
Abstract
Highlights
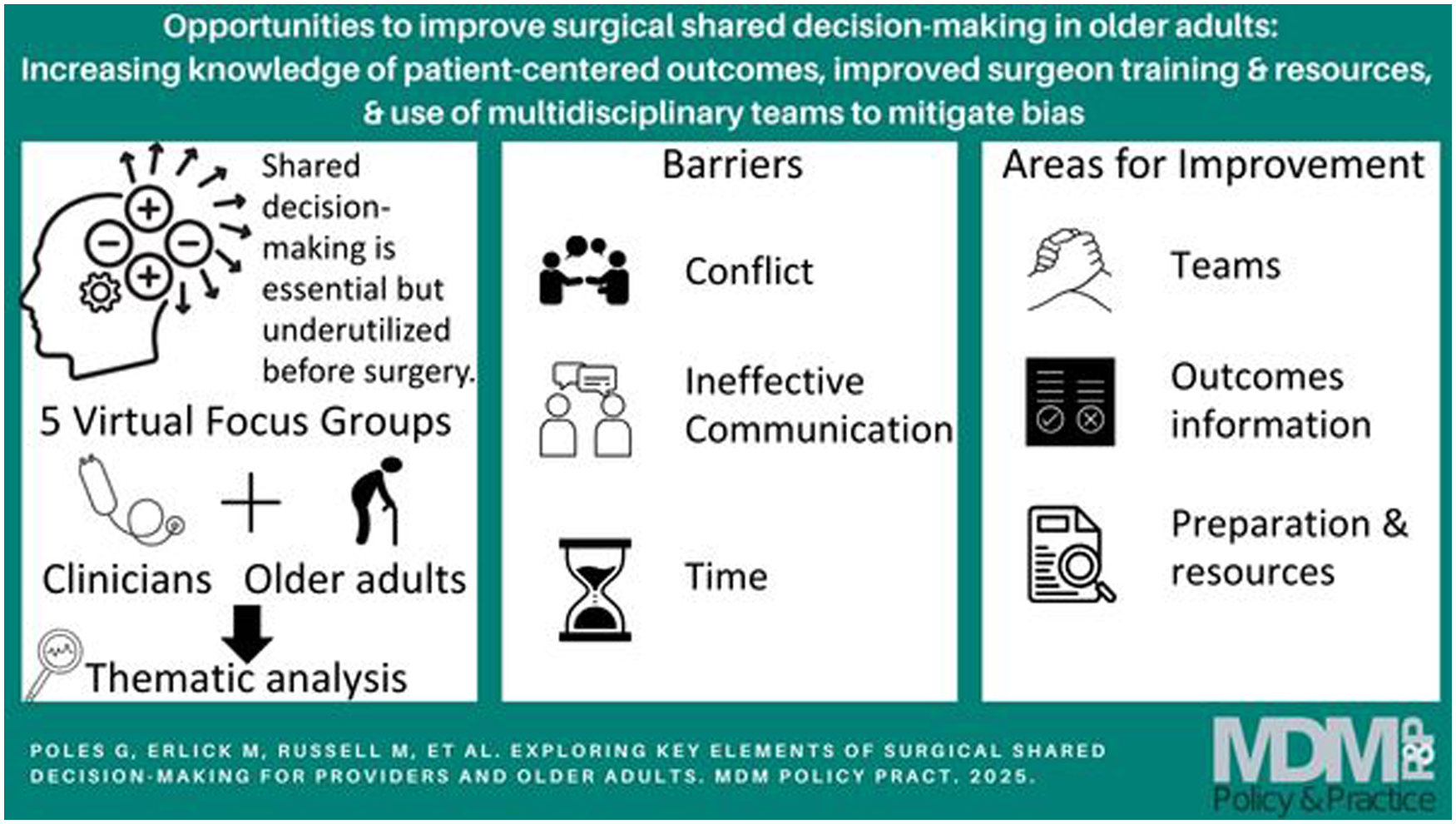
Critical components of shared decision making (SDM) identified in this study include understanding patient values, building trust, understanding the patient’s baseline function, and defining possible treatment outcomes.
Specific components of SDM in older adults include navigating companions to conversations and the challenges of navigating potential postoperative changes to cognitive or physical function.
Possible areas to improve SDM include improved dissemination of SDM resources; the importance of communication skills and empathy and an emphasis on additional training for this, particularly for trainees; improved engagement of patients in the SDM process; and using other care team members such as palliative care and social work when appropriate.
Older adults (≥65 y old) are high utilizers of surgical services, which is increasing with the ongoing rise in this population. 1 There is an urgent need to improve shared decision making (SDM) in this population to ensure goal-concordant care. 2 Increasing age is associated with a higher comorbidity burden, increased frailty, increased rates of depression, and less physiologic reserve, which puts this population at higher risk of postoperative mortality and morbidity.3–8 There are also unique long-term postoperative risks in this vulnerable population, such as functional and cognitive decline, which can affect survival and quality of life. 9 The willingness of older adult patients to undergo certain treatments may be heavily dependent on the burden of treatment and its impact on quality of life, with a focus on avoidance of disability rather than additional years of life.10–12 These factors make SDM especially important but inherently more complex in this population.
