
Abstract
Highlights
A patient decision aid (PtDA) was developed to support individuals with head and neck cancer in deciding whether to participate in a proton radiotherapy trial.
The PtDA was developed through an iterative, theory-informed, and user-centered process with input from clinicians and trial-eligible patients.
The PtDA provides structured, balanced information and explicit comparisons between standard photon radiotherapy and the trial option.
This development approach may be adapted to support decision making in other radiotherapy trials and clinical trial contexts.

Keywords
Clinical cancer research is essential for developing new treatments to improve patient care and quality of life.1–3 Approximately 8% of cancer patients in the United States participate in clinical trials, and this low participation rate is attributed to multiple barriers.4,5 In Denmark, the Danish Head and Neck Cancer Study Group (DAHANCA) has set an ambitious goal of designing relevant clinical trials that would enable up to 50% of Danish patients with head and neck cancer to participate. 6 Structural barriers include logistical challenges, for example, geographic distance to experimental treatment facilities.7–12 Systemic barriers include strict eligibility criteria and organizational inefficiencies that complicate recruitment and research processes.3,13,14 Physician-related barriers include limited awareness of ongoing trials and selective patient invitation, sometimes influenced by clinicians’ personal attitudes toward a specific trial or the treatment under investigation.15–19 Patient-related barriers include low health literacy, financial concerns, anxiety about randomization, and mistrust of experimental treatments.20–23
Information, communication, deliberation, and decision making regarding participation in clinical trials often occur concurrently with decisions about active cancer treatment. This creates a complex and ethically challenging context for patients, who may experience emotional distress related to the cancer diagnosis, and for health care professionals (HCPs), who must balance the standard care trajectory with the trial opportunity.3–5,19,23
Informed consent in clinical trials is based on the principles outlined in the World Health Organization’s Good Clinical Practice guidelines and the Declaration of Helsinki, which emphasize the ethical obligation to provide patients with clear and sufficient information to support an informed decision about trial participation.24–26 Patient information leaflets (PILs) are standard tools for communicating trial information and are required to comply with these principles.24–26
PILs describe study treatments and potential risks but do not provide balanced comparisons of the study treatment versus standard care, incorporate elements such as values clarification or structured decision guidance, or often pay insufficient attention to health literacy. 27 Hence, when assessed against the International Patient Decision Aid Standards (IPDAS), PILs typically fall short of supporting clinical trial decision making.28,29
Prior research demonstrates that information provision alone does not adequately support informed, value-based decisions, as patients often require additional decision support to clarify values and deliberate among options.30–32 These include recognizing trial participation as a treatment decision alongside standard care, understanding randomization and clinical equipoise, and weighing logistical challenges, such as distance to the study treatment and potential treatment delay, against personal values.17,23,28,32–34
Patient decision aids (PtDAs) are resources designed to support people in making reasoned decisions between 2 or more options.30,31 Research indicates that PtDAs designed to support clinical trial decision making can improve patients’ knowledge and preparedness, and some studies also show reductions in decisional conflict. In contrast, effects on values, clarity, and decisional regret are less consistent.17,35–41 As the evidence for clinical trial PtDAs remains limited, further development and refinement are warranted. This article reports the development of a PtDA for use in the DAHANCA 35 proton radiotherapy trial. In this article, the methods used to scope, develop, and alpha-test PtDA with multiple users are described.42–45
Methods
Context
The Danish Head and Neck Cancer Study Group, DAHANCA, is a Danish multidisciplinary study group dedicated to enhancing treatment outcomes for patients with head and neck cancer. DAHANCA is responsible for organizing and conducting clinical trials across Danish cancer centers that diagnose and treat patients with head and neck cancer. The research teams comprise clinicians from oncology departments who also serve as clinical trialists. 6 This study used an ongoing clinical trial (DAHANCA 35) as a development case for designing a clinical trial PtDA prototype. DAHANCA 35 is a randomized controlled trial (RCT) comparing proton versus photon radiotherapy for patients with pharyngeal and laryngeal cancer, with long-term side effects as primary endpoints. 46 Proton therapy aims to reduce long-term toxicities of treatment by limiting irradiation to surrounding healthy tissues. 47 Participant enrolment in DAHANCA 35 began in 2020 and is expected to conclude in 2027.
