
Abstract
Highlights
Our results provide arguments supporting the decision of suspending kidney transplantation activity in case of future crises, provided that the moratorium duration does not exceed a few months.
We report that patients active on the waitlist at the beginning of the moratorium lose the most quality-adjusted life-years due to the suspension, particularly candidates younger than 60 y. Hence, if another crisis occurs with the possibility of maintaining only small kidney transplantation activity, giving priority to younger patients active on the list may be justified.
Considering quality-adjusted life-years rather than raw survival time results in a more complete assessment of the effect of suspending kidney transplantation in patients with end-stage renal disease by taking their quality of life into account.
Keywords
During the earliest period of the COVID-19 pandemic, many hospitalizations were postponed due to the shortage of health care resources. In particular, kidney transplantation (KT) activity was suspended in many countries to redeploy hospital care capacities for pandemic management. This decision also aimed to reduce the risk of severe forms of COVID-19 in kidney transplant recipients due to their immunosuppressed status. 1 In France, KTs were officially suspended from March 16 to May 11, 2020, corresponding to a decrease of nearly 600 KTs compared with the same period in 2019. KT activity remained limited until June 2020.
Several studies have reported the effect of these moratoriums on the life expectancy of populations with end-stage renal disease (ESRD) and candidates for KT.2–5 In particular, Massie et al. 3 predicted a 2.9-mo loss in 5-y life expectancy when delaying transplantation up to 12 mo. Bonnemains et al. 4 predicted no significant differences in 10-y life expectancy for the observed French moratorium. 4 The 2 studies support the feasibility of temporarily stopping KT activity. Nevertheless, McElroy et al. 6 called for further predictive tools to evaluate the risks versus benefits of KT during an epidemic.
The previous studies mainly focused on mortality and access to KT as outcomes. Only Vinson et al. 5 considered health-related quality of life (HRQoL), which has been identified as an important component of the core outcomes set for ESRD patients 7 and kidney transplant recipients. 8 It is well-established that dialysis is associated with lower HRQoL compared with KT.9,10
Consequently, for crisis preparedness, we aimed to predict the impact of a wide range of durations of KT moratoriums in terms of expected numbers of quality-adjusted life-years (QALYs) of the ESRD population who are candidates for KT. 11 In the future, such moratoriums could be considered in case of different types of crises, including but not limited to a new COVID pandemic (war, shortage, another pandemic, etc.). The QALYs principle is to convert a health state sequence over time into an equivalent number of years lived in perfect health (i.e., a composite outcome merging both quantity and quality of life). Initially designed for the economic evaluation of health programs, 12 the composite nature of QALYs can also support decision making in clinical studies. 13
Patients and Methods
Training Cohorts
This study was performed in accordance with the Helsinki Declaration and approved by the scientific councils of the REIN registry (Renal Epidemiology and Information Network, data collection was approved by the National Commission for Data Protection and Liberties, CNIL No. 180092587) and the DIVAT cohort (Données Informatisées et Validées en Transplantation, CNIL No. 891735).
The first training cohort, used to estimate the predictive models of the natural history of the ESRD, was based on the children and adults who entered the French REIN registry between September 1, 2011, and December 31, 2019. This registry enables the tracking of patients’ health evolution through the health states defined in Figure 1. More precisely, registration corresponded to the time of the first dialysis or the registration on the waiting list for preemptive KT candidates. We did not include patients from overseas districts, those without follow-up, or those registered for multiorgan transplantation. The age, sex, body mass index, diabetic status, history of cardiovascular comorbidities, region of residence, and calendar year were collected at the time of entry into the registry.

Multistate natural history of end-stage renal disease from entry into the REIN registry (chronic kidney disease [CKD] stage 5). Patients “inactive on the list” are registered on the waitlist for kidney transplantation (KT) with a temporary contraindication (cancer, cardiovascular event, etc.): they cannot access KT until the latter is withdrawn. In contrast, patients “active on the list” might access KT at any time. Patients “not listed” are not registered on the waitlist. Patients who started dialysis while being registered on the waitlist at inclusion were considered beginning dialysis first and being registered on the waitlist afterward.
