
Abstract
Highlights
Identified barriers and facilitators on shared decision making for breast reconstruction from multistakeholder perspectives in China’s health care context.
Explored cultural influences on shared decision making for breast reconstruction in Chinese patients.
Emphasized the importance of integrating shared decision making into existing clinical workflows.
Proposed integrating traditional Chinese medicine diagnostics with shared decision making for culturally sensitive care.
Breast cancer is the most common malignant tumor among women worldwide and the leading cause of cancer-related mortality in women, posing a significant threat to women’s health. 1 Mastectomy is a common surgical treatment for breast cancer, 2 but it often has a profound impact on patients’ body image and psychosocial health.3,4 To mitigate the adverse effects of mastectomy, patients can opt for immediate or delayed breast reconstruction (BR). 5 Studies have shown that BR can improve body image and psychological health, reduce stigma, and enhance quality of life.4,6,7 However, the decision-making process for BR is complex,8–10 often involving decision conflicts and regret.11–13 This complexity arises partly because patients must navigate decisions about the type and timing of surgery, choice of implants, and factors such as surgical risks, postoperative complications, prognostic uncertainties, and costs. In addition, the surgery involves an organ that symbolizes femininity, closely tied to body image and social integration. 14 Therefore, it is crucial to support patients in making decisions that align with their personal values and preferences.11–13
Shared decision making (SDM) is a process that promotes active collaboration among patients, their family members, and health care providers (HCPs) in making health decisions where multiple medically appropriate treatment options exist.15,16 This process ensures that patients make the most suitable decisions for themselves. SDM can enhance the quality of preference-sensitive decisions, especially when facilitated by patient decision aids (PtDAs).16,17 This model is well developed and widely applied in the field of BR in Western countries. 18 However, the practical implementation of SDM and PtDAs remains challenging. 19 Several scoping reviews on SDM in the breast cancer field have highlighted that, despite increasing evidence of the effectiveness of SDM interventions, there is still limited knowledge supporting its sustained implementation in routine care.19,20 There is a notable lack of exploration into the various factors influencing breast cancer patients’ participation in SDM for BR, particularly at the HCP and organizational system levels.
In China, sociocultural and health care context factors significantly influence patients’ decision making by affecting social expectations related to female roles and family responsibilities. 21 These norms often lead women to prioritize family health over their own, hindering SDM.22,23 Critical yet underexplored factors such as cognitive understanding of decision makers, communication styles, and trust also affect SDM implementation.24–27 For instance, family dominance in decision making and reluctance to question doctors further limit SDM.25,26 In addition, despite increased patient education resources, a lack of decision support tools such as PtDAs impedes effective patient engagement in SDM. 24
Qualitative research enables an in-depth exploration of complexities, providing insights into stakeholders’ experiences and attitudes during the SDM process. Therefore, as part of the development and application research of BR PtDA, this study aims to explore the factors influencing SDM implementation for BR decisions among breast cancer patients from multistakeholder perspectives in the Chinese context. The findings will contribute to addressing barriers and promoting SDM in BR, informing subsequent studies.
Methods
Study Design
This study is part of a larger project that uses literature review, qualitative interviews, and surveys to explore and develop SDM models and corresponding PtDAs for BR in breast cancer patients within the context of China. This article specifically focuses on a qualitative exploration of stakeholders’ perspectives regarding the factors influencing the implementation of SDM in clinical practice for BR decision making among breast cancer patients in China. Previous related studies18,24,28 have been published elsewhere. The study design and analysis adhered to the standards for reporting qualitative research. 29
Study Population and Recruitment
The study was conducted in 3 tertiary hospitals in Beijing, Hebei, and Guangzhou from November 2021 to January 2022. The interviewees included stakeholders involved in the BR SDM process, including patients who face BR decisions after breast mastectomy, breast surgeons or plastic surgeons who perform BR procedures, perioperative nursing staff who care for surgically treated breast cancer patients, and relevant hospital administrators. Specific inclusion and exclusion criteria for participants can be found in Appendix A.