While there is a growing interest in SDM in surgery and development of various strategies to promote it, it is not clear if it has been more successfully incorporated into clinical practice over time. 13 For example, patients and providers feel that SDM is important and often desire to engage in this process but have differing views of what constitutes SDM. 14 Preoperatively, it is predominantly utilized by surgeons when they feel that surgery is not beneficial to the patient, whereas it underutilized in other settings.13,15–20 However, it is underutilized in preference-dependent surgery, when there may be tradeoffs that are important to patients’ quality of life.13,18,20 In addition, surgeons often focus on assessing risk and setting expectations with patients and exclude other key components of the SDM process such as inviting active participation, goal setting, or “teach back.”13,20,21 Despite this, patients often report higher levels of SDM than surgeons do in objective SDM measurements, which suggests a lack of patient understanding of the process that may affect patient engagement. 14 Finally, who should participate in the SDM conversation may be different in older adults, where having family or caregivers present may be more impactful, but this is inconsistently done. 22
Variations in SDM perception between patients and provider subjective measurements and more objective measurements may be due to baseline understanding of what constitutes SDM as well as differing priorities of what is important in these interactions. Examining baseline understanding, priorities, knowledge of existing tools and frameworks to promote SDM, as well as barriers and facilitators to effective communication in this population is key to developing next steps to improve SDM. Our aim was to characterize these components specifically in the context of older adults considering surgery from provider, patient, and caregiver perspectives.
Methods
Study Design
Semi-structured focus groups were conducted with important stakeholders in older adult SDM at a single institution. They occurred from February to April 2022, were 90 to 120 min in duration, and were completed via Zoom and recorded (audio and visual). Each focus group was led by a primary moderator (M.E.) who had prior experience moderating focus groups and a secondary moderator (G.P.) to help facilitate and take notes. The focus group guide was informed by a review of existing frameworks for SDM in older adults15,21,23–25 and identified gaps in the surgical SDM process in older adults.13,14 The literature review demonstrated gaps in the perception of successful SDM between providers and patients,14,26 lack of understanding of issues of older adults specifically in surgical SDM, 27 and variable uptake of existing SDM tools and frameworks by clinicians. 28 This was exploratory research to understand the surgical SDM process and priorities, use of tools to support this, understanding of issues specific to older adults, and barriers and facilitators of effective SDM in this population from provider, patient, and caregiver perspectives.
A preliminary focus group guide was created and then refined through a focus group with surgical residents (Supplement 1). Sample size was determined by an estimated 3 to 6 focus groups to reach saturation. 29 Providers were identified through the primary investigator’s’ (G.P.’s) clinical network and snowball sampling at a large academic teaching hospital and then recruited via e-mail. Only providers who worked in a surgical subspecialty or directly with older adult (≥65 y) perioperative patients were included. This included providers at multiple levels (surgical residents, advanced practice providers [APPs], and physicians) and across specialties (surgery, intensive care, geriatrics, palliative care/ethics) to obtain varying perspectives. Providers were excluded if they did not work directly with perioperative older adult patients on a regular basis. Patient representatives were recruited through the Patient Advisory Council (PAC) at a large academic teaching hospital. The research team presented the background and premise of the study at a regularly scheduled PAC meeting, and patients volunteered to participate. Patient participants had to have an interaction with the medical community for surgical SDM as an older adult patient (≥65 y) or as a family member to an older adult. Two provider participants declined to participate due to time reasons. Once recruited, all members participated in a focus group. The primary moderator (M.E.) had minimal interaction with any participants prior to the focus groups. The study rationale was provided to participants prior to recruitment, but no personal information about study personnel was given.
A total of 5 focus groups were conducted, with a total of 24 participants. This included surgical residents (5), attending providers from various subspecialties (2 surgeons/intensive care unit [ICU] providers, 2 geriatricians, 1 palliative care provider, 3 surgical APPs), and 11 patients/caregivers (see Table 1). Each focus group included between 3 and 9 participants (average = 5), and no repeat focus groups were completed. Verbal consent was obtained from participants. The study was approved by the University of Rochester Institutional Review Board (No. 00007067).
Descriptive Characteristics of Focus Group Participants (N = 24)

ICU, intensive care unit; NA, not applicable.
Thematic Analysis and Model Development
Focus groups were transcribed using Landmark automated software and reviewed for quality assurance using video recording. Transcripts were not returned to participants for comment. We then conducted iterative, inductive, classic thematic analysis of transcripts using grounded theory. Analysis was completed using Dedoose version 9.0.86 software (2023). An initial round of coding was conducted by 2 researchers (M.E., A.Z.).29,30 The 3 researchers (M.E., A.Z., and G.P.) then met; the coded data were reviewed and discussed, and the codes were organized to develop a preliminary codebook. All had prior experience with qualitative analysis. The transcripts were then reread and coded using a focused coding approach (M.E., A.Z.), and any discrepancies of how to code data were resolved as a group over multiple meetings to establish consensus. Participants did not comment on findings. Thematic analysis was initially completed with 4 focus groups based on sample size estimates. There was significant heterogeneity within the themes among the 4 initial focus groups. We proceeded with 1 additional focus group, but because no new themes emerged in this focus group, we concluded that thematic saturation was reached. 31
Results
A total of 6 major themes emerged: importance of SDM, components of SDM, barriers to SDM, preparation for SDM, age-specific considerations, and suggestions for improvement.