The second training cohort, used to estimate post-KT HRQoL, was based on the French DIVAT cohort. Inclusion criteria were adult recipients of a single kidney graft from a deceased or living donor who completed at least 1 EQ-5D questionnaire. We considered the following characteristics because they were available in both DIVAT and REIN and possibly associated with patient survival and HRQoL: age at transplantation, gender, body mass index, history of diabetes, history of cardiovascular comorbidities, preemptive registration, and time since transplantation.
Statistical Analyses
Estimation of the natural history of the disease and simulations according to the moratorium durations
The analysis can be decomposed into several steps. First, we estimated a multistate model with cause-specific Cox regressions for each health-state transition defined in Figure 1 under normal conditions (about 300 KT per month) using the first training cohort. Second, we estimated several generalized linear models depicting the number and characteristics of incident ESRD patients from the first training cohort as well. Third, these models were used to simulate the evolution of the KT waitlist and of the French ESRD population from March 16, 2020 (i.e., the date of the French COVID-19–related KT moratorium), considering several moratorium durations. The competing events were simulated following the recommendations of Beyersmann et al. 14 We assumed KT activity similar to that observed before the moratorium. All of these steps were performed identically to Bonnemains et al., 4 where they are described in detail, resulting in an identical multistate model.
Estimation of the utility scores among the KT recipients
Using the second training cohort described above, we estimated a linear mixed-effects model (LME) to model the utility scores of KT recipients in the DIVAT cohort (Supplementary Table S1). Utility scores are synthetic HRQoL scores in which 0 corresponds to death and 1 corresponds to perfect health. As the French EQ-5D-3L scoring allows utility scores ranging from −0.53 to 1, 15 we truncated the LME predictions so that they all lie within that range. The time effect was modeled considering 2 slopes before and after 1 y post-KT. A random intercept and a random evolution slope during the first year post-KT were considered to account for repeated observations. A random slope after 1-y post KT was not included because it resulted in a higher Bayesian information criterion. We performed a forward selection (P < 0.05, likelihood-ratio statistics) for the previously listed explicative characteristics.
Estimation of utility scores for the dialysis and/or waitlisted patients
We estimated the utility of a patient on the waiting list by applying decrements obtained from the models proposed by Li et al. 16 to the 6-mo post-KT HRQoL (obtained from the previous LME). As synthetized in Supplementary Table S2 and Appendix A, this conversion depended on the time spent in dialysis.
Computation of QALYs
Utility scores were simulated using the time-dependent utility functions at the beginning of each health state of each patient according to the LME and conversions from Li et al. 16 (Supplementary Tables S1–2). Random effects and residuals were simulated to reproduce the variability estimated in the LME.
This utility simulation process using different data sources is illustrated on Supplementary Figure S1. QALYs were then calculated without discount rate by summing the integrals of the utility functions over the times spent in the health states.
Estimations of the moratorium impact
Being registered on the active waitlist is a prerequisite for KT. Therefore, only patients who access the active waitlist at a given time may be affected by a KT moratorium. We distinguished 3 subpopulations (Supplementary Figure S2): 1) patients active on the waiting list at the beginning of the moratorium (population A), 2) prevalent ESRD patients inactive or not registered on the waiting list at that time who will become active within the next 5 y (population B), and 3) incident ESRD patients after the beginning of the moratorium who will become active candidates for within the next 5 y (population C). Hence, all patients active on the waitlist at any given time within a 5-y window from the beginning of the moratorium are considered, whether they eventually access KT or not. We considered moratoriums ranging from 1 mo to 12 mo and predicted their effects at a 10-y horizon compared with no moratorium. In addition to QALYs, we also considered the restricted mean survival time (RMST). 17 Because survival and HRQoL are correlated with age, we also performed a subgroup analysis to compare the impact of the moratorium between patients younger and those older than 60 y. Each scenario was simulated 1,000 times, and nonparametric 95% confidence intervals (CIs) were derived for each outcome using the 2.5% and 97.5% percentiles.
