value interpretation, and operating room scrubbing techniques. The residents were also tested on basic medical knowledge such as atrial fibrillation medication use, patients’ oxygen supplementation requirement, and correct intravenous catheter placement.
The Likert scale results from the presession and postsession surveys were compared to see whether there was a change in confidence level or knowledge level after participating in the boot camp.
Results
A total of 6 dental residents participated in the 2016 boot camp. The results were obtained from a voluntary anonymous institutional review board–approved survey prior at the start of the boot camp and on completion of the 3-day course. All the residents just completed their dental school requirements and were starting their GPR program. The residents were from 4 different dental schools.
The dental residents’ confidence scores increased in 4 out of 5 of the clinically relevant categories. The average Likert scale from the presession survey was 2.8, and the average on the postsession survey was 4.0. The categories included patient history taking, use of the stethoscope, assessing lung sounds, laboratory value interpretation, and operating room scrubbing techniques. The only score that did not increase was the comfort level regarding the stethoscope use (Figure 1).
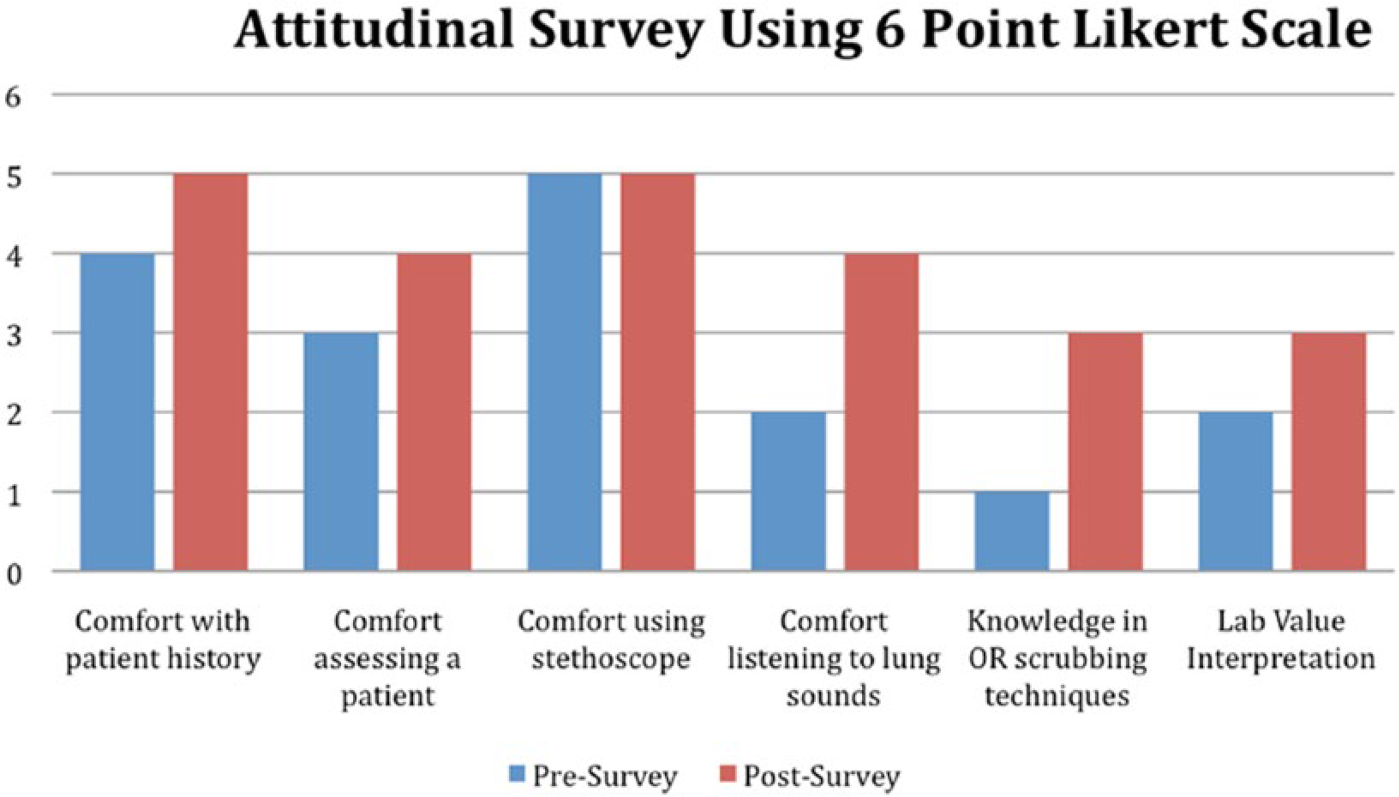
Confidence scores from pre- and postsession surveys.