Importance of SDM
All participants felt that surgical SDM was important to avoid nonbeneficial care, establish a collaborative relationship with the patient and other team members, and respect the patient’s wishes. Both patients and providers felt that understanding patients’ wishes was crucial to fostering trust and collaboration in the therapeutic relationship.
It’s not a caregiver to . . . recipient, but it’s a partnership, it’s like a collaboration . . . whatever kind of term it should be viewed as an equal . . . trust is such a super important word. (Caregiver, ID:21)
Patients emphasized wanting to be active decision makers, while providers stressed the importance of developing a relationship with patients, ensuring patient understanding of treatment, and collaboration within the care team.
Everyone’s so different, both kind of how they’re gonna take the surgery and how they’re going to handle the afterwards and their opinions about trust and kind of health care and doctors and everything . . . I think we’re focusing the conversation about the surgery here, but the surgery is just a start. (Caregiver, ID:21)
Providers saw SDM as a way to prevent nonbeneficial care and discussed the importance of assessing patients’ values and aligning surgical recommendations with them. They also discussed the risk of prioritizing family preferences over personal values, particularly in older adults and patients unable to participate in SDM.
We have the families that say . . . let’s do everything and then at the end, when the patient was in ICU with all these complications, the patient was really cursing out the surgeon. It’s like, everybody lied to me, that I was gonna be okay, and everybody just pushed me toward this point, and it should not have been like this. (Resident, ID:2)
Components of SDM
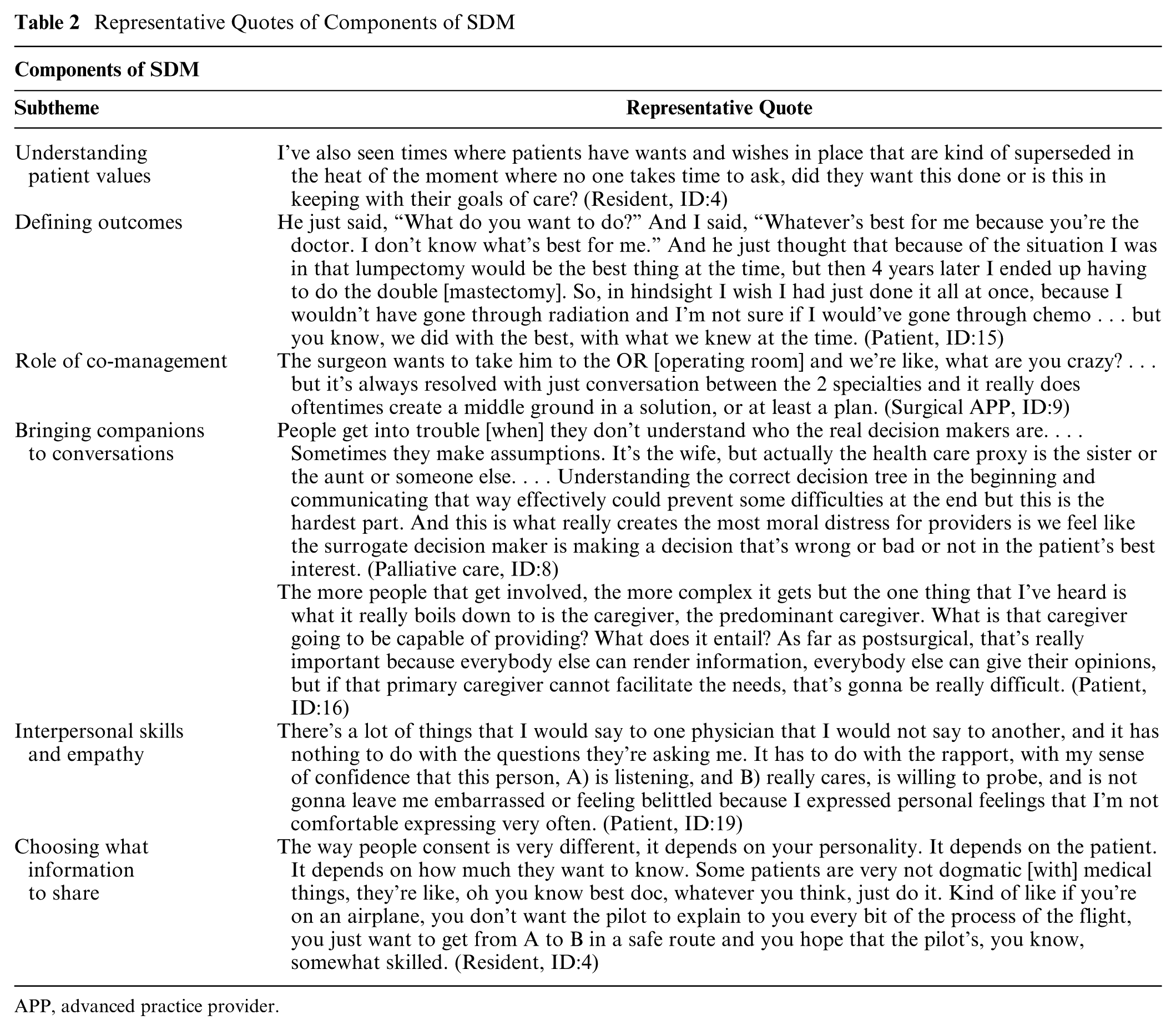
Components of SDM discussed included understanding patient values and baseline function, defining outcomes, bringing companions to conversations, the role of co-management, interpersonal skills and empathy, and choosing what information to share (Table 2).