Sensitivity analysis
In what precedes, we assumed HRQoL differences between kidney transplant recipients and dialyzed patients based on Li et al., 16 with a maximum utility decrease of 0.07 for more than 3 y spent in dialysis (Supplementary Table S2). Nevertheless, other studies estimated a greater difference in HRQoL between kidney transplant recipients and dialyzed patients.9,18 Therefore, we performed a sensitivity analysis following exactly the same modeling strategy but assuming a higher difference in HRQoL, with a utility decrease due to dialysis of 0.25 as reported by Liem et al. 18
The statistical analyses were performed using R version 4.5.0.
Results
Description of the Studied Populations
The 76,980 incident ESRD patients in the period from 2011 to 2019 of the REIN registry included to model the natural history of the disease (first training cohort) were described previously. 4 On March 16, 2020, the registry included 89,972 patients: 40,544 (45.1%) had a functional kidney transplant, 46,328 (51.5%) were undergoing dialysis, and 3,100 (3.4%) were registered for preemptive KT. Among these 89,972 patients (prevalent cohort), 8,350 were on the active waitlist (population A), and an average of 10,862 patients (across our simulations) accessed the active waitlist before March 16, 2025 (population B). We simulated an average of 16,355 incident patients in the registry after March 16, 2020, and active on the waitlist before March 16, 2025 (population C). We describe their characteristics in Table 1, in comparison with the 2,870 kidney transplant recipients of the DIVAT cohort involved in the modeling of the post-KT HRQoL. Note that 2,878 recipients completed at least 1 EQ-5D questionnaire, but 8 (0.3%) were excluded due to missing data on at least 1 of the considered characteristics.
Description of Kidney Transplantation (KT) Recipients and the 3 Populations of KT Candidates: Active on the Waiting List on March 16, 2020 (Population A); Inactive or Not Registered on the Waiting List on March 16, 2020, but Who Will Become Active before March 16, 2025 (Population B); and Incident Patients after March 16, 2020, Who Will Become Active Candidates for KT before March 16, 2025 (Population C).

Data are presented as the mean (±standard deviation) or effective (%).
For KT recipients, age at transplantation; for KT candidates, age at the beginning of the KT moratorium for patients active on the list at this time or at the registration on the active list for the other 2 populations.
Among the 2,870 kidney transplant recipients (second training cohort), the mean age at transplantation was 50.0 y (±14.0 y), and 62.8% were men. The transplantation year ranged from 2000 to 2021, 598 KT recipients (20.8%) underwent preemptive transplantation, and the mean dialysis time before nonpreemptive transplantation was 3.3 y (±3.7 y). The post-KT HRQoL modeling was based on 4,881 questionnaires and 1,175 patients (40.9%) completed several questionnaires (up to 10). The mean utility reported was 0.82 (±0.24). Delay from the transplantation to the first questionnaire completion ranged from 0 to 21.3 y, with a median at 3.5 y (interquartile range [1.0, 7.8 y]). The multivariate LME estimated from this second training cohort is described in Supplementary Table S1 and its calibration by Supplmentary Figures S3 to 4. The predictions resulting from the estimated model presented a root mean squared error of 0.08 and a mean absolute error of 0.06 when considering random effects and 0.22 and 0.17, respectively, otherwise.
Effects of the Moratorium on Life Expectancy and QALYs
Patients active on the list on March 16, 2020 (population A)
The outcomes at a 10-y horizon are reported in Figures 2 and 3 and in Table 2 and Supplementary Table S3. In the scenario without a KT moratorium, we estimated a 10-y RMST of 8.30 y (95% CI [8.25, 8.36]), corresponding to a life expectancy of 8.30 y for a cohort followed up to 10 y. The mean number of QALYs was 6.28 y (95% CI [6.23, 6.34]), which corresponds to the expected number of years lived in perfect health for a cohort followed up to 10 y.
Impact of the kidney transplantation (KT) moratoriums on the restricted mean survival time for a 10-y follow-up for the 3 populations: (a) active on the waiting list on March 16, 2020; (b) inactive or not registered on the waiting list on March 16, 2020, but active before March 16, 2025; and (c) incident patients after March 16, 2020, who will become active candidates for KT before March 16, 2025.

