
Abstract
Highlights
This study investigated whether axicabtagene ciloleucel (axi-cel) is cost-effective in second-line (2L) and third-line (3L) treatment sequences in the current relapsed or refractory (R/R) diffuse large B-cell lymphoma (DLBCL) treatment paradigm.
Using a novel treatment sequencing model, axi-cel was found to be cost-effective in both 2L treatment sequences and in direct comparisons with 3L bispecific T-cell antibodies.
These findings suggest that axi-cel is a cost-effective treatment for R/R DLBCL regardless of treatment line positioning.
Keywords
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma, accounting for approximately one-third of cases. 1 With chemoimmunotherapy, 60% to 70% of patients can achieve long-term remission. 2 However, the prognosis for patients who do not respond to therapy or relapse after an initial response has historically been poor. 3 In recent years, novel immunomodulatory treatments have become available in the management of relapsed or refractory (R/R) DLBCL, representing a marked advancement in treatment options in addition to the second-line (2L) historic standard therapeutic option comprising high-dose chemotherapy (e.g., BEAM combination containing carmustine, etoposide, cytarabine, and melphalan) followed by autologous stem cell transplant (ASCT) for patients who responded to 2L chemotherapy. However, because of its toxicities, ASCT cannot easily be offered to elderly or unfit patients.3,4 ASCT-ineligible patients may be treated with other options such as polatuzumab vedotin in combination with bendamustine and rituximab (Pola-BR), tafasitamab in combination with lenalidomide (tafa-len), or rituximab in combination with gemcitabine and oxaliplatin (R-GemOx). 5
Notably, the availability of chimeric antigen receptor T (CAR T)-cell therapies has been considered a breakthrough in cancer treatment, and CAR T-cell therapies have emerged as a curative treatment option for hematologic cancers. 6 Real-world studies have shown that eligibility criteria may be less stringent than those for ASCT, creating a population of patients eligible for CAR T-cell therapy but ASCT ineligible. 4 In the United States, axicabtagene ciloleucel (axi-cel) has been approved by the Food and Drug Administration (FDA) for the treatment of R/R DLBCL.7–9 Current US treatment guidelines recommend axi-cel for the 2L treatment of DLBCL for patients who relapsed within 12 mo or had primary refractory disease, as well as for third line (3L) and above. 10
Bispecific T-cell antibodies (BsAbs) are the most recent targeted therapies approved for treating R/R DLBCL. Two BsAb products, glofitamab and epcoritamab, received accelerated FDA approvals in 2023 for DLBCL in patients who received at least 2 prior systemic therapies11,12 and are recommended 3L and later treatments for DLBCL in the United States. 10 Unlike CAR T-cells, which need to be manufactured by genetically modifying patient-derived T-cells ex vivo before transferring the modified cells back into the patient, BsAbs are considered an off-the-shelf product. 13 However, BsAbs require multiple dosing, including up to 12 cycles of treatment across over 8 mo in the case of glofitamab and indefinite treatment until disease progression in the case of epcoritamab, while CAR T-cell therapies are administered via a 1-time dose.
Given the dynamic treatment paradigm in many oncology indications, understanding the impact of treatment sequences has become increasingly important to health care decision makers. 14 Most cost-effectiveness studies of treatment strategies in DLBCL published to date have focused on specific treatment lines.15–18 However, with several treatments, including CAR T-cell therapies, now being approved for use in different lines for DLBCL, it has become increasingly relevant not only to estimate which treatments are more cost-effective at a given line or in a specific subpopulation but also to incorporate treatment sequencing across therapy lines in the modeling approach. Furthermore, with the recent introduction of bispecific therapies into the 3L+ DLBCL treatment landscape, there is also a need to determine the most cost-effective strategy in a more conventional line-specific analysis. To understand the impact of treatment sequencing on patient outcomes and costs to the health care system, we developed a patient-level discrete event simulation (DES) model in DLBCL to compare the cost-effectiveness of different treatment sequences in the 2L and above setting and of novel bispecific treatments compared with axi-cel in the 3L setting from the US payer perspective.