Purposeful and snowball sampling methods 30 were employed to recruit potential subjects with diverse characteristics, including gender, age, occupation, education level, and decision-making experience, ensuring a range of experiences. In addition, recruited participants were invited to recommend other potential participants for the study. Researchers then contacted potential subjects individually, offering options for face-to-face or telephone interviews (due to the impact of the COVID-19 pandemic, face-to-face interviews were not possible for all participants) and coordinating interview times and locations. The sample size for this qualitative study was determined by data saturation. 30
Procedures
In-depth semi-structured individual interviews were conducted either face to face or via telephone. Before the interviews, separate interview guides were developed for patients and HCPs based on a prior literature review by our research team. 18 The patient guide focused on decision-making experiences, information needs, and influencing factors, while the HCP guide addressed roles in SDM, perceived barriers/facilitators, and implementation challenges (see Online Appendix B for detailed questions). Both guides were piloted with 2 participants (data excluded from final analysis).
Each interview lasted 40 to 50 min and was audio-recorded with the participants’ consent prior to transcription. During the interviews, notes were taken to document new concepts or areas needing further clarification or discussion with the participants. Additional notes were made after the interview to reflect on the interview process and the interviewer’s overall impressions.
Given that the primary subjects of this study were breast cancer patients, to ensure the data encompassed a wide range of perspectives and phenomena, HCPs and hospital administrators who frequently engage in SDM for BR were also included as stakeholders and supplementary data sources. The criterion for data saturation in this study was the point at which no new themes emerged across all groups of participants.
Data Analysis
To ensure confidentiality, the participating institutions were labeled as A, B, and C, while patients were designated as P and HCPs/hospital administrators as H. Interviewees were uniquely identified using combinations of these letters and Arabic numerals (e.g., AP1, AH1).
After transcription, 3 researchers (YY, SC, and ZW) reviewed the transcripts to ensure accuracy and consistency with the interview recordings. Following this, thematic analysis 31 was conducted to identify key themes and patterns in the data. Initially, the interviews, conducted by the researcher (Xuejing L), were transcribed verbatim and imported into NVivo 12.0 software for analysis. Two researchers (MM and DY), both adept in qualitative methods and with backgrounds in breast surgery and SDM, independently reviewed and coded the interview transcripts. They applied initial codes to text segments reflecting participants’ narratives, followed by in-depth discussions to categorize the data into emerging themes and collaboratively refine the codes. In cases of differing interpretations, a third researcher (JZ) was consulted to reach a consensus.