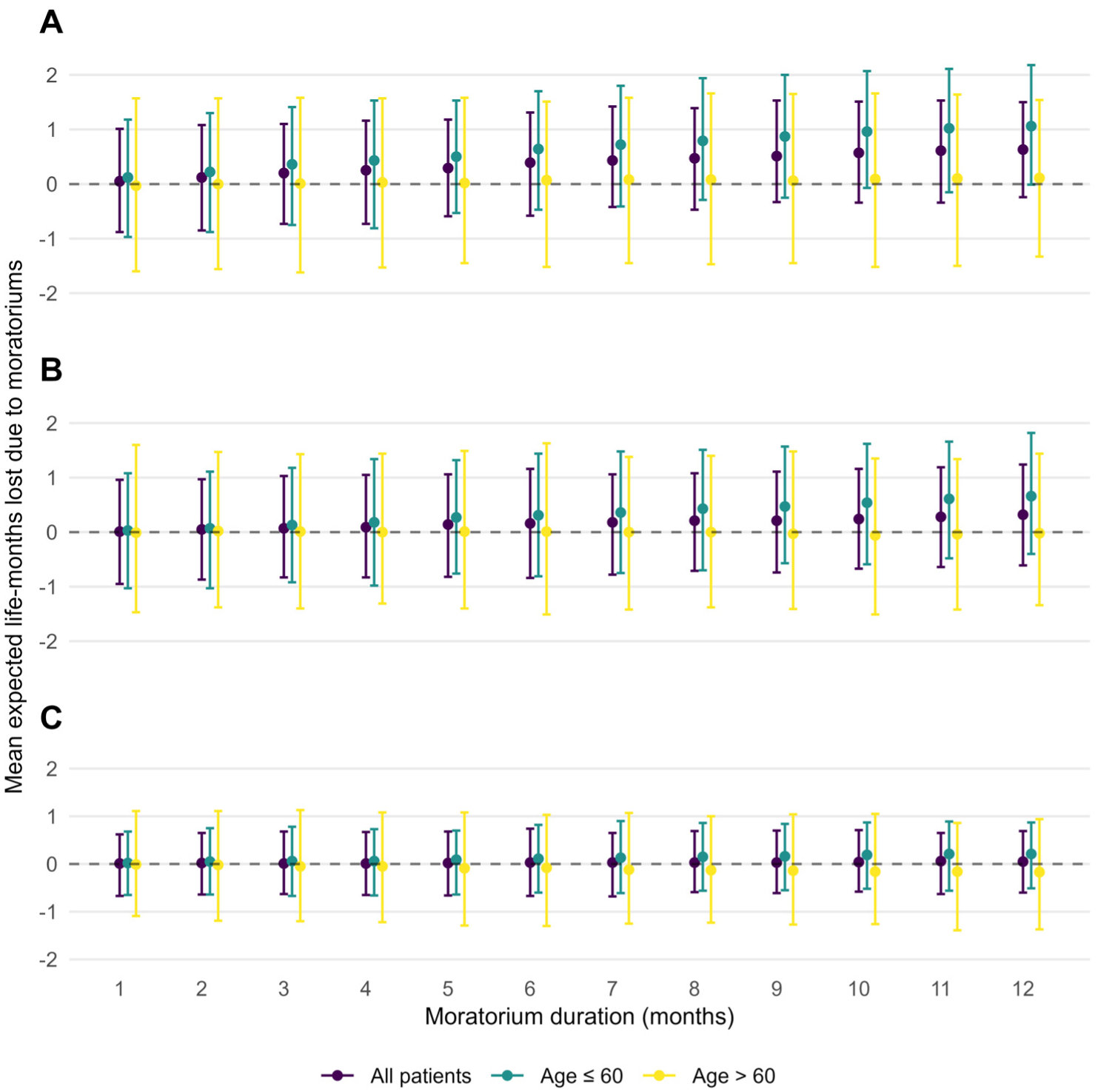
Impact of the kidney transplantation (KT) moratoriums on the quality-adjusted life-years (QALYs) for a 10-y follow-up for the 3 populations: (a) active on the waiting list on March 16, 2020; (b) inactive or not registered on the waiting list on March 16, 2020, but active before March 16, 2025; and (c) incident patients after March 16, 2020, who will become active candidates for KT before March 16, 2025.