The total number of correct answers for the knowledge-based questions from the pre- and postsurveys was also compared. There was a considerable increase in the number of correct answers after completing the boot camp. The number of correct answers on the presession survey was 55, whereas the number of correct answers on the postsession survey was 90 (Figure 2).
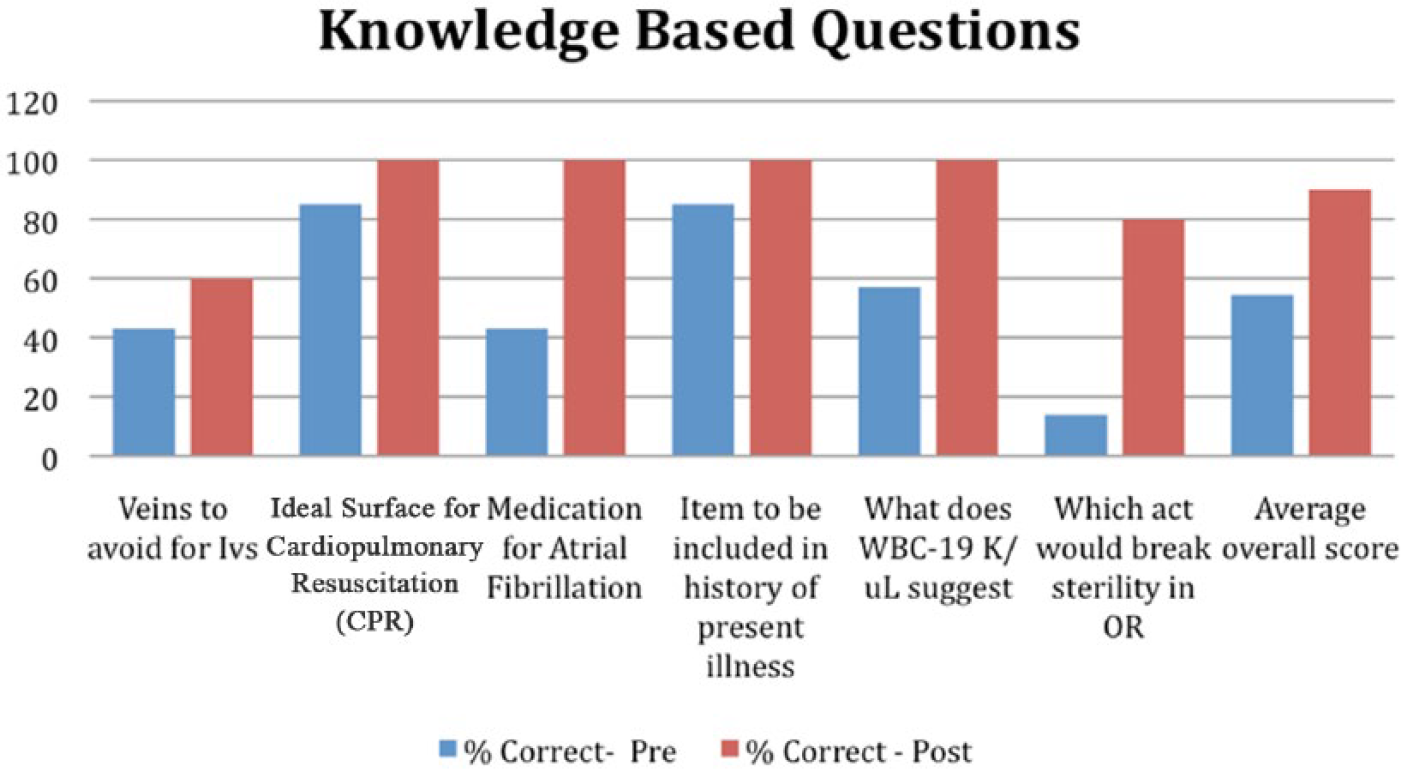
Number of correct answers from the pre- and postsession surveys. WBC indicates white blood cell.