In Denmark, standard photon radiotherapy is provided at 6 regional hospitals. In contrast, proton therapy is available only at the Danish Centre for Particle Therapy at Aarhus University Hospital, Aarhus, Denmark. Patients consenting to DAHANCA 35 who are allocated to the proton therapy arm must travel up to 350 km to this centralized facility, with local accommodation provided for those living far from the center.
Patients receive verbal information about DAHANCA 35 during a clinical encounter at 1 of the 6 Danish regional hospitals, where the mandatory PIL is also provided. In this consultation, physicians first present the standard treatment options. While surgery may be relevant for some patients, radiotherapy is the primary treatment for most. The standard of care with photon radiotherapy is explained before introducing the trial option involving proton therapy. In the final 10 min of a typically 1-h encounter, patients are informed about DAHANCA 35, including a brief introduction to proton therapy, the eligibility assessment, the randomization procedure, and the practical arrangements if proton therapy requires treatment away from home. A follow-up encounter, either in person or by telephone, is scheduled for 1 to 2 d later, during which patients typically decide whether to participate in the trial.
The PtDA was developed as part of a PhD project led by the first author (A.W.K.), who managed its development and revisions. A.W.K. is a specialist cancer nurse/radiotherapist and researcher with the Danish Centre for Particle Therapy. A.W.K.’s doctoral project advisory team comprises experts serving as HCPs, clinical trialists, and methodologists.
Development Frameworks
This study was guided by 2 overarching frameworks applied across the whole process:
The Medical Research Council (MRC) framework for developing and evaluating complex interventions provided the overall approach, with scoping of core elements followed by an iterative development process.43,44
The Making Informed Decisions Individually and Together (MIND-IT) in health care framework was applied as a conceptual framework and analytic lens to understand the context in which the PtDA should function. It provided a lens for analyzing how decisions are shaped by both individual reasoning (patients and HCPs) and the interactional domain, ensuring the PtDA was developed to support decision making at both levels.48,49
Three complementary frameworks informed design and quality decisions throughout:
The Ottawa Decision Support Framework (ODSF) guided the identification of decisional needs and their translation into PtDA content and tools.30,50
The IPDAS criteria were applied to review the standard PIL, identify gaps, and ensure compliance with international quality standards for patient decision aids.29,51,52
The Measure of User- and Human-Centred Design for Personal Health Tools (UCD-11) supported planning and documentation of user involvement throughout the development process.45,53
Development Process
The development process ran from April to November 2023 and is reported in 5 steps (scoping, drafting, iterative refinement, alpha testing, and finalization), aligned with the exploration of core elements and the development process in the MRC framework. 43 Figure 1 provides an overview of the 5-step iterative process and the guiding frameworks

Five-step iterative development process of the clinical trial patient decision aid.
Step 1: Scoping
In accordance with the MRC framework for complex interventions, the scoping phase aimed to identify the core elements and contextual factors that influence trial decision making. 43 Patient and physician perspectives on barriers to and factors influencing participation in DAHANCA 35 were explored in 3 prior studies.12,19,23 Guided by the ODSF, these findings were mapped onto relevant decisional domains to inform trial-specific decision support considerations.50,54
In parallel, the DAHANCA 35 PIL was reviewed against IPDAS domains.29,51,55 The review was conducted to identify gaps in the PIL that needed to be addressed in the clinical trial PtDA to support informed, value-based decision making about participation in DAHANCA 35.
To complement these findings, a predevelopment workshop was held with HCPs involved in DAHANCA 35. During the workshop, the potential development of a PtDA was discussed in group sessions and subsequently in a plenary session. The group discussions were facilitated using a worksheet divided into 4 quadrants, each representing a discussion topic: 1) what content should be included in the PtDA, 2) the timing of providing the PtDA, 3) the expected benefits of the PtDA, and 4) concerns regarding the PtDA. Data from the workshop included completed worksheets from each group and notes taken by a designated notetaker. A.W.K. facilitated the workshop, drawing on principles from the UCD-11 to support a structured, systematic consideration of relevant stakeholder perspectives in the PtDA intervention development process.45,53
Together, these activities informed the initial scope of the PtDA by synthesizing findings from preceding studies on barriers and factors influencing trial participation, including perspectives of patients who declined participation and HCP input on PtDA content priorities and integration into the care pathway.