Impact of the KT Moratoriums for a 10-y Horizon on the 3 Populations: Active on the Waiting List on March 16, 2020; Inactive or Not Registered on the Waiting List on March 16, 2020, But Active before March 16, 2025; and Incident Patients after March 16, 2020, Who Will Become Active Candidates for KT before March 16, 2025.
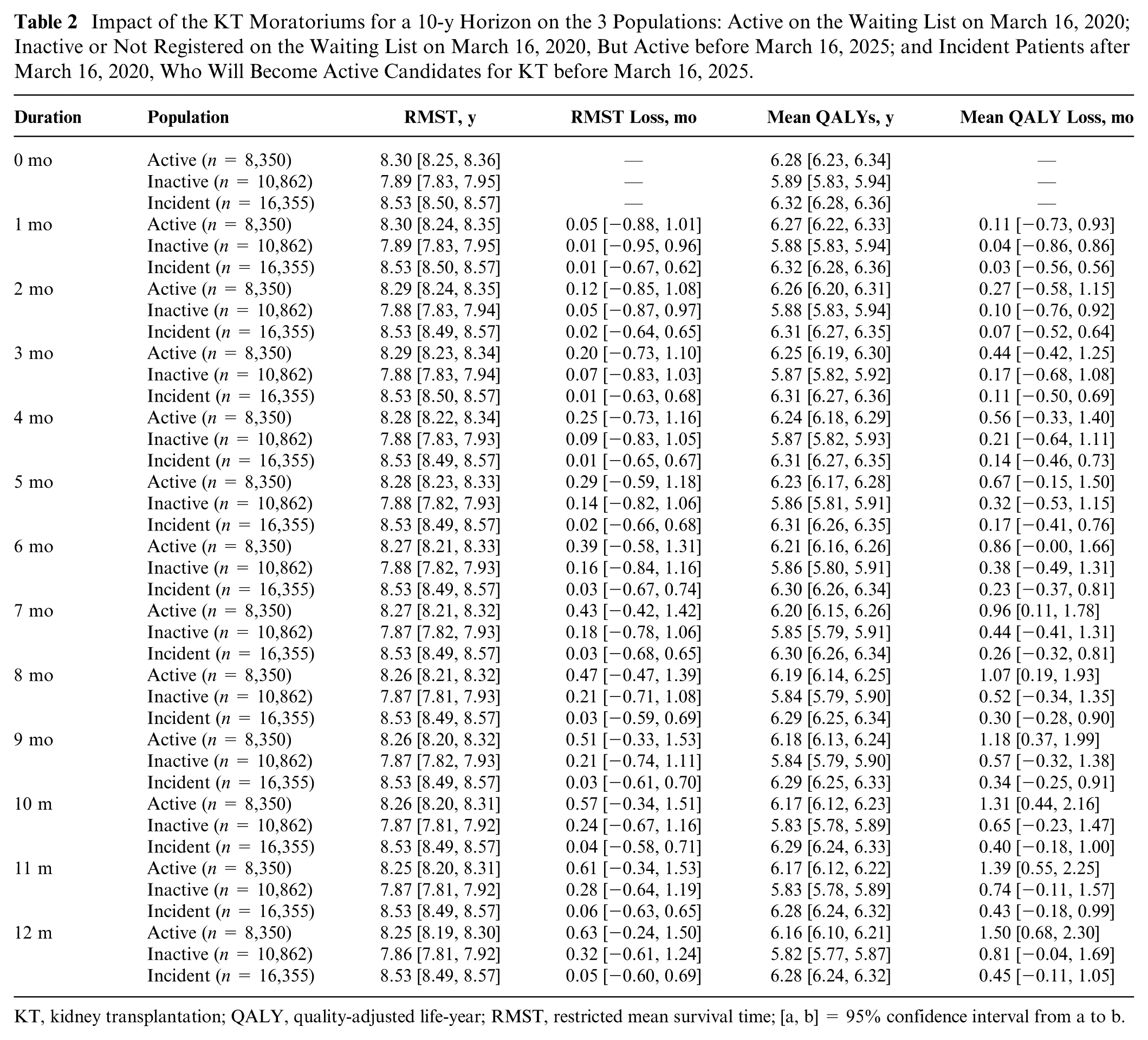
KT, kidney transplantation; QALY, quality-adjusted life-year; RMST, restricted mean survival time; [a, b] = 95% confidence interval from a to b.