Representative Quotes of Components of SDM
APP, advanced practice provider.
Key elements of SDM across both groups were understanding patients’ values and baseline function, particularly in older adults. This was seen by providers as especially important when things did not go well postoperatively.
[You] spent your 10:00 PM until 3, 5, and 5 in the morning trying to fix the patient. You’re now well invested in that patient and I think it’s a little harder to step back and say, on day 5, what are we doing here? (Surgical APP, ID:8).
Patients valued providers’ willingness to develop an understanding of their values and felt that this was as important preoperatively as discussing things such as functional limitations and pain tolerance. While identifying patient values was a key first step, defining outcomes was a necessary next step.
Patients recognized this as important for making an informed decision about care and especially planning for caregivers and other needs. Providers discussed the difficulty of discussing surgical interventions when outcomes were uncertain, particularly in emergent settings with limited time and resources, and that discussing palliative care options in these situations was especially difficult. As a result, providers often felt compelled to offer surgical treatment unless certain about a negative outcome.
You want people to offer people palliative care and . . . and not see that as a failure, but you also don’t want to have this nihilistic view . . . the bowel obstruction cases, like the most classic example, right? You get this a 90-year-old person or the bowel obstruction and you know what, it may be a 20-minute surgery and you cut 1 adhesion and that’s it. You don’t know. (Surgeon, ID:10)
The role of co-management was highlighted as one way to mitigate uncertainty and navigate complex situations. While this could result in conflict between teams and sometimes with families, this often led to more comprehensive plans for patients. In addition, in situations where surgery was not appropriate, it allowed for other teams to discuss noncurative options. Not offering surgery was seen as an important first step to give space for patients and families to engage in discussion about these other treatment options.
We need people to kind of have that really hard realization that a surgical procedure is not going to be something that’s on the table anymore. They need to have that door kind of close in order for them to have a good discussion with me about what can we do, you know, a more of a symptomatic basis because actually there’s a lot we can do. (Geriatrician, ID:11)
Providers generally viewed companions as crucial for ensuring patients understood information, especially when patients had cognitive impairment. As such, there was considerable overlap between bringing companions to conversations and the code category age-specific considerations. However, opinions on involving companions in the SDM process varied among providers. While providers emphasized the role of family members in helping patients see the larger picture, others expressed concerns about misalignment between the patient’s values and the families’ desires.
In more elderly populations . . . it suddenly becomes the rest of the family making these decisions for the patient. And they’re willing to go along with those decisions, even if that’s not necessarily what they want or value. . . . I think . . . having a family member can be helpful there, but it can also be a hindrance in a way. (Resident, ID:1)
Similarly, patient participants felt that there were both pros and cons of companions to conversations. Multiple patient participants agreed that having a companion present to receive information is beneficial as companions may ask questions the patient may be unwilling to ask and provide insight into the patient’s functional abilities, problem-solving strategies, or the abilities and limitations of the patient’s caregivers. However, some expressed uncertainty about whether this was appropriate and worried that the presence of family members might disrupt the patient–provider relationship. One patient stated, “I felt very uncomfortable with everybody else in my family asking questions. This bothered me because I thought it would affect the attitude of the physician” (ID:19)
All groups stressed the importance of good communication skills and empathy. Patients emphasized these as important to establish trust and facilitate SDM, while providers highlighted their significance in understanding patient goals and values.
You might not actually know who they are, [but] you might know their goals . . . and I think that makes a big difference. If you have some, some sort of stepwise relationship with the patient . . . if you can meet them over a few settings and then, then you really get the whole consent framed, whether or not this is the right thing for the patient. (Resident, ID:4)
Providers discussed other important aspects of effective communication such as the balance of providing enough information for informed decisions while not overwhelming patients with excessive details, in particular, the importance of offering only options that are in line with patient values or reasonable outcomes. Non-surgical providers discussed the general strategy of avoiding statistics, such as a “1% chance of survival” and terminology such as “doing nothing,” which often result in patients and families pushing for interventions that are nonbeneficial because of the perceived alternative. In these instances, phrases to communicate empathy such as “I wish” and “I worry” statements, the importance of nonverbal communication, acknowledging the limitations of medicine, and staying goal oriented were helpful.