Step 2: Drafting the prototype (version 1)
Based on the findings in step 1, the PtDA prototype was drafted by the first author (A.W.K.).29,51 While no patients or HCPs were directly involved in this step, the development was informed by perspectives from 3 preceding studies that identified patient and HCP barriers and factors influencing participation in DAHANCA 35.12,19,23 These perspectives constituted the user input for the present development process, consistent with selected principles of user-centered design (UCD-11). 45
Step 3: Iterative development (versions 2–4)
Following the initial drafting of the PtDA prototype, the development group reviewed and discussed its content, structure, and components in two 1- to 1.5-h monthly meetings. The development group comprised the research team and PhD supervisory group (Table 1). It was selected to ensure relevant clinical and methodological expertise in head and neck radiotherapy, qualitative research, complex intervention development, shared decision making, and user-centered research. Between meetings, A.W.K. prepared revised versions, which were circulated via e-mail for comment. Data from step 3 comprised written feedback on circulated drafts and notes from group discussions. These discussions were dialogue based and guided by findings from step 1 and relevant development frameworks, including IPDAS, ODSF, and selected principles from UCD-11.29,45,50,51,54 No significant disagreements occurred, and consensus, defined as agreement without remaining objections after all comments had been reviewed, was consistently reached through this process.
Participants and Recruitment Sources

Step 4: Alpha-testing (versions 5 and 6)
To assess the comprehension and clarity of the PtDA, it was alpha tested using think-aloud interviews with patients and physicians. 56 This step represented the primary phase of user involvement in the development process. It focused on whether the content, language, and format were understandable and meaningful to the intended users and were consistent with standard approaches to alpha testing of PtDAs.42,45
Participants in the think-aloud interviews comprised patients enrolled in DAHANCA 35, who were recruited at the Danish Centre for Particle Therapy, and physicians with dual roles: researchers in DAHANCA 35 and physicians in clinical practice.
At the beginning of the think-aloud interview, participants received the PtDA (version 4). They were instructed to read each section aloud, one at a time, and to articulate their interpretation of each section. This approach provided insight into their comprehension and cognitive processes during use of the PtDA. 56 Patient interviews were conducted face-to-face by A.W.K. in a meeting room at the Danish Centre for Particle Therapy, while physician interviews were conducted by telephone.
Findings from the think-aloud interviews informed further refinement of the PtDA, resulting in version 5. This version was circulated to participants via e-mail for additional written feedback, which informed subsequent revisions leading to version 6.
Step 5: Revisions and finalization (versions 7 and 8)
Version 6 of the PtDA was shared with the development group for review. This review focused on the overall coherence of the PtDA, its intended function as a decision-support tool in clinical trials, and its feasibility for use and integration into routine clinical practice. It informed further refinement, resulting in version 7.
Consensus in the development group during step 5 was defined a priori as reached when no further objections remained after structured discussion.
Version 7 was reviewed by A.W.K. and H.B. (a professor in medical decision making) to provide an external expert perspective and ensure alignment with the IPDAS criteria. At this stage, the readability of the revised text was also assessed using the Scandinavian Readability Index (LIX), with scores converted to the Flesch–Kincaid grade level to facilitate comparison with international standards for patient-facing materials.57,58 This led to minor language refinements, resulting in the final version 8, which was deemed ready for feasibility testing.
Participants and Recruitment
The PtDA development process involved patients, HCPs, and researchers. Table 1 summarizes the participants and their recruitment sources for the 3 key activities: scoping (preceding studies and predevelopment workshop), the development group, and think-aloud interviews (alpha testing).
Patients were invited to join the development group via announcements at 7 radiotherapy clinics; however, no patients participated in the scoping and development stages. Patient perspectives were instead incorporated through preceding studies exploring HCPs’ perspectives and patient-reported barriers and factors influencing participation in the DAHANCA 35 clinical trial, as well as through alpha testing using think-aloud interviews with patients and HCPs.
Data Collection and Analysis
Data collection and analysis were guided by interpretive description. 59 Interpretive description is appropriate for an inductive, iterative development process because data collection and analysis proceed in parallel, thereby enabling iterative action on findings. 59 It also focuses on complex human phenomena and aims to develop and improve practice, aligning with a user-centered development process.45,59 Interpretation of the findings was further informed by the MIND-IT framework, which served as an analytical lens for understanding how decision making manifests at both the individual level (patients and HCPs) and within the interactional clinical context.48,49
Data sources comprised 1) 3 preceding studies on patient and physician perspectives on barriers and factors influencing participation in DAHANCA 35, 2) the DAHANCA 35 PIL reviewed against IPDAS criteria, 3) workshop materials (worksheets and contemporaneous notes), 4) minutes from development group meetings and written e-mail feedback collated by A.W.K., and 5) transcribed think-aloud interviews. Data were analyzed and used iteratively to inform successive versions of the PtDA during steps 1 through 5.