Methods
Model Structure
To simulate the clinical and economic outcomes of different treatment sequences, a DES model was used to explore treatment pathways. Although the model was developed to consider a more comprehensive DLBCL pathway from 1L to 3L, the current evaluation had 2 focuses: a 2L to 3L sequence analysis and an exclusively 3L analysis. Thus, the patient population of this analysis and the results presented herein relate solely to patients who had progressed after 1L or 2L and were eligible to receive a 2L or 3L treatment, respectively. Model outputs included discounted health outcomes (life-years [LYs] and quality-adjusted life years [QALYs]) and economic outcomes (total costs, incremental cost-effectiveness ratios [ICERs] and net monetary benefit [NMB]).
A detailed description of the methodology of the treatment-sequencing model is provided in the Supplemental Methods, Supplemental Table 1 and Supplemental Figures 1 to 4. The model was conducted from the perspective of a US health care payer, and the base-case analyses used a lifetime horizon of 50 y with costs and outcomes discounted at 3.0%, per guidelines. 19 Analyses were considered cost-effective at a threshold of $150,000 per QALY, as per the upper limit in ICER guidelines, 19 but they were also calculated for a range of thresholds from $100,000 to $200,000 per QALY. For the current analyses, 100,000 patients were simulated starting at diagnosis, and the model reported results for the line of interest onward, with discounting starting at that same line; for example, for a 2L to 3L sequence, results were reported for 2L patients onward and discounting started at the initiation of 2L therapy.
The cost-effectiveness of 2L axi-cel followed by 3L treatments (specified proportions of patients receiving salvage chemotherapy or BsAbs; Table 1 and Figure 1) were compared with treatment sequences of 2L intended ASCT (i.e., high-dose chemotherapy followed by ASCT for those 30%–35% who respond; Table 1), 2L polatuzumab vedotin with bendamustine and rituximab (Pola-BR), 2L tafastimab with lenalidomide (tafa-len), or rituximab with gemcitabine and oxaliplatin (R-GemOx), all followed by 3L treatments (salvage chemotherapy, BsAbs, or axi-cel). In addition, to investigate the cost-effectiveness of 3L axi-cel compared with the newly approved 3L BsAbs, the following 3L-focused comparisons were made: axi-cel versus glofitamab and axi-cel versus epcoritamab. As the analysis involves multiple comparators, comparators were first arranged in ascending order of cost, then ICERs and NMBs were calculated after ruling out either strongly or extendedly dominated comparators.