Participants were invited to provide feedback on the research findings, and there was no disagreement with the analysis. All analyses were conducted in Chinese, and the final results were translated into English by researcher JZ.
Results
Demographic Information of Participants
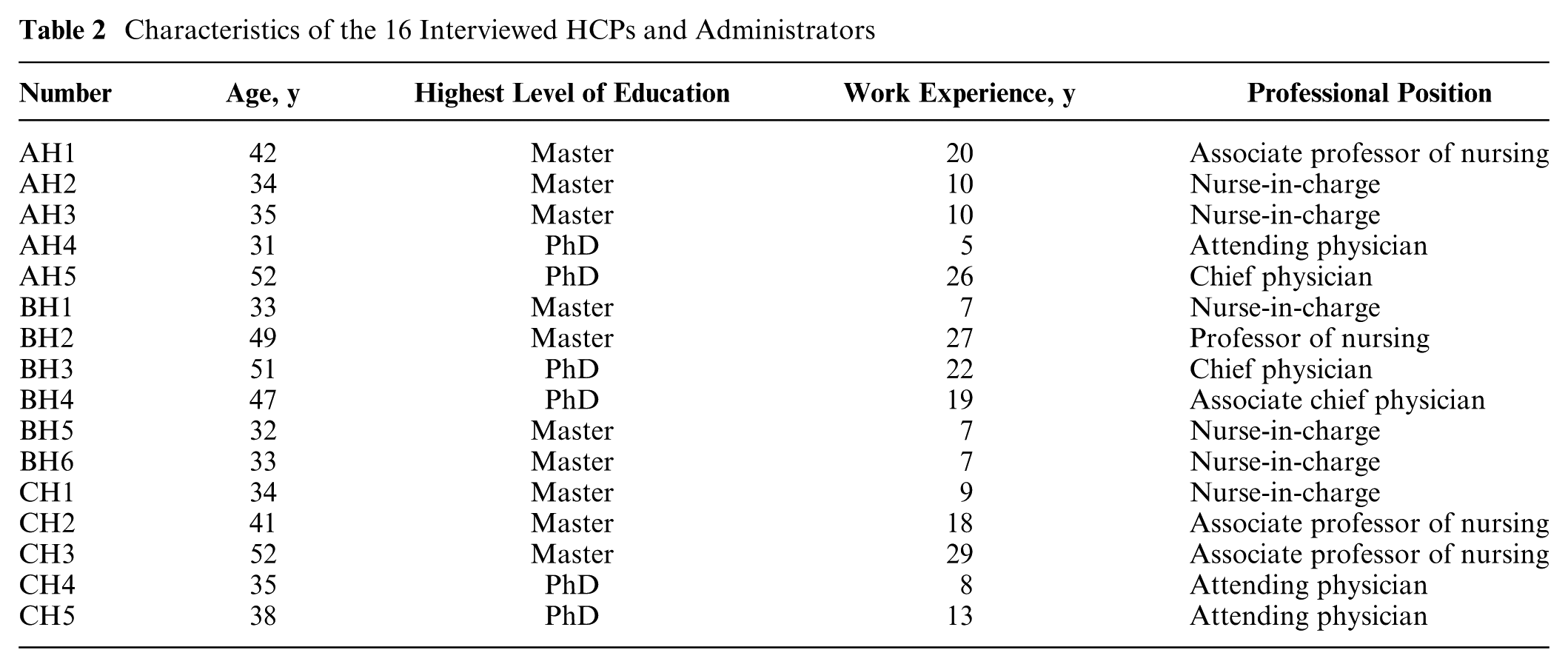
A total of 36 participants from different institutions across 3 regions were interviewed. This group included 20 patients and 16 HCPs, which comprised 6 doctors and 10 nurses. Among the HCPs, 8 also held clinical management positions. All participants who provided consent completed the interviews, with no dropouts reported during the study. Detailed information about the patients is provided in Table 1, and information about the HCPs and administrators is presented in Table 2.
Characteristics of the 20 Interviewed Breast Cancer Patients

BR, breast reconstruction.
Characteristics of the 16 Interviewed HCPs and Administrators
Multilevel Barriers and Facilitators of SDM for BR among Chinese Breast Cancer Patients
Through qualitative analysis of interviews with 36 stakeholders, this study identifies complex interactions across 5 interconnected dimensions: decision-making level, patient level, HCP level, organizational level, and societal level. The following contextualized narrative integrates participant quotes and data patterns to elaborate on these findings.
Decision-making level: Dual challenges of time pressure and complexity
The urgency and unpredictability of decisions posed core barriers. Patients often faced abrupt decision making due to acute illness presentation, as described by “Everything happened so suddenly. After diagnosis, I had to undergo surgery immediately with no time to deliberate” (AP5). Objective medical imperatives further constrained decision space: “Admitted and operated on the same day, I had no choice but to follow the doctor’s advice” (BP8). Unpredictable timing compounded passivity—some patients could not participate in intraoperative BR decisions under general anesthesia: “The doctor decided based on surgical findings, and my subsequent treatment depended on those results” (AP1).
Decision complexity arose from specialized options and social interference. Patients struggled with multiple technical choices (e.g., implant-based v. autologous tissue reconstruction), as noted by “Breast cancer diagnosis confronts patients with complex, nonprescriptive questions, making decisions extremely challenging” (BH1). The social sensitivity of BR amplified external pressures, as revealed by “BR is not just a personal choice—it affects family and social perceptions. Coping with others’ curiosity and pity post-surgery is a psychological ordeal” (BP4).
Patient level: Vicious cycle of physical–mental burden and support gaps
Disease-related physical and psychological effects significantly hindered decision participation. Sixty percent of patients avoided discussions due to psychological stress (“The emotional toll of cancer made me reluctant to communicate with anyone, including doctors” [BP4]), while 35% adopted fatalistic attitudes (“This is my destiny—no decision will reduce my suffering” [BP7]); “It feels predetermined, beyond my control even if I understood the options” [AP1]).