As previously reported, 4 the predicted loss in the 10-y RMST in moratorium durations from 1 to 12 mo was too small to be demonstrated as significant (0.63 mo lost, 95% CI [−0.24, 1.50] for a 12-mo moratorium). In contrast, for a 7-mo moratorium, we estimated a mean loss of 0.96 mo (95% CI [0.11, 1.78]). Population wise, this corresponded to a total of 670 (95% CI [77, 1,241]) life-years in perfect health lost among the 8,350 patients. Moreover, the restricted mean survival time on the waiting list (RMWL) increased by 10.51 mo (95% CI [9.37, 11.57]).
Patients who were inactive or not registered on the list on March 16, 2020, and become active candidates before March 16, 2025 (population B)
In case of no moratorium, we estimated a 10-y RMST of 7.89 y (95% CI [7.83, 7.95]) and a mean QALY of 5.89 y (95% CI [5.83, 5.94]). The predicted 10-y RMST and mean QALY losses were too small to be demonstrated as significant, for any moratorium duration. For the maximum simulated duration of 12 mo, the mean QALY loss was 0.81 mo (95% CI [−0.04, 1.69]), which is comparable to the QALY loss due to a 6-mo moratorium in population A. Population wise, it corresponded to a total loss of 733 (95% CI [−36, 1,529]) life-years in perfect health among the 10,862 patients. In this scenario, the estimated RMWL increase was 8.83 mo (95% CI [7.90, 9.82]).
Incident ESRD patients after March 16, 2020, who will become active candidates before March 16, 2025 (population C)
Assuming no moratorium, we predicted an RMST of 8.53 y (95% CI [8.50, 8.57]) and a mean number of QALYs of 6.32 y lived in perfect health (95% CI [6.28, 6.36]) for a 10-y follow-up. Again, in all scenarios, we predicted RMST or mean QALY losses that were too small to be demonstrated as significant. For a 12-mo moratorium, the predicted mean QALY loss was 0.45 mo (95% CI [−0.11, 1.05]), which is comparable to the QALY loss due to a 3-mo moratorium in population A. It corresponded to a total of 613 (95% CI [−144, 1,432]) life-years in perfect health among the 16,355 patients. In this scenario, the estimated RMWL increase was 5.88 mo (95% CI [5.06, 6.72]).
Moratorium Effects according to Age of the Patients
The RMST and mean QALY losses were higher for patients younger than 60 y than for older patients regardless of the studied population and the moratorium duration (Figures 2 and 3, Supplementary Tables S4 and S5).
In population A, we predicted a loss of 1.29 mo lived in perfect health (95% CI [0.06, 2.50]) for a 7-mo moratorium in patients younger than 60 y. This is higher than the estimated loss for patients older than 60 y in case of a 12-mo moratorium (1.01 mo lived in perfect health, 95% CI [−0.21, 2.30]).
In population B, we predicted a QALY loss of 1.13 mo lived in perfect health (95% CI [0.06, 2.25]) for a 12-mo moratorium in patients younger than 60 y, compared with 0.45 mo lived in perfect health (95% CI [−0.80, 1.71]) for patients older than 6 y0.
In population C, we predicted losses of 0.61 mo lived in perfect health (95% CI [−0.10, 1.35]) and 0.22 mo lived in perfect health (95% CI [−0.77, 1.33]) in patients younger than and older than 60 y, respectively.