Model Parameters
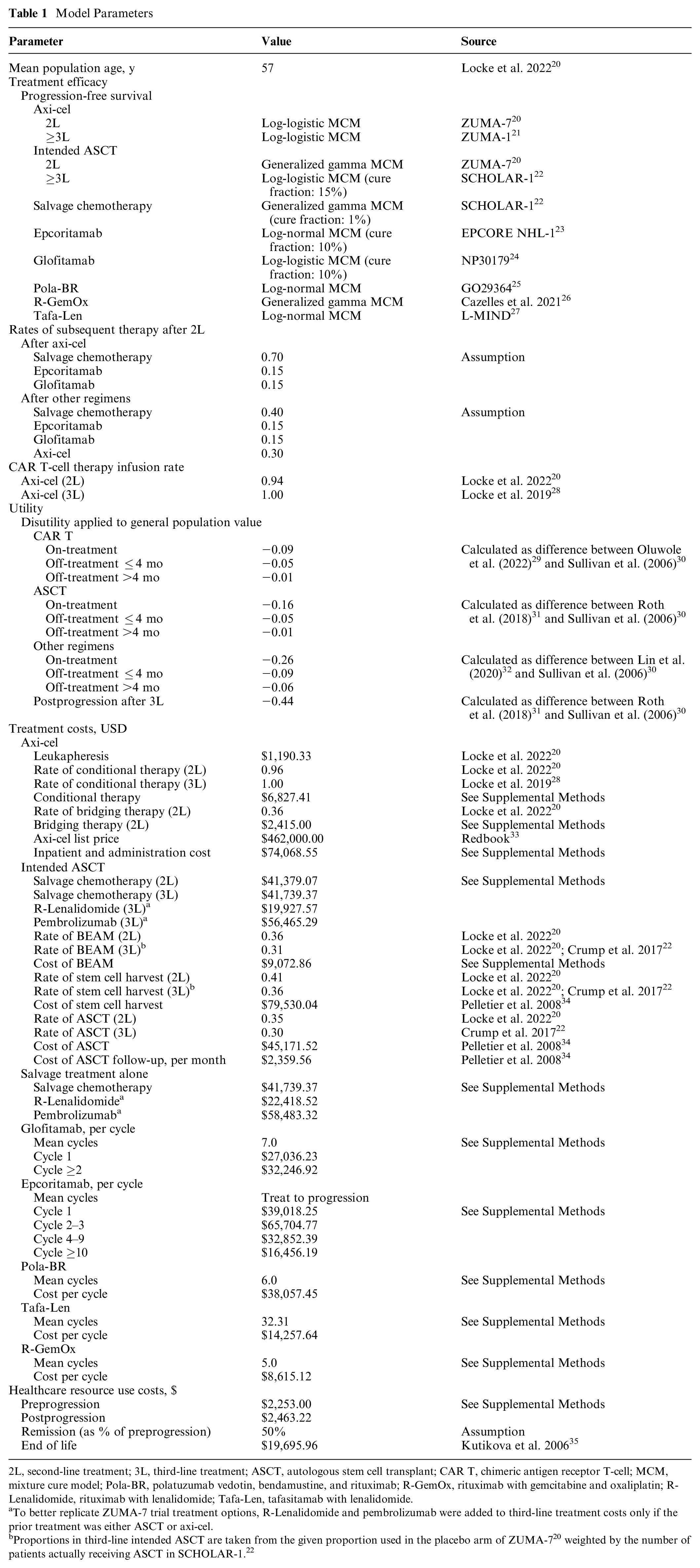
2L, second-line treatment; 3L, third-line treatment; ASCT, autologous stem cell transplant; CAR T, chimeric antigen receptor T-cell; MCM, mixture cure model; Pola-BR, polatuzumab vedotin, bendamustine, and rituximab; R-GemOx, rituximab with gemcitabine and oxaliplatin; R-Lenalidomide, rituximab with lenalidomide; Tafa-Len, tafasitamab with lenalidomide.
To better replicate ZUMA-7 trial treatment options, R-Lenalidomide and pembrolizumab were added to third-line treatment costs only if the prior treatment was either ASCT or axi-cel.

Overview of treatment pathways.
Model Parameters
An overview of clinical, economic, and quality-of-life parameters used in the model is provided in Table 1. In terms of efficacy, in the absence of direct evidence on comparative effectiveness between axi-cel and each comparator, naïve comparisons were used in the cost-effectiveness analysis as statistically adjusting the small, heterogenous study populations may introduce bias and compromise the robustness and reliability of the analysis given the differences in available follow-up. Progression-free survival (PFS) and overall survival (OS) data were sourced from the pivotal trials. Pseudo-individual patient data were generated using a common algorithm developed by Guyot et al.36,37 and extrapolated using parametric mixture cure models (MCMs), using the flexsurvcure package in R. 38 Since the BsAbs trials have a short follow-up, the durability of the response to these treatments is still uncertain. The modeled cure fraction was therefore set to 10%, which was chosen such that the predicted OS data best fit the OS data from the respective BsAbs trials.23,24 An MCM approach was used for modeling the efficacy of axi-cel as it is the most accurate method for CAR T-cell therapies. 39 In an effort to not unduly favor axi-cel, MCM, rather than standard parametric survival methods, was also used for the other treatments. Further details of survival modeling are available in the Supplemental Methods.
Costs are reported in 2023 US dollars (USD). Healthcare Resource Use (HCRU) costs were sourced from the published literature and include costs for general practitioner visits, inpatient and outpatient hospital days, computed tomography (CT) scans, full blood counts, and liver and renal function tests. HCRU rates associated with the preprogression and postprogression health states were assigned without regard for line of treatment based on a previous cost-effectiveness model based on the ZUMA-7 trial (Supplemental Table 3).