Weak support systems exacerbated dilemmas: emotional neglect from families prioritizing survival over choice (“My family only cares about my survival, deeming BR choices irrelevant” [CP15]), financial strain leading patients to forgo BR for family savings (“At my age, saving for my son’s marriage is more important than understanding BR options” [BP20]), and patients lacking experiential or reliable information (“No one around me has undergone BR, and I receive conflicting advice from patient groups” [BP20]). Cognitive deficits included role ambiguity (“I didn’t know my role—the doctor mentioned BR but didn’t seem to seek my input” [BP7]), low self-efficacy (“My family and I trusted the doctor blindly due to limited understanding” [BP17]), and insufficient grasp of risks/benefits (“I wondered about post-surgery appearance, implant rejection, and long-term complications—but received no clarity” [BP2]).
HCP level: Tensions between role conflicts and competency demands
Role-perception conflicts pervaded SDM practice. Physicians’ authoritative roles and time constraints dominated decision making (“Doctors are too busy to engage fully in SDM, focusing only on core explanations for patients and families” [AH2]), while nurses’ expertise was undervalued (“Nurses detect patient changes first but are often overlooked in SDM by physicians” [AH2]), with hierarchical norms discouraging nurse initiative (“Physicians’ dominance prevents nurses from taking SDM responsibility” [AH2]).
High competency demands underscored training needs: translating medical jargon into lay terms (“Simplifying explanations for low-literacy patients requires skill” [BH2]), tailoring communication to diverse backgrounds (“Patients’ varied life experiences necessitate flexible, context-aware communication” [BH1]), and eliciting values effectively (“Equal opportunity for expression is key, but mastering question design for meaningful insights is a learned skill” [AH3]). Despite challenges, HCPs expressed proactive attitudes (“I encourage patients to ask questions and am eager to expand my knowledge” [BH1]; “Collaborative decision making with physicians, especially in resolving patient difficulties, is essential” [AH2]).
Organizational level: Constraints of process fragmentation and resource shortages
Ineffective team coordination resulted in decision-making gaps. Poor integration between departments, such as outpatient and inpatient services, was evident (“Most breast cancer patients have a short interval from diagnosis to hospitalization, so outpatient departments must participate in decision making to fill information gaps” [BH5]). Ambiguous role delineation among HCPs caused conflicting messages (“Nurses’ health education often contradicts physicians’ instructions—ideally, a tripartite consensus among all stakeholders should be achieved” [AH2]), while nurses avoided proactive involvement due to unclear accountability (“We fear making mistakes or contradicting physicians’ orders” [CH3]).
Systemic support deficiencies included inadequate workflow integration (HCPs reported that SDM was not embedded in routine practice: “Staff workloads are already saturated; SDM can only be promoted if integrated into daily workflows” [AH3]), lack of technological tools (manpower shortages necessitated digital solutions: “Understaffing requires technologies like internet-based videos to alleviate burdens” [BH5]), and insufficient training/policy incentives (HCPs desired communication skills training: “Specific guidance on effective SDM communication is urgently needed” [AH4]). Financial and institutional support remained scarce (“SDM processes would improve if mandated by hospitals” [AH3]; “Media and hospital advocacy could enhance public acceptance of SDM” [AH1]).
Societal level: Implicit impacts of trust crisis and cultural values
The fragility of doctor–patient trust exacerbated risk aversion in decision making. HCPs expressed concerns about medical disputes: “What safeguards exist if patients are dissatisfied with postoperative outcomes following SDM?” (AH2). Traditional role stereotypes simultaneously devalued nurses’ participation in SDM: “Patients trust only physicians, viewing nurses as mere caregivers or even servants” (AH2), while “Patients perceive HCPs through a consumerist lens—‘I pay, so you serve’—rejecting collaborative decision making as equals” (BH6).
Cultural values exerted dual influences: a collectivist survival mindset led patients to prioritize health over appearance, with older generations more inclined to save resources for family members (“Traditional norms emphasize health over aesthetics, particularly among elders who sacrifice personal choices for familial needs” [BH1]). Conversely, HCPs attempted to integrate traditional Chinese medicine (TCM) philosophy—“TCM’s holistic view sees patients as integrated beings. By aligning cultural perspectives and TCM education with SDM, we aim to make patients feel truly heard” (BH3)—demonstrating potential for culturally adaptive SDM promotion.