Sensitivity Analysis
Assuming a constant difference of 0.25 between the utilities of KT versus dialysis regardless of the patient characteristics, we reported larger QALYs losses. For population A, a 3-mo moratorium resulted in a decrease of 1.27 mo of life in perfect health (95% CI [0.25, 2.13]) at a 10-y horizon. Comparable losses were estimated in populations B and C for moratoriums of 7 mo (1.29 mo of life in perfect health lost, 95% CI [0.41, 2.21]) and 11 mo (1.25 mo of life in perfect health lost, 95% CI [0.53, 1.97]), respectively.
Discussion
The COVID-19 pandemic has shown that we could be forced to stop KT activity in crisis contexts. We have to better prepare for future crises, which could also be due to multiple other causes (nuclear incident, war, shortage, etc.). Should that happen, being able to assess the costs of suspending KT activity would be of great importance.
According to our simulations, the most impacted population will be patients active on the waitlist. For patients active on the waitlist at the beginning of the moratorium, we predicted a loss of 0.96 life-months in perfect health for a 7-mo moratorium (95% CI [0.11, 1.78]). This result highlights the importance of considering both the quantity and the quality of life because we reported smaller effects on life expectancy, even for a 12-mo duration. In our simulations, these patients’ access to KT was delayed by more than the duration of the moratorium. This result illustrates the fact that candidates who are registered on the waitlist after KT resumes may access transplantation before someone who was already on the active waitlist at the beginning of the moratorium, since waiting time is not the only allocation criterion. Additional research into the ethical concerns of postmoratorium graft allocation would be interesting but is beyond the scope of our work. We reported smaller losses in mean QALYs for patients who become active candidates after a moratorium decision. Therefore, given the overall low impact of the moratoriums, our results confirm the sustainability of suspending KT activity in case of future crisis, 4 provided that the moratorium duration does not exceed a few months.
Because future decisions regarding suspending KT activity can vary according to patient age, we additionally investigated the impact of KT moratoriums on patients younger or older than 60 y. In the 3 considered populations, we reported higher losses of QALYs for patients younger than 60 y than for older patients, regardless of the moratorium duration. In particular, in the most affected population was composed of patients active on the waitlist at the beginning of the moratorium; a 3-mo moratorium resulted in an impact on patients younger than 60 y that was comparable with that of a 7-mo moratorium on patients older than 60 y (0.60, 95% CI [−0.57, 1.77] and 0.63, 95% CI [−0.65, 1.91] quality-adjusted life-months lost, respectively). If another crisis happens with the possibility of maintaining only small KT activity, giving priority to younger patients active on the list may therefore be justified. Note that this decision may satisfy 3 principles for allocation in case of scarcity: youngest first, maximization of QALYs, and saving the most lives. 19
In a previous study, Vinson et al. 5 reported that maintaining KT activity during the COVID-19 pandemic was preferable both in terms of quantity and quality of life. They assumed utilities of 1 for kidney transplant recipients versus 0.8 for patients in dialysis. Our work offers a more precise estimation of QALYs lost due to KT moratoriums by taking patients characteristics into account.