Treatment costs were sourced from the available literature and Micromedex 33 where applicable (Supplemental Tables 4 and 5); inputs were inflated using the consumer price index medical care inflation index. 40 All drug costs were based on no vial sharing. For the CAR T-cell therapies, in addition to the acquisition costs, patients also required leukapheresis, and they may also have bridging and/or conditioning chemotherapy.
The model includes grade 3 or higher adverse events (AEs) (Supplemental Table 6). AE costs were included in the model as one-off costs and were sourced from published cost-effectiveness models (Supplemental Table 7). Following prior cost-effectiveness studies in DLBCL, it was assumed that patients who received axi-cel were hospitalized for a total of 17.6 d on average, including 3.7 d in the intensive care unit. 31 In line with previous cost-effectiveness studies in DLBCL, hospitalizations were assumed to include the management of all occurring grade ≥3 AEs.15,31 For glofitamab and epcoritamab, AE management costs were sourced from Mahmoudjafari et al. 41
Health state utilities were used to estimate QALYs and were sourced from the literature (Supplemental Table 8). 30 Baseline general population utility was adjusted by applying utility decrements to preprogression (on and off treatment) and postprogression health states by calculating the difference between baseline and health state utilities (Table 1). Disutilities for AEs were not considered separately but assumed to be included in the “on-treatment” disutility.
Scenario and Sensitivity Analyses
Additional scenario analyses were explored to address key uncertainties. The model leveraged data from separate clinical trials and used them in a naïve manner (i.e., population differences are not adjusted for). The included trials are summarized in Supplemental Table 2. Differences between trials are minimal; however, there is some variability in patient age as well as in some patient fitness measures (i.e., Eastern Cooperative Oncology Group score, disease stage, International Prognostic Index [IPI] score). Trials using older patients have some measures of lower patient fitness and vice versa. For example, the trials for pola-BR, R-GemOx, and tafa-len have a greater median age as well as a greater proportion of patients with high-risk IPI scores. The age of the population in the analysis was anchored to the median age in ZUMA-7, age 57 y. To test the impact of this choice, a scenario analysis was run with the population age at 72 y, the oldest among the comparator trials; intended ASCT was not run in this setting as this age would likely preclude most patients from having a transplant. Given the unknown composition of subsequent treatment, we tested the impact of increasing the axi-cel proportion in 3L from 30% to 50% (50% axi-cel, 15% glofitamab, 15% epcoritamab, 20% salvage) and the impact of increasing the proportion of BsAbs in 3L from 15% each to 30% each (30% axi-cel, 30% glofitamab, 30% epcoritamab, 10% salvage).
For the 3L-focused scenarios, 2 analyses were conducted: the first restricted the treatment duration of epcoritamab to 2 y (versus treat until progression in the base case), and the second explored the impact of reducing the cure fraction for BsAbs from 10% to 0%.
Input uncertainty was evaluated through probabilistic sensitivity analyses, in which all parameters were varied across predetermined distributions. Results of the probabilistic sensitivity analyses are presented as cost-effectiveness planes and cost-effectiveness acceptability curves. Detailed methods are available in the Supplemental Methods, and the detailed results are available in Supplemental Figures 5 to 8.
Results
2L to 3L Treatment Sequencing for 1L R/R Patients
In considering the 2L treatment in patients who were simulated over 2-3L (Table 2), after arranging 2L comparators according to discounted cost, treatments ranged from $379,412 for R-GemOx to $706,460 for tafa-len. Discounted QALYs ranged from 3.38 for R-GemOx to 7.23 for axi-cel. ASCT was strongly dominant over pola-BR in 2L, meaning it was less costly and more effective, and axi-cel was strongly dominant over tafa-len. Both total lifetime discounted costs and QALYs were higher for 2L ASCT compared with R-GemOx, and the resulting ICER for 2L ASCT was cost-effective at $9,495 per QALY. Compared with 2L ASCT, both total discounted costs and QALYs were higher for 2L axi-cel. The resulting ICER for 2L axi-cel versus 2L ASCT was $145,004 per QALY, which is below the $150,000 per QALY willingness-to-pay (WTP) threshold. Axi-cel was the overall most cost-effective strategy in 2L, yielding an optimal NMB at WTP thresholds of $150,000 per QALY as well as $200,000 per QALY (Table 2). Intended ASCT was, however, more cost-effective at the lower threshold of $100,000. This is supported by a cost-effectiveness efficiency frontier plot, which has R-GemOx, ASCT, and axi-cel as cost-effective options depending on the WTP threshold (Figure 2).