Audio records from the think-aloud interviews were transcribed verbatim and analyzed using a structured 4-step approach comprising repeated readings, coding, categorization, and theme development.56,59 All qualitative materials were organized in NVivo 15 to ensure systematic data management and analysis. 60
Results
The development and refinement of the PtDA prototype followed a structured iterative process and incorporated elements of user-centered design involving multiple stakeholders.43,45 The results are structured according to the 5 methodological steps. Step 1 reports the scoping activities, including the decisional needs identified when translating findings from the 3 preceding studies into the trial context, using ODSF; the gaps identified in the PIL through review against the IPDAS criteria; and the conclusions of the predevelopment workshop. Step 2 outlines the drafting of version 1 of the PtDA. Step 3 describes revisions made by the PtDA group during iterative development. Step 4 presents findings from the think-aloud interviews. Step 5 summarizes the final revisions and the prototype content.
Step 1: Scoping
Decisional needs were synthesized using the ODSF
Patient and physician perspectives on barriers and factors influencing participation in DAHANCA 35 were investigated and reported in 3 prior studies, drawing on HCPs in clinical practice and patients who declined to participate in the DAHANCA 35 clinical trial.12,19,23 Guided by the ODSF, their findings were translated into trial-specific decisional needs shown below with the ODSF domain in bold.30,50,54
Identified IPDAS gaps in the standard PIL
The DAHANCA 35 PIL was developed to support informed consent and to comply with ethical and regulatory requirements.24–26 When reviewed against the IPDAS criteria, which focus on patient decision support, domains not addressed by the PIL were identified.29,51,52 These domains indicate where a clinical trial PtDA could provide additional value. The following illustrates the IPDAS criteria in bold, followed by the corresponding PIL gaps to be addressed in the PtDA.
Predevelopment workshop
In April 2023, a 2-h DAHANCA 35 predevelopment workshop was held, with 24 stakeholders contributing to defining the scope and priorities for a PtDA for DAHANCA 35. Participants included HCPs involved in DAHANCA 35 across 6 radiotherapy clinics (Table 1). Recommendations reflected both practical concerns and HCPs’ perceptions of patients’ needs. In Table 2, the workshop recommendations are mapped against IPDAS domains.
Workshop Recommendations Mapped against IPDAS Domains
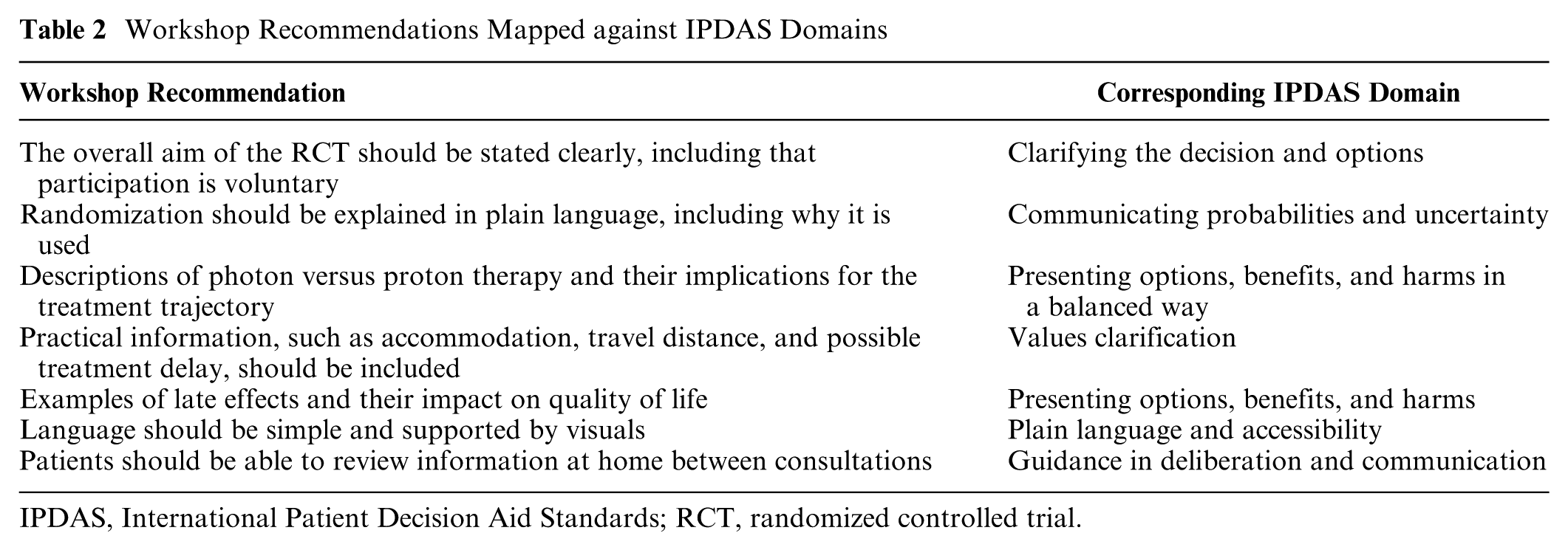
IPDAS, International Patient Decision Aid Standards; RCT, randomized controlled trial.