Discussions
The Complexity of Decision Making and Patient Participation Challenges
The decision-making process for BR in female breast cancer patients is highly complex, shaped by medical factors and personal challenges such as body image issues, quality-of-life concerns, and social discrimination. 32 This study identified that tight decision timelines and the emotional burden of diagnosis hinder SDM. Newly diagnosed patients often struggle with anxiety and fear, affecting their ability to engage in decision-making effectively. 33
In addition, the study revealed that patients often lack understanding and confidence in the decision-making process, largely influenced by Confucian culture and the traditional authoritative role of doctors in China.34–36 This cultural dynamic leads patients to rely heavily on oncologists, often suppressing their own emotions and preferences. Burdened by heavy workloads and limited awareness of promoting patient participation, doctors struggle to provide neutral and comprehensive treatment options or to fully grasp patient values. The study highlights “insufficient decision support” and “insufficient knowledge” as key barriers, emphasizing that timely, comprehensive information is essential for informed decisions—consistent with prior research by Hui Zheng et al. 37 and Wu Qing et al. 38 Early provision of such information enables patients to compare treatment options rationally and choose plans aligned with their values.
Enhancing HCPs’ Role Recognition in SDM
Globally, rigid professional roles and work patterns limit oncologists’ deep engagement with patients, restricting interactions to consultations and routine care.39–41 In contrast, nurses—integral to continuous patient care—are better positioned to understand patients’ needs and psychological states, 42 fostering the growth of nurse-led SDM,43–47 as seen in diabetes care, where such models improve outcomes such as glycemic control, satisfaction, and self-management.48–50
However, our study revealed that traditional Chinese health care stereotypes, such as viewing nurses as “servants,”“doctors’ legs,” or “only capable of administering injections and infusions,” undermine their SDM involvement. Limited recognition of their role and authority hinders patient trust and cooperation in nurse-led SDM, while insufficient doctor–nurse respect and hierarchical constraints (e.g., nurses needing doctors’ permission to contribute to decisions) further restrict their SDM participation, impeding organizational cooperation.
Notably, China’s nursing workforce is evolving, particularly in tertiary hospitals: the proportion of undergraduate nurses is rising, alongside growing numbers of master’s and doctoral-prepared nurses51–53; specialized nurses are also expanding in numbers and professional capacity.54,55 These highly qualified nurses are capable of taking on more complex and specialized care tasks, with the potential to play a more significant role in SDM.
Therefore, efforts should focus on enhancing nurses’ roles in medical decision making through improved social awareness, medical education, and hospital management. For instance, media and public education can highlight their SDM role to reshape stereotypes and build trust. Policies should grant nurses more decision-making autonomy, clarify doctor–nurse collaboration standards in SDM, and establish accountability mechanisms to reduce dispute concerns. Such strategies can elevate nurses’ SDM role and promote its clinical integration.
Integrating SDM into Clinical Workflows
Given China’s large patient population and limited health care workforce, it is crucial to strike a delicate balance between meeting the demands of SDM and addressing the realities of daily patient care. This study highlights that ensuring the convenience of SDM should be a key organizational priority, particularly by integrating SDM into existing clinical workflows.
Research indicates that health care institutions should prioritize reconfiguring clinical workflows to prevent SDM implementation from excessively increasing staff workload, which could compromise efficiency and the quality of patient care. 56 In addition, using decision support tools (such as online platforms, personal digital assistants, and multimedia resources) can effectively alleviate personnel workload 57 —a key consideration given China’s medical resource constraints. These tools enhance and simplify complex medical information for patients via streamlined transmission and personalized education and improve the patient experience.57–59 Interviews indicate urgent provider demand for such tools, underscoring the need for their development and full utilization.
Integrating SDM is an innovative step for organizations yet to implement it, with success requiring financial and policy support—including monetary incentives, expanded human resources, and policy guidance. In China’s context of top-down reform, such supports are foundational to SDM’s smooth implementation. 60 Policy makers and hospital administrators should introduce incentive measures, combining “encouragement” and “pressure” to drive successful SDM adoption and enhance overall medical service quality.