Cost-Effectiveness Results (Discounted) for ≥2L Sequences, 2023 $US

2L, second line; 3L, third line; ASCT, autologous stem cell transplant; axi-cel, axicabtagene ciloleucel; ICER, incremental cost-effectiveness ratio; LY, life-year; NMB, net monetary benefit; Pola-BR, polatuzumab vedotin, bendamustine, and rituximab; QALY, quality-adjusted life-year; R-GemOx, rituximab in combination with gemcitabine and oxaliplatin; Tafa-Len, tafasitamab lenalidomide; USD, United States dollar; WTP, willingness-to-pay.
Optimal strategy maximizing NMB at the corresponding WTP threshold (λ).

Cost-effectiveness efficiency frontier plot for second-line comparators.
Key model parameters were tested for their impact on the results in a set of scenarios (Supplemental Table 10). In terms of the population age, the implication of the results was unchanged, although they did yield lower QALYs and marginally lower costs for each treatment, as shown in the cost-effectiveness efficiency frontier (Figure 2). Pola-BR and tafa-len were extendedly dominated by axi-cel, rather than strongly dominated compared with the results using a mean age of 57 y, and only axi-cel yielded an ICER below the WTP threshold of $150,000 per QALY compared with R-GemOx, the least expensive treatment and the only other treatment not extendedly dominated. Changing the treatment composition of the 3L treatments had some impact on the cost-effectiveness of the 2L options. This was impactful for intended ASCT, which became the least expensive treatment option, and this shifted the ICERs for axi-cel to just above $150,000, while the other treatments remained dominated by either ASCT or axi-cel.
The 2-3L probabilistic sensitivity analysis found that axi-cel had the greatest probability of being cost-effective at a WTP threshold of $150,000 per QALY with a probability of 49%, followed by 33% for ASCT and 15% for tafa-len (Supplemental Figure 6). Axi-cel was also the most cost-effective at the $200,000 per QALY upper bound with a probability of 58% followed by tafa-len at 22% and ASCT at 18%. At the $100,000 per QALY lower bound, ASCT had the greatest cost-effectiveness probability at 59%, with axi-cel having a probability of 29%.
3L Treatment Focused on Axi-Cel versus BsAbs
In considering the 3L setting, treatment costs ranged from $283,147 for glofitamab to $654,116 for epcoritamab (Table 2). Similar to the 2L setting, axi-cel use resulted in greater QALYs when compared with BsAbs in 3L. The discounted QALYs were higher for axi-cel compared with glofitamab (4.59 versus 2.01; Table 2). Treatment costs for glofitamab were lower than for axi-cel ($598,484), and the resulting ICER was $122,224 per QALY, indicating that axi-cel would be considered cost-effective in the US payer setting. When comparing axi-cel to epcoritamab in 3L, total discounted QALYs were higher for axi-cel compared with epcoritamab (4.59 versus 1.81; Table 2). Total discounted costs were $654,116 with epcoritamab, higher than axi-cel; hence, axi-cel is a dominant treatment option in the 3L setting compared with epcoritamab. The 3L cost-effectiveness comparisons are shown in a cost-effectiveness efficiency frontier plot, which supports glofitamab and axi-cel as cost-effective options with the latter being optimal at the base WTP threshold of $150,000 per QALY (Figure 3).

Cost-effectiveness efficiency frontier plot for third-line comparators.