Synthesis across scoping activities
The 3 scoping activities demonstrated the need for structured decision support that extends beyond a standard PIL. The ODSF-based synthesis highlighted the trial-specific decisional needs of HCPs and patients who declined to participate in the DAHANCA 35 clinical trial, related to knowledge, uncertainty, emotional support, and values. The IPDAS review confirmed that these domains were insufficiently addressed in the existing PIL, identifying gaps in balanced presentation, clarification of values, support for deliberation, and accessibility. The predevelopment workshop with HCPs reinforced and expanded these findings, with stakeholders explicitly recognizing that such domains could add value to clinical trial decision making if integrated into a PtDA supplementing the PIL.
Step 2: Drafting the First Version (Version 1)
The results of step 1 were translated into a prototype of a clinical trial PtDA. The draft consisted of 19 pages structured around key domains from the ODSF framework and IPDAS.
The content of the first version is outlined below the table. Table 3 summarizes the content and revisions for versions 1 through 8.
Clarifying the decision and options: The need to decide between photon radiotherapy (standard care) and participation in DAHANCA 35 was made explicit. A brief overview of the decision and a simple decision tree outlined the 2 options.
Presenting options, benefits, and harms in a balanced way: Parallel descriptions of photon and proton radiotherapy were presented in a balanced and neutral way. A side-by-side comparison table summarized the expected effects, potential risks and late effects, impact on daily life, and treatment duration and procedures.
Communicating probabilities and uncertainty, including decisional conflict and need for support: Uncertainty associated with randomization and the principle of clinical equipoise was explained. Allocation probabilities were presented explicitly, using both natural frequencies (“two in three”) and percentages (66.6%), to set expectations regarding allocation. A dedicated section on psychological reactions to a cancer diagnosis acknowledged emotional distress and information overload at diagnosis, thereby addressing decisional conflict as defined in the ODSF.
Values clarification: Informed by practice-based insights from routine radiotherapy clinical encounters, where patient preferences often center on travel logistics and temporary accommodation, a matrix presented the main pros and cons of these considerations. The “Explore your decision” component of the Ottawa Personal Decision Guide, together with free-text fields for questions and comments, facilitated the articulation of individual tradeoffs and preferences. 54
Guidance in deliberation and communication: The SURE Test 61 and an unvalidated 11-item questionnaire on understanding, values, and support needs prompted discussion with relatives and HCPs, evaluating the perceived understanding of options and randomization, risk–benefit appraisal, clarity of personal values, perceived support and involvement, and readiness to decide, thereby identifying residual needs for further dialogue.
Plain language and accessibility: The PtDA prototype was developed as a pamphlet to ensure accessibility for all patients. It was easy to distribute in clinical settings and allowed patients to review the information at their own pace. The pamphlet followed a structured information flow with concise headings, supporting illustrations, simple terminology, a named contact person, and references, thereby enhancing readability and improving accessibility across different levels of health literacy.
Transparency and stakeholder involvement: A list of co-designers (the development group) was included, along with a brief description of the development context.