Furthermore, the interview results highlight HCPs’ urgent need for SDM-related training, echoing the calls of Coughlin et al. 61 Therefore, health care institutions planning to implement SDM should incorporate courses on communication skills, patient engagement techniques, and SDM ethics into HCPs’ onboarding training and continuing education.62,63
Cultural Influences on SDM in China
Influenced by traditional Chinese cultural philosophies of Confucianism, Buddhism, and Taoism, Chinese life perspectives emphasize enduring life’s ordinariness and hardships and facing death with resilience and perseverance. 64 For many Chinese, encountering illness often entails bearing burdens and confronting death with fortitude, 65 as captured in a bestselling book: “The word ‘alive’ in Chinese is imbued with strength. Its power does not come from shouting or attacking, but from enduring the responsibilities that life imposes on us, enduring the happiness and hardships, the boredom and ordinariness.” 66
This resilience manifests in patients prioritizing family interests over personal ones, particularly financially—avoiding additional financial burdens on families while safeguarding health. Consequently, many patients choose to endure the physical and psychological impacts of surgery, autonomously forgoing considerations of BR decisions. Some older patients, viewing breast cancer as an inevitable hardship with fatalistic attitudes, consciously disregard BR options. Clinically, HCPs should identify such patients and use culturally appropriate methods to facilitate their decision-making involvement.
The interviewees in this study noted several key capabilities HCPs need for effective SDM: translating specialized language into lay terms; conducting personalized care dialogues; understanding patient preferences, values, and beliefs; demonstrating insight into medical care; and judging when to initiate SDM. In the clinical context of China, these abilities can be prioritized by transforming existing competencies among Chinese HCPs rather than separate cultivation.
In China, patient seeking and health care delivery are deeply influenced by the philosophical and cultural underpinnings of TCM. 67 TCM philosophy emphasizes the integration of subjective and objective aspects, upholding the unity of nature and humanity. 68 This holistic perspective views patients as whole individuals within their environment, not just symptom collections, encouraging HCPs to communicate thoroughly with patients and respect their perspectives. 69 Within the cultural backdrop of TCM, the concept of “;仁” (benevolence) can be interpreted within a broader SDM framework, and its core principles such as “patient-centeredness,”“harmony between nature and humanity,” and “medicine as an art of benevolence” reflect the spiritual and psychological needs of Chinese patients seeking medical care. 70
Therefore, the promotion and training of SDM among HCPs in China should integrate SDM with TCM culture. Aligning the “talk” process of SDM with TCM’s diagnostic methods of “looking, listening, questioning, and palpating” can foster a culturally sensitive exploration and adaptation of the SDM model with Chinese characteristics, strengthening contemporary HCPs’ identification with TCM culture.
Cross-Contextual Comparisons and Generalizability Implications
While contextualized within China’s health care and cultural settings, this study offers insights for cross-cultural discussions on SDM in BR. China’s family-centered decision making—where family consensus often influences treatment choices—contrasts with the individual autonomy-driven frameworks dominant in Western SDM research. 71 This distinction highlights how Confucian-based collectivist cultural norms shape patient engagement in decision-making processes, 72 suggesting that SDM interventions in similar contexts may need to integrate family involvement as a core component rather than focusing solely on individuals.
In addition, the analysis of systemic barriers to SDM (e.g., time constraints, standardized protocols) enables comparisons of centralized versus decentralized health care systems. In China’s hierarchical medical structure, SDM is constrained by provider workloads and top-down practice guidelines, whereas Western systems may face challenges related to fragmented care coordination or variable insurance coverage. 73 These observations contribute to a global dialogue on tailoring SDM tools to institutional realities, such as developing structured communication templates for time-limited consultations or enhancing interdisciplinary training to promote SDM across diverse practice environments.
By documenting these context-specific dynamics, this study enriches the international SDM literature with a non-Western perspective on how cultural values and health care infrastructure mediate patient–provider interactions. The insights are particularly relevant for regions with collectivist traditions or centralized health care models, as they highlight the need for SDM frameworks that balance evidence-based guidance with local sociocultural norms. This bridges gaps between universal SDM principles and context-specific applications, fostering more inclusive and effective decision-making practices globally.