Axi-cel remained cost-effective in scenario analyses. In the base-case analysis, glofitamab was assumed to have a 10% cure fraction. In a scenario analysis with no patients (0%) treated with glofitamab achieving cure, the resulting ICER for axi-cel versus glofitamab was $88,272 per QALY (Supplemental Table 10). In the base-case analysis, epcoritamab was administered until progression. In a scenario analysis in which the maximum treatment duration for epcoritamab was restricted to 2 y, the resulting ICER for axi-cel versus epcoritamab was $82,395 per QALY, which is below the cost-effectiveness threshold of $150,000 per QALY (Supplemental Table 10). In a scenario analysis in which the 10% cure fraction of epcoritamab was lowered to 0%, epcoritamab was less effective (1.06 QALYs) but was also considerably less expensive ($472,622) than axi-cel. Nevertheless, axi-cel remained cost-effective with an ICER of $32,655.
The 3L-focused probabilistic sensitivity analysis found that axi-cel had the greatest probability of being cost-effective at a WTP threshold of $150,000 per QALY with a probability of 73%, followed by 26% for glofitamab and <1% for epcoritamab (Supplemental Figure 8). Axi-cel also had the highest probability of cost-effectiveness at thresholds of $200,000 per QALY (84%) and $100,000 per QALY (57%).
Discussion
This analysis explored the cost-effectiveness of axi-cel in the 2L and beyond treatment of DLBCL using various scenarios. In the sequences starting from 2L, all modeled treatment sequences with BsAbs available in 3L demonstrate the cost-effectiveness of axi-cel compared with other 2L comparators (intended ASCT, Pola-BR, tafa-len, and R-GemOx) at a WTP threshold of $150,000 per QALY, evidenced by axi-cel’s maximal NMB versus the other comparators. Axi-cel remains the most cost-effective 2L treatment option, yielding the greatest NMB, at a $200,000 per QALY threshold; however, intended ASCT (i.e., high-dose chemotherapy followed by ASCT for those 30%–35% who respond; Table 1) is more cost-effective at a lower $100,000 per QALY threshold. This indicates that the optimal treatment strategy in R/R DLBCL is sensitive to the WTP threshold, favoring 2L intended ASCT at ≤$100,000 per QALY and favoring 2L axi-cel at ≥$150,000 per QALY. Importantly, OS is significantly greater for patients receiving axi-cel compared with those with intent to ASCT; thus, while the latter may be a cost-effective option at this lower threshold, it may not be the best clinical option for patients. 42 For these 2L sequences, to our knowledge, this is the first study to evaluate the current treatment permutations. Indeed, one of the primary advantages of the DES sequencing approach is that it allows for rapid comparison of different treatment permutations, required to account for the evolving shifts in the treatment paradigm. Nonetheless, our 2L ASCT-eligible results can be placed in the context of prior cost-effectiveness analysis of the ZUMA-7 trial. A recent update to the original partitioned survival model (PSM) predicted incremental QALYs of 1.63 in favor of axi-cel (versus standard of care) and incremental costs of $159,909 for in ICER of $98,040, compared with incremental QALYs of 2.12 and incremental costs of $305,958 predicted by the DES in this study. 16 That both incremental costs and incremental QALYs are higher in the current analysis is explained by the difference in the proportion of patients using CAR T post-ASCT, which was higher in the ZUMA-7 trial than modeled here due to the availability of BsAbs as a 3L option. Although ZUMA-7 PSM results provide context, the models are not identical. The PSM directly models the ZUMA-7 randomized controlled trial, while the current models bridge the gap between available head-to-head data and emerging treatment paradigms. The current work does compare well with the results of PSMs estimating the cost-effectiveness of Pola-BR (discounted QALYs of 3.46 in the current study [Supplemental Table 10] v. 3.31) and R-GemOx (discounted QALYs of 2.93 in the current study [Supplemental Table 10] v. 3.10).