Overview of Revisions Performed during the 8 Iterations
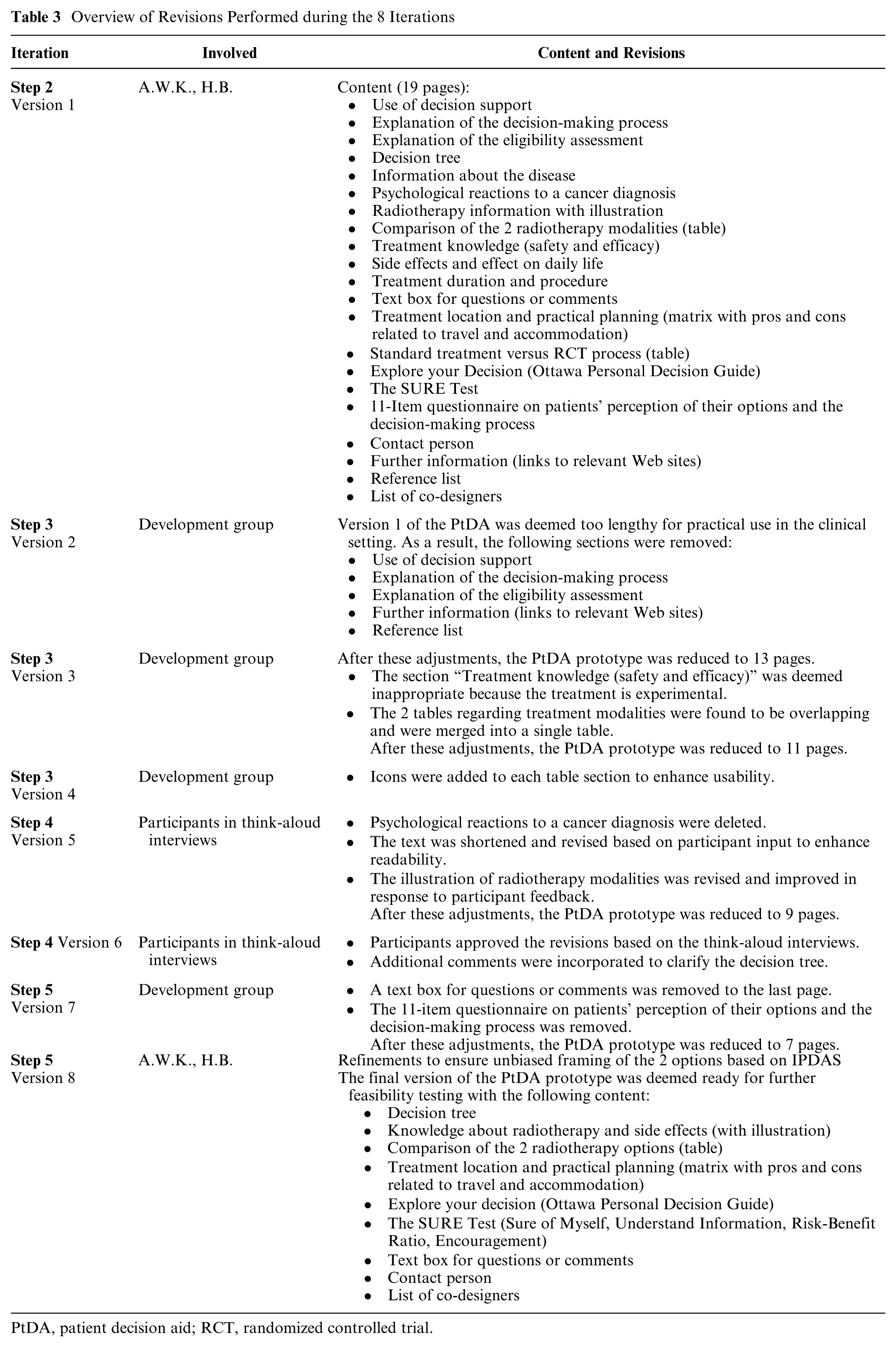
PtDA, patient decision aid; RCT, randomized controlled trial.
Step 3: Development Group Iterations (Versions 2–4)
The development group reviewed version 1 in 3 consecutive iterations. Initial feedback indicated that the PtDA was too lengthy for clinical use. In response, several sections considered nonessential were removed, including background explanations of decision support, the decision-making process, eligibility assessment, and supplementary references. These changes reduced the prototype from 19 to 13 pages (version 2).
In the next iteration, the focus shifted to the appropriateness of content. The section on “Treatment knowledge (safety and efficacy)” was removed because the trial context precluded definitive statements regarding efficacy.
Finally, revisions addressed usability. Two overlapping tables (“Comparison of the two radiotherapy modalities” and “Standard treatment vs. RCT”) were merged into a single side-by-side comparison table, and illustrative icons were added to each section to improve clarity and navigation. These adjustments further streamlined the PtDA, resulting in an 11-page prototype (version 4), which was then taken forward to alpha testing.