Discussion
Simulation-based education has been regularly used to provide a safe, effective means of teaching medical students for many years. It is an alternative to the “See one, Do One, Teach One” model that is no longer considered acceptable due to the importance of patient safety and care. 3 Simulation-based learning is not a substitute for direct patient care; instead, it is an educational tool which uses aides, such as high-fidelity mannequins and standardized patients, to replicate clinical scenarios. 3 The use of this type of education has been underused by dental education. 4 Within dentistry, simulation has been used to aid in teaching oral surgery skills 5 and as a medical crisis simulation activity for dental residents and assistants. 6 However, as far as we are aware, simulation has not been used to orient new residents for the inpatient, hospital-based GPR year.
Our innovative dental resident boot camp was created after doing a needs assessment and realizing that the incoming dental residents were lacking clinical skills and knowledge not covered in the traditional dental school curriculum. The dental residents did not have much exposure to inpatient consultations or hospital-based rotations prior to their arrival for residency. The boot camp was designed to allow the residents to learn or review the basis of history and physicals and practice physical skills both relevant to dental cases and general medicine cases. The residents were introduced to hospital operations and the key players they will be working with while on rotations or doing consults. The residents were also taught sterile technique which is important during their rotation through the operating room and emergency medicine department. We allotted time for the residents to practice learned skills on standardized patients. These sessions helped to ensure proper discussion and evaluation of history and physicals prior to seeing patients on their own as consultants.
The results of the surveys taken by the residents were very encouraging. The assessment of their knowledge base increased by correctly answering almost double the questions after the boot camp compared with before the session. Also, possibly even more important, the dental residents’ confidence levels increased after taking the clinical skills boot camp. We received comments such as the “accuracy of simulation was high compared to real patients” and “efficient and risk-free simulation allowed me to become familiar with handling various situations” from the dental residents after completing the course. The confidence level regarding stethoscope use did not increase because new lung sounds, such as wheezing, were introduced during their practice session.
This study was limited by the numbers of residents who have completed the boot camp and survey. To determine any significant differences between the presession and postsession survey results, more residents need to be assessed. After completing 3 years of boot camps, we have a better idea of the particular skills the dental residents need to be familiar with prior to entering their rotations. The 2016 boot camp case scenarios were based on actual cases seen by prior dental residents, thus providing the residents with concrete examples of consultations and providing more relevancy to their education. Long-term studies, however, are necessary to evaluate the effectiveness of the boot camp in knowledge retention and relevancy to general dental practice after completion of the residency program.
Conclusions
Dental residents starting their inpatient hospital-based residencies were found to have difficulties during their rotations leading to the development of a simulation-based clinical skills boot camp. This program provided both didactic and practical sessions allowing the residents to improve both their skill confidence levels and knowledge base. Having more confident and skilled dental residents will only improve patient care and ultimately help dental residents to successful complete their year of residency.
Footnotes
Acknowledgements
The authors would like to acknowledge Ms Colleen Acevedo for her assistance in coordinating the boot camp.
Peer Review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 999 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JC, KA, JK, PJ, ZM, and JS conceived and designed the experiments and made critical revisions and approved the final version. JC analyzed the data and wrote the first draft of the manuscript. JC, JK, and JS contributed to the writing of the manuscript and jointly developed the structure and arguments for the paper. JC, KA, JK, PJ, and ZM agree with manuscript results and conclusions. All authors reviewed and approved the final manuscript.