In the 3L setting, axi-cel was less costly and more effective versus epcoritamab, attributed in part to patients undergoing continued treatment with epcoritamab while in preprogression as per the product’s prescribing information. However, the effect of this assumption did not change the conclusion of the analysis as axi-cel remained cost-effective in the scenario in which epcoritamab treatment was limited to a maximum of 2 y. In addition, in the 3L setting, while patients treated with axi-cel incurred higher treatment costs, survival time was longer compared with glofitamab, and consequently, the ICER is cost-effective at the commonly accepted $150,000 per QALY WTP threshold in the United States. These conclusions were consistent when reducing the proportion of patients receiving glofitamab who would remain in long-term remission to zero (versus cure fraction of 10% in the base case), which resulted in a lower ICER favoring axi-cel. Whereas 3L axi-cel yielded optimal NMBs at $150,000 and $200,000 per QALY thresholds, glofitamab was favored at $100,000 per QALY. Although axi-cel was still favored in probabilistic results at $100,000 per QALY (Supplementary Figure 8), the 3L analysis may be sensitive to the WTP threshold and 3L glofitamab may be a cost-effective strategy at this lower threshold.
Previous economic analyses have compared BsAbs to axi-cel in the 3L setting. Using a PSM and an unanchored matching-adjusted indirect comparison (MAIC) to inform the relative effectiveness of epcoritamab versus axi-cel, Qu et al. 43 found that epcoritamab was dominant over axi-cel (less costly and more effective). However, there are important differences between the current analysis and those from Qu et al. The use of the unanchored MAIC is questionable because the improved efficacy claimed for epcoritamab compared with axi-cel was not statistically significant. Furthermore, axi-cel efficacy, rather than epcoritamab efficacy, was improved compared with the naïve comparison in another epcoritamab versus axi-cel MAIC study. 44 In addition, treatment costs for epcoritamab were incurred only in the first 2 y of being progression free. In contrast, our analysis adopted a more pragmatic approach and provided an assessment of the cost-effectiveness of epcoritamab and axi-cel within the boundaries of the available evidence, given the demonstrated long-term survival of axi-cel patients 45 versus the current short-term follow-up available for epcoritamab. Another study, also based on an MAIC, compared the cost-utility of glofitamab in adult patients with R/R DLBCL versus a set of different comparators, including axi-cel, in the Italian setting. 46 Authors reported comparable incremental QALYs (2.80 versus 2.65) in favor of axi-cel and found glofitamab to be cost-effective in the southwest cost-effectiveness quadrant at a WTP threshold of EUR €40,000 per QALY, a threshold far lower than is commonly used in the United States. In line with this, a QALY advantage was reported for axi-cel compared with glofitamab in the National Institute for Health and Care Excellence health technology assessment submission for 3L+ glofitamab. 47
Previous economic analyses have highlighted the importance of long-term evidence on increasing certainty in estimates of clinical efficacy. 16 The length of follow-up for survival outcomes for axi-cel (median: 47.2 mo) 42 is notably longer than that for glofitamab and epcoritamab (median: 12.0 mo)23,24; hence, survival data for the BsAbs may be considered immature given the shorter follow-up time. The available data strongly suggest a curative effect of axi-cel. Indeed, between the 4-y and 5-y follow-up analyses of ZUMA-1, 92% of patients remained alive without the need for subsequent therapy. 48 MCM has been shown to be a valid approach for modeling survival for axi-cel; however, modeling the curative potential of BsAbs has not yet been demonstrated. To that end, even under an assumption of a low but plausible cure fraction of 10%, axi-cel remained cost-effective versus both BsAbs.