I think you . . . just to speak in a very simple language, which is appropriate . . . but you really have to adjust your language appropriately to the patient. So that’s probably the most important thing . . . in terms of understanding what that surgery is going to be about. (Resident, ID:3)
Patients highlighted their reliance on physicians to relay important information but varied in their desire for detailed information versus just relying on physician expertise. Many expressed wanting comprehensive information about postoperative outcomes, including short- and long-term side effects, but they also stressed the importance of other outcomes such as caregiver needs, difficulties eating and sleeping, changes to mobility and independence, and side effects associated with required medications that had a big impact on their quality of life but were not discussed preoperatively.
When I watched all that [preoperative educational video], it didn’t tell me I was gonna have all those tubes and grenades and 3 months’ worth of tube feeding . . . I didn’t know that. . . . That was actually worse than the operation. (Patient, ID:22)
In addition, patients expressed not knowing what was okay in SDM discussions—whether they could record information or bring someone with them. Even when patients desired to participate in SDM, they often wanted explicit permission to engage in this process.
It’d be nice to have permission . . . to have someone with you, maybe you hadn’t thought about that, you might want to think about some questions and have them written down . . . you might wanna think about bringing someone to hear things or bring a recording or just having that permission. (Patient, ID:15)
Preparation for SDM
Although both groups discussed patient preparation, patient participants were primarily concerned with provider training and discrete resources available to patients, while providers appeared to be most concerned with discrete resources for the provider as well as peer modeling and culture (Table 3).
Representative Quotes of Preparation for SDM

CT, computed tomography; SDM, shared decision making.
Patients relied on Google or materials provided by physicians for preoperative preparation. Patient believed their preparation could be improved by 1) providing a standardized checklist during the SDM process, suggesting that such a checklist might “provoke other concerns that [the patient] might have” (patient, ID:8) that they would otherwise be unaware of, and 2) providing written information on the risks of surgery and potential short- and long-term side effects of surgery. This written information could come in the form of charts, graphs, and figures and be written in simple language, which would improve its accessibility. Providers were primarily concerned with gathering the patient’s clinical information, particularly with increased access to medical information. In addition, they felt it was important to ensure that a surrogate decision maker or companion was available when discussing their patients’ care, which was especially salient in older patients with cognitive decline as well as when discussing potentially difficult information. Most surgeons occasionally use resources such as the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) risk calculator, but mostly only if patients were perceived to be high risk. Nonsurgical providers found online communication training resources helpful, such as those offered by the Center to Advance Palliative Care.
Although providing training in SDM emerged in all provider focus groups, opinions on the feasibility and benefits of providing such training were mixed. All providers stated that they mostly learned this through peer modeling and feedback as trainees. However, the residents mentioned that supervision of trainees was very dependent on the attending surgeon and their senior residents. One provider stated, “I think that the comfort with consenting patients just comes with time. There is no crash course which can speed it up” (resident, ID:3) Another, however, argued for a “20-minute formal session . . . during intern orientation” (resident, ID:2) to provide interns with a framework with which they could approach patients. Generally, providers agreed that nonemergent settings are a more appropriate venue for residents to learn how to consent patients.
Barriers to SDM
Reported barriers to SDM included provider skills, cultural and structural barriers such as time and power dynamics, patient understanding of information and health literacy, and conflict between team members or family members (Table 4).