However, our study suffered from several limitations. With regard to multistate modeling, the following limitations have been previously detailed 4 : possible bias of extrapolation due to the training cohort of incident patients in the registry between 2011 and 2019, the absence of overmortality related to the crisis, and the increase in the number of dialysis patients potentially outnumbering the available capacities. It should also be noted that the simulation of moratorium-dependent health-state transitions from the French ESRD population in March 2020 resulted in partially paired data. The use of an unpaired nonparametric CI may therefore overestimate the dispersion of the estimands. In this novel QALY-based study, we predicted KT patients’ longitudinal utility scores using an LME. This choice of modeling can be questioned considering the typical features of utility distributions, notably boundedness, right-skewness, and a mass of observations at the maximum value. However, despite these theoretical limitations, the LME was reported to be the best calibrated model in a previous study aimed at modeling the utility scores of the KT recipients from the clinical characteristics in the DIVAT cohort. 20 Moreover, our simulations did not directly account for the potential correlation between life expectancy and quality of life, even if we considered covariates associated with both survival probability and HRQoL, which are susceptible to at least partly capture this correlation. To the best of our knowledge, there are currently no available predictive models of both the quantity and quality of life. Another limitation is the absence of utilities collected in dialyzed patients. We used the models proposed by Li et al. 16 to convert utilities to dialysis and waitlisted patients, which did not allow us to distinguish the utility scores associated with all health states defined in Figure 1, especially the patients active or inactive on the waiting list. Even though the validity of this conversion can be questioned, it is reassuring to note that the mean observed utility in our cohort was close to the one estimated for KT recipients in the model proposed by Li et al. 16 We referred to the study of Li et al. because it was a recent publication that provided an EQ-5D–based multivariate adjusted estimation of utility scores among both kidney transplant recipients and waitlisted patients as well as distinguished the latter according to the time spent in dialysis. Nevertheless, other models could have been chosen.9,18 They reported utility differences between dialysis and kidney transplant recipients of 0.11 and 0.25, respectively. Therefore, we performed a sensitivity analysis with the estimation proposed by Liem et al. 18 (the worst-case scenario for the KT moratorium). This resulted in greater effects of the moratorium. For the most affected population, a 3-mo moratorium resulted in a loss of 1.27 mo of life in perfect health (95% CI [0.25, 2.13]) at a 10-y horizon. In our subgroup analysis, we compared only patients older than 60 y to younger ones. Lastly, we did not evaluate the potential benefits of the KT moratoriums. Although providing a reliable estimation of these benefits would be useful, they are likely to depend on the type of crisis faced. In our work, we preferred to focus on costs in terms of quantity and quality of life for the population so that the results may remain relevant in case of any future crisis. Furthermore, considering the potential benefits of the moratorium would likely strengthen our conclusion that such a decision can be sustainable.
To conclude, our QALY-based results suggest that KT moratoriums can be sustainable with regard to both quantity and quality of life, provided they do not exceed a prolonged period. In case of future crisis, our study can provide health authorities with valuable QALY predictions to decide to suspend suspending or reduce KT activity. Especially in the case of a long reduction in KT activity, we reported that priority may be proposed to younger patients.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683261440974 – Supplemental material for Crisis Preparedness by Simulating Quality-Adjusted Life-Year Loss in Patients with End-Stage Renal Disease due to Kidney Transplantation Suspensions
Supplemental material, sj-docx-1-mpp-10.1177_23814683261440974 for Crisis Preparedness by Simulating Quality-Adjusted Life-Year Loss in Patients with End-Stage Renal Disease due to Kidney Transplantation Suspensions by Vincent Bonnemains, Florent Le Borgne, Etienne Dantan, Myriam Pastural, Magali Giral, Cécile Couchoud and Yohann Foucher in MDM Policy & Practice
Footnotes
Acknowledgements
The authors would like to thank the REIN registry and the DIVAT consortium for providing the data for this study. We also thank all patients, the physicians who helped recruit them, and the clinical research associates who participated in data collection.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant overseen by the French region Pays de la Loire and the French National Research Agency (ANR-20-COV8-0002-01, ANR-22-CE36-0009-01). The funders had no role in the study design, analysis and interpretation of data, writing of the report, or the decision to submit the report for publication.
Author Contributions
Y.F. supervised this work. F.L.B. and V.B. performed the simulations and other statistical analyses. C.C. and M.G. performed the data extraction. V.B., F.L.B., E.D., M.G., M.P., C.C., and Y.F. participated in the design of the study and were engaged in the writing of the final proposal.
Ethics Approval and Consent to participate
This study was performed in accordance with the Helsinki Declaration and approved by the scientific councils of the REIN registry (Renal Epidemiology and Information Network; data collection was approved by the National Commission for Data Protection and Liberties, CNIL No. 180092587) and the DIVAT cohort (Données Informatisées et Validées en Transplantation, CNIL No. 891735). Informed consent was collected for all patients at inclusion in the REIN registry and the DIVAT cohort, whose scientific councils approved the present study.
Consent for Publication
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.