Limitations
The limitations of this study primarily stem from the narrow sample source, which includes only 3 regions in mainland China. This geographic and cultural selection bias may affect the generalizability and representativeness of the research findings. To enhance the study’s breadth, future research should incorporate samples from more regions, encompassing stakeholders from diverse geographic, cultural, and social backgrounds. In addition, due to data acquisition constraints and the scope of the study, family members of patients were excluded. However, influenced by Confucianism and collectivist culture, families play a significant role in medical decision making in China. Patients and their families are often considered a decision-making unit, particularly evident in SDM processes. Future research should include family members in the sample to explore their influence in SDM, analyze the interactive mechanisms between patients and their families in decision making, and delineate their roles in the process.
Conclusions
This qualitative study provides an in-depth exploration of the facilitators and barriers to implementing SDM for BR among breast cancer patients within the Chinese context. Our findings highlight several critical factors influencing successful SDM implementation, including enhancing patients’ self-efficacy, addressing their information needs, improving HCPs’ role recognition and SDM-related competencies, strengthening medical team coordination, and ensuring the convenience of SDM. The results also underscore the unique cultural nuances that shape SDM processes in China, emphasizing the need for HCPs to understand and respect patients’ cultural perspectives rooted in Confucian, Buddhist, and Taoist philosophies.
Notably, our study suggests an innovative approach to SDM implementation in China: integrating TCM diagnostic methods with SDM practices. This integration could potentially create a culturally tailored SDM model. Future research should focus on developing and evaluating culturally adapted SDM interventions that incorporate these facilitators and address the identified barriers.
Practice Implications
To enhance the implementation of SDM in BR for breast cancer patients in China, health care institutions should integrate SDM into clinical workflows through standardized protocols, such as embedding decision checklists in electronic health records and allocating dedicated 30-min consultation slots with PtDAs (e.g., interactive 3-dimensinoal models) to enhance patient comprehension. Culturally tailored practices are critical, requiring providers to use structured family consultation guides that align with Confucian values, balancing patient autonomy with family consensus via scripts for addressing intergenerational preferences. Training programs should emphasize role-playing for empathetic communication and ethics workshops grounded in Confucian “仁” (benevolence) to harmonize decision-making dynamics. Systemically, incorporating SDM into tertiary hospital accreditation criteria ensures institutional accountability, while health insurance coverage for PtDA development and National Health Commission–established SDM training funds would financially sustain capacity building for HCPs. These integrated strategies—merging protocol standardization, cultural adaptation, and policy-backed resourcing—will anchor SDM as a sustainable, patient-centered practice in China’s health care system.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683251386466 – Supplemental material for Barriers and Facilitators for Shared Decision Making in Breast Reconstruction among Stakeholders in the Chinese Context: A Qualitative Study
Supplemental material, sj-docx-1-mpp-10.1177_23814683251386466 for Barriers and Facilitators for Shared Decision Making in Breast Reconstruction among Stakeholders in the Chinese Context: A Qualitative Study by Xuejing Li, Meiqi Meng, Yiyi Yin, Dan Yang, Junqiang Zhao, Xiaohua Li, Xiaoyan Zhang, Liu Han, Sihan Chen, Ziyan Wang, Pei Xue and Yufang Hao in MDM Policy & Practice
Footnotes
Acknowledgements
We extend our sincere gratitude to all the participants, including the patients, doctors, nurses, and hospital administrators from Beijing, Hebei, and Guangzhou, who contributed to this study. Their insights and experiences were foundational to the completion of this research. Meng Meiqi acknowledges the support of the China Scholarship Council program (project ID: 202406550037).
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from Basic Research Grant Program for 2023 at Beijing University of Chinese Medicine (grant No. 2023-JYB-XJSJJ019). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethical Considerations
Ethical approval for this study was obtained from the Medical Ethics Committee of Beijing University of Chinese Medicine, with approval number 2021BZYLL0307.
Consent to Participate
All participants provided written informed consent to participate in this study.
Consent for Publication
Not applicable.
Data Availability
The data supporting the findings of this study are available from the corresponding author, Yufang Hao, upon reasonable request. Access to the data will be granted in accordance with ethical guidelines and participant consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.