Step 4: Alpha Testing Using Think-Aloud Interviews (Versions 5–6)
During September and October 2023, version 4 of the PtDA was alpha tested in think-aloud interviews with 13 participants, including 5 patients with pharynx or larynx cancer (4 male, 1 female, aged 51–55 y) and 8 HCPS (6 physicians, 2 nurses) from 5 radiotherapy clinics (Table 1). All invited participants agreed to take part, and all interviews were deemed eligible for analysis.
The think-aloud interviews provided insights into participants’ comprehension, interpretation, and immediate impressions of the PtDA. Three themes emerged:
Plain language and contextual clarity: Participants highlighted language and terminology as central to comprehension. Compound words and medical jargon were perceived as challenging, and terms such as “photons” were replaced with more familiar words, such as “X-rays,” because “photons” and “protons” were too similar and challenging for patients to distinguish. Participants also emphasized that readability and navigability should be prioritized, with only essential information included. A section on psychological reactions to cancer was therefore removed as it was deemed irrelevant to the decision context. Visual design elements, particularly icons, were well received for their support of orientation and comprehension.
Supporting deliberation and comparison of options: Participants found the decision tree, the radiotherapy modality illustration, and the comparison table particularly useful for clarifying the 2 options. These features helped participants weigh the pros and cons and articulate their own preferences, thereby fostering more informed, value-based decision making. To improve clarity, the decision tree was revised, and the comparison table was enhanced.
Accessibility across clinical and home settings: Both patient and HCP participants emphasized the importance of patients being able to take the PtDA home, allowing them to process the information at their own pace and discuss it with their relatives. The pamphlet format was therefore retained and further simplified to enhance usability in both clinical and home settings.
Based on feedback from think-aloud interviews, the PtDA was revised to version 5. Changes included simplifying the language, removing the section on psychological reactions, revising the modality illustration, and clarifying the decision tree. Participants subsequently reviewed version 5 and approved the revisions, with minor comments leading to version 6. At this stage, the PtDA had been reduced to 9 pages.
Step 5: Revision and Finalization (Versions 7–8)
In version 6, the exploratory 11-item questionnaire and a text box for questions or comments were removed, reducing the PtDA to 7 pages to improve feasibility for routine clinical use and to inform subsequent refinement in version 7.
The review of version 7 confirmed alignment with the IPDAS criteria. This refinement resulted in only minor linguistic corrections to ensure unbiased wording and a balanced presentation of photon (X-ray) radiotherapy and trial participation. Readability testing indicated that the text corresponded to an eight- to ninth-grade reading level, consistent with international recommendations for patient-facing materials. Minor corrections were then made, resulting in the final version 8 (Appendix 1), which was agreed upon as the final prototype and prepared for feasibility testing.
Discussion
Through an iterative development process that incorporated elements of user-centered design, a PtDA was developed to support patients in considering participation in DAHANCA 35, an RCT comparing proton and photon radiotherapy.43,45 The PtDA was designed to address decisional needs identified among patients who declined participation in the DAHANCA 35 clinical trial and HCPs in the clinical trial context and to fill gaps identified when the standard PIL was reviewed against IPDAS criteria, ensuring balanced presentation of options, clarity of information, explicit communication of uncertainty, and prompts to support deliberation and dialogue.29,51,52 Development was informed by 3 preceding studies in the DAHANCA 35 context, a multidisciplinary workshop, iterative revisions by the development group, and think-aloud interviews with patients and HCPs.12,19,23
The PtDA addresses key decisional needs among patients with head and neck cancer who are considering clinical trial participation. It explains what an RCT is, clarifies equipoise, and illustrates randomization with simple terms, including allocation probabilities. Practical implications, such as travel and accommodation, are explicitly included. Information is presented in parallel formats, with diagrams and side-by-side tables to minimize processing bias. The SURE test is integrated as a prompt for patients to reflect at home and bring to the subsequent consultation, enabling HCPs to identify unresolved decisional conflict and provide tailored support. 61 In this way, the PtDA supplements the mandatory PIL by supporting deliberation and values clarification.30,50,54
IPDAS criteria and the MRC framework for complex interventions guided the development process.29,43,51,52 IPDAS standards on balanced information, clarity of options, uncertainty, and guidance in deliberation were systematically addressed. The MRC framework provided methodological rigor and structured the development phase; subsequent feasibility and implementation work are reported separately. The development process was further informed by the MIND-IT framework, which provided a conceptual perspective on decision making as both an individual cognitive process and an interactional clinical activity. This perspective was particularly relevant in the context of clinical trial participation, where decisions are shaped through dialogue between patients and HCPs. By explicitly attending to both levels of decision making, the framework informed the design of a PtDA that is feasible, acceptable, and usable in routine clinical practice.