Representative Quotes of Barriers to SDM
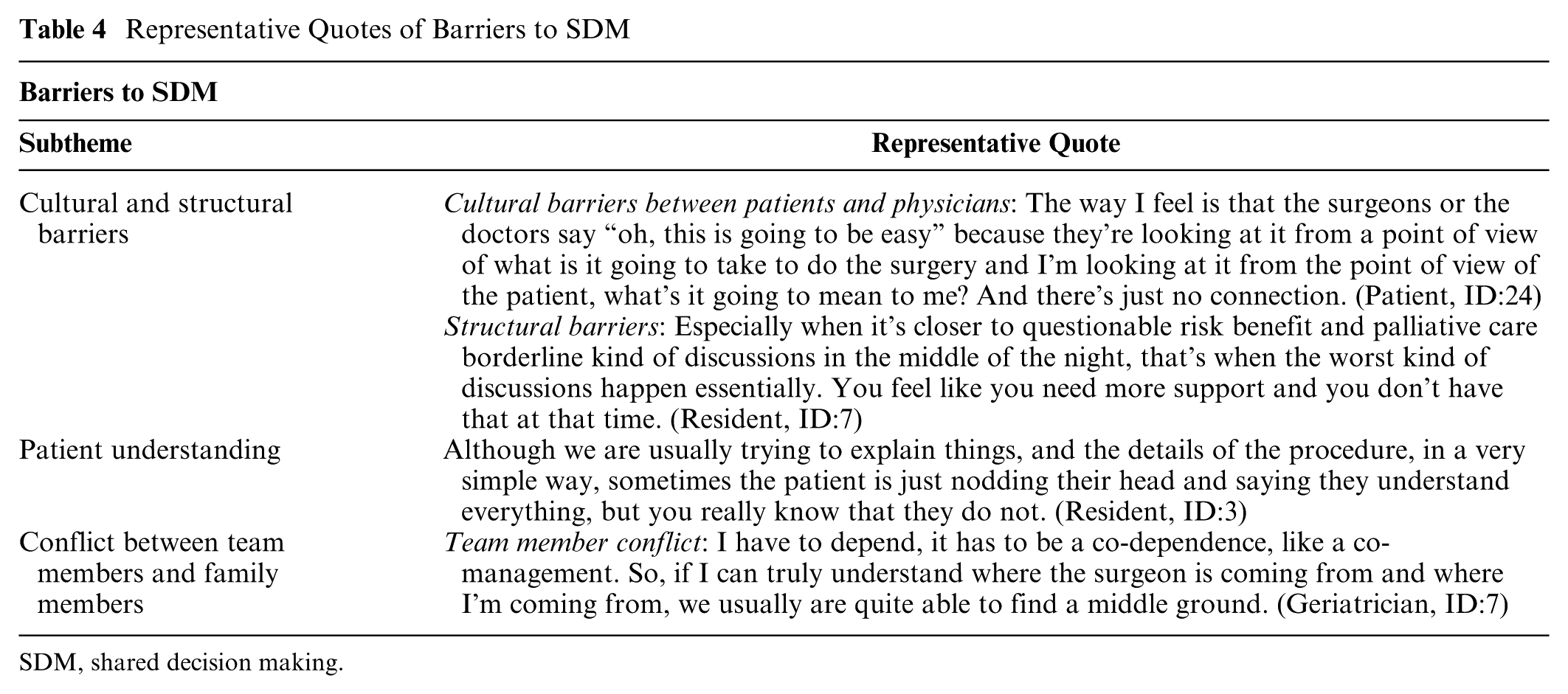
SDM, shared decision making.
Patients acknowledged reliance on the physician to relay the important information and the importance of a physicians’ ability to engage with patients on a personal level to allow for open communication. Patients felt that this skill was innate and not able to be taught, particularly with respect to empathy.
It’s like when you meet a friend, how do you feel good about this person? When you feel good, you’ll open up, you’ll talk, you’ll express your feelings. When you don’t feel good, you get suspicious, you get quiet, you don’t want to expose yourself and all the [SDM tools] in the world aren’t gonna change that. So I think there’s a real personal thing in this thing and I don’t know how to put metrics around that, but I think it’s real. (Patient, ID:19)
Providers acknowledged that provider skill was important, but surgeons reported that this was mostly learned through clinical experience. Very few had explicit training (see suggestions for improvement).
Patient participants were less likely than providers to discuss either cultural barriers or structural barriers to SDM, and when they did, they discussed emotional stress hindering comprehension and the impact of time limitations on the SDM process. Both groups discussed conflict within the SDM process, including conflicts with other medical teams or family members/caregivers, as a significant barrier. Patients also brought up worries about confusion and disruption to the patient–provider relationship if family members joined preoperative discussions.
I was concerned that too many people would be asking too many questions and creating a nonpositive situation with the surgeon, that it would be creating conflict both within our family and with the surgeon. And also I was much more concerned that we were bothering the doctor and that we were, you know, putting ourselves in a position that was not the best for the patient. (Patient, ID:19)
Providers discussed concerns about the patients’ ability to comprehend information based on emotional state, cognitive deficits, and health literacy, which may limit understanding of crucial information. They also discussed the implications of time and staffing shortages, especially during night shifts for nonelective surgery, on the ability to engage in thorough SDM, the urgency of a patient’s condition limiting SDM, and concerns about litigation. Specifically, some providers felt pressured to offer surgical options even when they had a high risk of morbidity and mortality and did not seem to align with a patient’s values, particularly for emergent surgery. Providers noted that time constraints affect not only SDM quality but also teaching SDM effectively.
I have some trepidation about trying to make these conversations, these decisions, about these sometimes life and death decisions with somebody you’ve just met, and under time pressure. (Surgeon, ID:12)
Age-Specific Considerations
Age-specific considerations were prominent across all focus groups, with patients concerned about informing caregivers and family members about surgical procedures and potential caregiver burdens (Table 5).
I was trying to go through all the what ifs, but then I didn’t realize what could happen to me as the caregiver because I’m the only one. . . . So I didn’t realize that he could like hurt himself, you know, overnight. And I wouldn’t be aware . . . I can’t stay up all day and all night I realized later, . . . I’m gonna need someone to help me because this is gonna be a 24/7 job taking care of him. (Patient, ID:20)
Representative Quotes of Age-Specific Considerations

APP, advanced practice provider.