Results of the current analysis should be interpreted considering certain limitations. Except for the PFS outcomes for axi-cel and intended ASCT in 2L, which were assessed head to head in ZUMA-7, the survival data used in the model were compared naïvely. Although this does not affect the comparison of axi-cel to ASCT, both from ZUMA-7, it may underestimate the efficacy of other comparators (i.e., pola-BR, R-GemOx, tafa-len) as they are informed by trials with older and less fit patients. Importantly, subgroup analyses of the ZUMA-7 trial revealed that patient survival is not substantially affected by age or level of sickness after axi-cel or ASCT. 42 This was also explored in a scenario analysis, however, in which the patient age in the simulations was instead anchored to the trial with the oldest patients (L-MIND, age 72 y), and cost-effectiveness conclusions did not change substantively. In addition, the trial populations informing axi-cel efficacy were largely ASCT naïve, which may not be the case for some comparator sources, and the BsAbs trial population included some individuals who had previously used CAR T-cell therapy. Comparators were also sourced naively in the 3L comparison; however, the efficacy of axi-cel was either slightly improved or essentially unchanged in the MAIC analyses comparing 3L axi-cel to each of the bispecifics.44,49 In considering the best available evidence, there is therefore no suggestion of naïve comparisons in 3L meaningfully biasing the results in either direction. The rationale for using naïve comparisons, as opposed to an indirect treatment comparison adjusting for the population differences, was driven by the differences between the clinical trials, particularly the low number of study participants and different follow-up time horizons. In such cases, performing an indirect treatment comparison would not have resolved any uncertainties compared with using naïve comparisons. In 3L, imposing a cure fraction of 10% for the BsAbs was based on current clinical data, which have not demonstrated long-term durable remissions. The costs of epcoritamab have been estimated based on the prescribing information stating that patients remain on treatment until progression; however, the clinical reality may be different. Nonetheless, it should be noted that the conclusions of the current cost-effectiveness analysis were held even when the treatment time horizon was restricted.
Conclusion
Our analysis shows that although results are sensitive to the WTP threshold, axi-cel in the 2L treatment sequences is a cost-effective option compared with all other potential comparators at a threshold of $150,000 per QALY in the United States. In the 3L comparisons to the newly approved bispecifics, glofitamab and epcoritamab, axi-cel was also found to be the most cost-effective strategy at the $150,000 per QALY threshold in the United States.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683251345780 – Supplemental material for A Cost-Effectiveness Analysis of Diffuse Large B-Cell Lymphoma Treatment Pathways in the United States
Supplemental material, sj-docx-1-mpp-10.1177_23814683251345780 for A Cost-Effectiveness Analysis of Diffuse Large B-Cell Lymphoma Treatment Pathways in the United States by Anik R. Patel, Bradley Kievit, Ken Hasegawa, Markqayne Ray, Rishika Sharma, Sarahmaria Hofmann, Rob Blissett and Frederick L. Locke in MDM Policy & Practice
Footnotes
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kievit, Sharma, Hofmann (former), and Blissett are employees of Maple Health Group, who were contracted by Kite Pharma to conduct the work contained in this article. Patel (former), Hasegawa, and Ray are employees of Kite Pharma. Locke received consulting fees from Kite, A Gilead Company; A2; Allogene; Amgen; Bluebird Bio; Bristol-Myers Squibb; Calibr; Caribou; Cowen; EcoR1; Gerson Lehrman Group; Iovance; Janssen; Legend Biotech; Novartis; Sana; Umoja; and Pfizer. Locke received institutional support from the Society for Immunotherapy of Cancer, Leukemia and Lymphoma Society, and National Cancer Institute. Locke has patents under his name. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a contract with Kite, A Gilead Company. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following authors are employed by the sponsor: Patel, Hasegawa, and Ray.
Author Contributions
Concept and design: Patel, Kievit, Hasegawa, Ray, Sharma, Hofmann, Blissett, Locke; data analysis: Kievit, Sharma, Hofmann, Blissett; data interpretation: Patel, Kievit, Hasegawa, Sharma, Hofmann, Blissett, Locke; drafting of the manuscript: Kievit, Hofmann, Blissett; critical review of the manuscript: Patel, Kievit, Hasegawa, Ray, Hofmann, Blissett, Locke; administrative, technical, or material support: Patel, Kievit, Hasegawa, Ray, Sharma, Hofmann, Blissett, Locke. It is affirmed that everyone who has contributed significantly in the work are listed in this section.
Ethical Considerations
The present study does not involve human or animal subjects and was therefore not subject to an Ethics Committee or Institutional Review Board approval.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
Detailed descriptions of the analytic methods are available in the “Methods” section and the supplemental material. The data used for this study contain confidential and proprietary information and therefore cannot be shared for compliance purposes.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.