This study has several limitations that should be considered. First, despite invitations across 6 radiotherapy clinics, no patient partners attended the development phase. Patient perspectives on barriers and factors influencing participation in DAHANCA 35 were incorporated through 3 prior studies in the DAHANCA 35 context and alpha testing. Still, earlier co-design may have strengthened the user-centered approach.12,19,23,45 Second, no quantitative assessment of PtDA acceptability or usefulness was collected during development, limiting insight into whether feedback reflected broader consensus or individual views. While such an assessment is typically part of feasibility testing, its absence is acknowledged here as a limitation. 43 The implications of this study lie in its rigorous, iterative development process, which incorporated elements of user-centered design and may serve as a model for others developing clinical trial decision aids in oncology. Within the MRC framework for complex interventions, this approach is broadly applicable and may also inform decision support for clinical trial participation in other specialties.
Conclusions
This study reports the systematic development of a PtDA to support individuals with head and neck cancer in deciding whether to participate in an RCT comparing proton versus photon radiotherapy. Grounded in IPDAS criteria and informed by patient and HCP perspectives throughout iterative development phases, the PtDA provides balanced, accessible information, support, and values clarification. The development process may serve as a model for future trial decision aids in oncology and beyond.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683261441513 – Supplemental material for Development of a Patient Decision Aid for the DAHANCA 35 Proton Radiotherapy Trial: An Iterative Development Process with User-Centered Design Elements
Supplemental material, sj-docx-1-mpp-10.1177_23814683261441513 for Development of a Patient Decision Aid for the DAHANCA 35 Proton Radiotherapy Trial: An Iterative Development Process with User-Centered Design Elements by Anne Wilhøft Kristensen, Annesofie Lunde Jensen, Kenneth Jensen, Susanne Oksbjerg Dalton, Jeppe Friborg, Cai Grau and Hilary L. Bekker in MDM Policy & Practice
Footnotes
Acknowledgements
We thank the patients and health care professionals who contributed to the workshop and think-aloud interviews. Their perspectives provided crucial insights that enriched this development process. We are also grateful to the clinicians, researchers, and methodologists from the University of Aarhus and the University of Leeds with whom we discussed this study. Their valuable knowledge and perspectives have significantly shaped this work. Finally, we acknowledge the Danish Head and Neck Cancer Study Group (DAHANCA) for its contribution, approval, and recognition of this study. Each of these contributions was essential, and this study would not have been possible without them.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Comprehensive Cancer Centre (DCCC) under grant number 0310 and by a grant from the Novo Nordisk Foundation (NNF18OC0034612).
Author Contributions
AWK, conceptualization, formal analysis, investigation, writing–original draft, writing–review and editing, visualization, project administration; JF, conceptualization, supervision, funding acquisition; KJ, conceptualization, writing–review and editing, supervision; SOD, conceptualization, writing–review and editing, supervision; ALJ, conceptualization, formal analysis, writing–review and editing, supervision; CG, conceptualization, writing–review and editing, supervision, project administration, funding acquisition; HB, conceptualization, formal analysis, writing–review and editing, visualization.
Ethical Considerations
This study complies with the principles of the Declaration of Helsinki. Ethical approval was obtained from the relevant ethics committee as an amendment (109830) to the host RCT, reflecting the implementation of a new strategy for informing patients through the PDA. Approval was also granted by the Danish Data Protection Agency (record No. 1–10-72–181-20), and the study was registered on ClinicalTrials.gov (identifier: NCT06291610).
Consent to Participate
Participants who contributed to developing the clinical trial PtDA prototype received written and verbal information about the study and provided written consent to be interviewed. Their identities remain anonymous, and references are made using identification numbers.
Consent for Publication
Specific consent for publication was not obtained, but participants were anonymized and informed of the research objectives. No identifiable data are included in this publication.
ORCID iDs
Data Availability
The data supporting the results in the current study are available upon request by contacting the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.