Providers focused on obtaining consent from older adults, particularly those with cognitive decline, and managing how functional issues might affect outcomes. Understanding functional outcomes after surgery was seen as particularly challenging to predict in older adults. In addition, providers discussed difficulties navigating the desires of the patients’ family members while simultaneously honoring the patients’ goals of care and how it was essential to clearly identify surrogate decision makers prior to surgery. Again, co-management was brought up as a way to help when there was uncertainty about patient outcomes in complex situations and to help with nonsurgical treatment options.
There was significant overlap between age-specific considerations and importance of SDM, considerations for SDM, and barriers to SDM, and additional points specific to SDM in older adults are detailed in those sections.
Suggestions for Improvement
Suggestions for improvement fell into 3 major categories: communication skills training to providers, information provided to patients, and involving caregivers or surrogate decision makers in the decision-making process (Table 6).
Representative Quotes of Suggestions for Improvement

ICU, intensive care unit.
The importance of communication skills and empathy in the provider was highlighted by all groups. However, patients often felt that physician demeanor and empathy may be innate and unable to be taught. The patients’ main focus on improving physician communication was getting them to understand the patient experience. Physicians, however, felt that critical components of communication were teachable.
Teaching physicians about how to ask open-ended questions, like, what are you hoping for from this visit? Like what, what, what did your primary tell you? Or, or so something like that kind of just . . . set those expectations early on . . . that can be really helpful. (Geriatrician, ID:11)
Providers suggested structuring this into residency or medical school education whether as a rotation with palliative care, teaching communication skills, or even just education on SDM frameworks. It was felt that starting this education earlier was important and that medical school or residency was the appropriate time while habits were being formed.
You won’t have the medical knowledge and you won’t understand it from day one, but at least having some idea of a framework of how these discussions should go or could go is important to have. And as time goes on, then you get all those details to fill in the framework. So you can actually have a more meaningful discussion, but I think no matter how we try and structure residency, we’ll still be having interns going to consent people. They need something in their toolbox, instead of saying, you know, we’re gonna send you to clinic twice a week for a year and then you’ll figure it out. (Resident, ID:1)
Other suggestions from providers included better dissemination of existing communication resources to surgeons, templating the SDM process, and using other care team members such as palliative care and social work when appropriate.
Both groups felt that encouraging engagement in the SDM process was important. Various suggestions from both groups to encourage patient engagement include providing a space for patients to write down questions and offering information in accessible written formats, including simple charts. In addition, patients had a lot of questions about what was appropriate in these situations and stated that having explicit instructions about who they should bring to appointments, being welcomed to ask questions, and being allowed to record information as important steps to invite engagement in SDM (see also components of SDM). Patients also felt some of this could be templated into a patient checklist to guide the process. It was agreed by all groups that a surrogate decision maker should be identified for every older adult patient and that they should be present during any critical provider–patient communication.
Discussion
This is an exploratory, qualitative study examining how patients, caregivers, and providers define SDM and their knowledge of existing tools and frameworks to promote it as well as barriers and facilitators to effective communication in this population and suggestions for improvement. Our main findings further characterize the complexity of surgical SDM, particularly in older adults and emergent settings, as well as minimal structured training or knowledge of existing resources for this among surgical providers. Novel findings include critical components of the SDM process from the perspective of older adults and caregivers and a desire to be explicitly given permission to engage in the process. These findings highlight some potential novel areas to improve surgical SDM in this vulnerable population.
While both patients and providers agreed that SDM is important, they reported different reasons for this and different key components, which was a novel finding. While both patients and providers felt that defining outcomes was important in this process, patients focused more on specific concerns such as the need for caregivers and short- and long-term side effects of surgery (e.g., difficulties eating, sleeping, mobility, and potential changes to quality of life) rather than the surgeon-defined important outcomes that focus on early postoperative complications. In addition, patients stressed wanting to understand their role and “rules of engagement” in the process. They expressed concerns about negatively affecting the patient–physician relationship by involving family members, questioning decisions, discussing second opinions, or asking too many questions. These concerns may limit successful patient engagement in SDM even when there is a desire to participate and highlight the importance of patient education and preparation to empower engagement in the SDM process.14,32 The different priorities between patients and providers are important to address, as these may inadvertently result in the process being less patient centered than intended and affect patient engagement in the process. In addition, it may explain why prior research has shown that there are often varying subjective assessments of SDM between patients and providers rating the same interaction.14,18 This highlights the need for further research on patient-centered outcomes after surgery, such as changes in cognition and sleep; the need for caregivers to better inform these conversations; and the importance of including the patient voice in interventions to improve SDM.
Patients and providers reported minimal preparation for SDM and little knowledge about available resources. Patients did not report any preparation. Providers reported preparation that was mainly focused on assessing baseline function and surgical risk. The provider’s approach to SDM was mostly developed through modeling shaped by clinical experience over time. Surgical providers commonly used risk calculators such as the ACS NSQIP Surgical Risk Calculator to facilitate SDM and enhance transparency about risks and outcomes but had minimal knowledge of specific SDM or communication tools. Prior research has pointed out that although risk calculators and decision aids are useful, they are not enough to generate a complete SDM interaction on their own 33 and that there are significant gaps in surgeons’ effectively using SDM, particularly in patients with a language barrier or low health literacy.14,16,34 Improved dissemination of SDM tools for both patients and providers, the development of surgeon-focused SDM tools, and more explicit training of surgical residents and resident educators may help improve SDM. All participants felt this would be most effective early in training, whether in medical school or residency. In addition, although SDM seems to be used well prior to high-risk surgery, training should encourage the use of SDM in other treatment discussions, particularly those that are preference dependent.
Patients and providers reported several significant barriers that have important implications for the implementation of SDM in surgery. While time limitations are the most commonly reported barrier, particularly in emergent surgery, comprehensive SDM is possible in relatively brief interactions. 13 Embedding SDM tools or access to information that supports SDM such as frailty assessments or what matters to patients in the electronic health record in an accessible way may improve SDM. 13 A novel finding in this study was the use of co-management and using other teams such as palliative care and/or geriatrics in complex situations to empower surgeons to avoid nonbeneficial treatments and focus on nonsurgical options when appropriate. It may also protect against differences in physician and patient priorities and acceptance of risk, which have been shown to result in unwanted treatment. 35 However, managing conflict between team members and family as well as between patients and family members were recognized as potential barriers. Interestingly, both patients and physicians had mixed opinions about involving another person in SDM conversations, which was a novel finding. While potential benefits were recognized, concerns were raised about the effects on the patient–provider relationship and treatment plans when there was conflict. This suggests that inclusion of a support person in SDM may need to be more nuanced, and it may be necessary to discuss the specific role of a support person in SDM conversations, even if that support person is also a surrogate decision maker. In addition, more work is needed to understand how to best utilize a team approach, particularly in the acute setting, as well as the need for ongoing research around frailty and surgical outcomes and provider education to help providers counsel patients appropriately and assess risk.
Our study has several limitations. First, recruitment was confined to a single institution and a relatively small sample, potentially introducing bias and limiting the applicability of the results. However, we incorporated a variety of providers of different levels and different subspecialities to allow for a diversity of opinions. Second, recruitment from a hospital PAC might have led to selection bias, as participants likely had high interest and health literacy in SDM, which may not be representative of the average patient. However, even within this group, there were significant gaps identified in the SDM process. Third, our use of semi-structured focus groups might have introduced researcher bias, which could have missed other important components of this process. Finally, the focus group format might have limited the disclosure of certain opinions.
Conclusions
Our findings show important differences in the perception of SDM between patients and providers and potential ways to include more patient-centered outcomes, challenges in effective communication particularly when outcomes are unclear and there are multiple persons involved, and the lack of education and/or use of existing resources for SDM among surgeons. This study is novel in its use of diverse focus groups with multiple stakeholders including patients and their caregivers to understand and characterize surgical SDM in older adults. Future research should address patient priorities in the creation and refinement of existing SDM frameworks and tools, address patient-centered outcomes to improve counseling in the SDM process, and examine physician training as a method of improving surgeon training and long-term implementation of SDM in clinical practice. Given time barriers, the differing priorities of providers and patients, and age-specific issues related to older adults undergoing surgery, there is a need for targeted tools for surgical SDM, particularly in situations with complex decision making and for use by more junior providers. Embedding these tools and information that supports SDM such as patient goals (“what matters”) and frailty assessments into the electronic health record may improve knowledge and successful utilization of these resources.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683251382259 – Supplemental material for Exploring Key Elements of Surgical Shared Decision Making for Providers and Older Adults
Supplemental material, sj-docx-1-mpp-10.1177_23814683251382259 for Exploring Key Elements of Surgical Shared Decision Making for Providers and Older Adults by Gabriela Poles, Mariah Erlick, Alexis Zimmer and Marcia Russell in MDM Policy & Practice
Supplemental Material
sj-pdf-2-mpp-10.1177_23814683251382259 – Supplemental material for Exploring Key Elements of Surgical Shared Decision Making for Providers and Older Adults
Supplemental material, sj-pdf-2-mpp-10.1177_23814683251382259 for Exploring Key Elements of Surgical Shared Decision Making for Providers and Older Adults by Gabriela Poles, Mariah Erlick, Alexis Zimmer and Marcia Russell in MDM Policy & Practice
Footnotes
Acknowledgements
We would like to thank the members of the University of Rochester Patient Advisory Council. Their insights, lived experiences, and feedback were invaluable to this work.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by the American Society of Colon and Rectal Surgeons Research Foundation. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. This work is based on research supported by a grant from The Research Foundation of the American Society of Colon and Rectal Surgeons. The research, findings, conclusions, and recommendations expressed in this work are those of the authors and not The Research Foundation of the American Society of Colon and Rectal Surgeons.
Ethical Considerations
Not applicable.
Consent to Participate
Verbal informed consent was obtained from the participants.
Patient Consent
There is no identifying information in the article. All participants are identified by participant ID alone in quotes and tables. Verbal consent was obtained for participation in the study.
Consent for Publication
Not applicable.
Data Availability
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.