
Abstract
Highlights
Diminishing marginal lifespan utility (DMLU) means that the value of extending lifespan may differ based on the duration of life already lived.
DMLU is not typically considered in cost-effectiveness analyses.
Not considering DMLU may bias cost-effectiveness analyses against equity.
Not considering DMLU may reduce the accuracy of distributive cost-effectiveness analyses and other approaches to consider equity along with efficiency.
Cost-effectiveness analyses (CEAs) attach the same value to adding life-years to long versus short lifespans, assuming there are no age-related decrements in quality of life and that the additions occur presently rather than in the future. This brief report asks whether a third concept, diminishing marginal lifespan utility (DMLU), may also be relevant for valuing extensions of longer compared with shorter lifespans in CEA. DMLU is intertwined with the commonly cited notion of “utility curvature,”1–5 the concavity in a utility curve that is indicative of diminishing marginal returns to scale. In the case of health, the diminishing marginal returns are to a QALY gain variably constituted from changes in lifespan and quality of life together with the probabilities and temporal proximities of these changes. However, unlike the general notion of utility curvature, the more specific notion of DMLU reflects diminishing returns to increasing lifespan only, as distinct from quality of life, probability, and temporal proximity, implying that a particular increment in lifespan (e.g., 1 additional year of life) confers lesser marginal utility if added to a longer lifespan (e.g., 90 y to 91 y) than to a shorter lifespan (e.g., 60 y to 61 y). DMLU has evident implications for valuing health equity in CEA because it implies that a life-prolonging intervention would confer greater value if allocated to a community with a 60-y life expectancy (LE) than if allocated to a community with a 90-year LE.
Does DMLU exist?
The existence of DMLU can be inferred from the observation that people prefer to not live indefinitely long, regardless of their age, even in a hypothetical scenario in which slowing the aging process preserves health-related quality of life.6–8 When people in resource-rich countries are surveyed about their preferred length of life, median and/or mean ages are consistent (Germany, 85 y; Norway, 91 y; United States, 90–93 y). Most people do not want to live past 100 y old (United States, 74%–91%; Finland, 67%), even if they can preserve high quality of life (United States, 56%–80%). Surprisingly, notions of ideal lifespan change little as people age. In a nationally representative telephone survey in the United States of more than 2,000 adults conducted in English and Spanish, 8 the proportion of people desiring life expectancies between 79 and 100 y of age did not change by age group (18–29 y old, 64%; 30–49 y, 70%; 50–64 y, 71%; ≥65 y, 70%) nor did the median preferred lifespan, ranging from 85 y to 90 y. In a regionally representative mail-based survey of community-dwelling elders in Finland, the median preferred lifespans were 91 y among people ≥70 y old and 96 y among people ≥85 y old. 6
What Are Plausible Values for DMLU?
DMLU is difficult to measure directly because it is challenging to parse from other constituents of utility curvature.1–5 First, because lifespan is inextricably bound to the passage of time, measurements relevant to DMLU often encompass time preference. Second, because survival is never certain, measurements of DMLU may reflect risk attitudes unless tradeoffs are designed to be risk free, involving a known and fixed number of years to be lived (i.e., lifespan) rather than a probabilistic and average number of years to be lived (i.e., LE), or with adjustments for risk attitudes that may reflect optimism, pessimism, or other reasons for preferring a fixed lifespan to an equivalent probabilistic LE. 2 In addition, DMLU has been less often evaluated than other utility theory–based hypotheses such as correction of health utility elicitation methods to adjust for discounting and/or risk attitudes, such as probability weighting in prospect theory.2,9
Despite these challenges, insights about DMLU are available from studies of tradeoffs from an individual’s perspective using various stated preference approaches including time tradeoffs, standard gambles, discrete choice experiments, and willingness to pay.1,2,4,5,9–20 Table 1 shows a review of studies that parsed DMLU from other determinants of utility curvature by focusing on lifespan instead of LE (i.e., removing risk) and omitting age-related changes in quality of life. Notably, studies in Table 1 did not parse DMLU from discounting, and therefore, results reflect a combination of DMLU and discounting. However, many results have different parameterizations (e.g., power function) or have exponential declines exceeding the 3% discount rate typically used in CEAs, implying that either 1) DMLU exists apart from the effect of discounting or 2) discount rates should be substantially higher than those typically used in CEAs (Table 2).
Literature Review of Individual Preference Studies Quantifying Valuation of Future Lifespan with Risk-Free or Risk-Adjusted Framing a
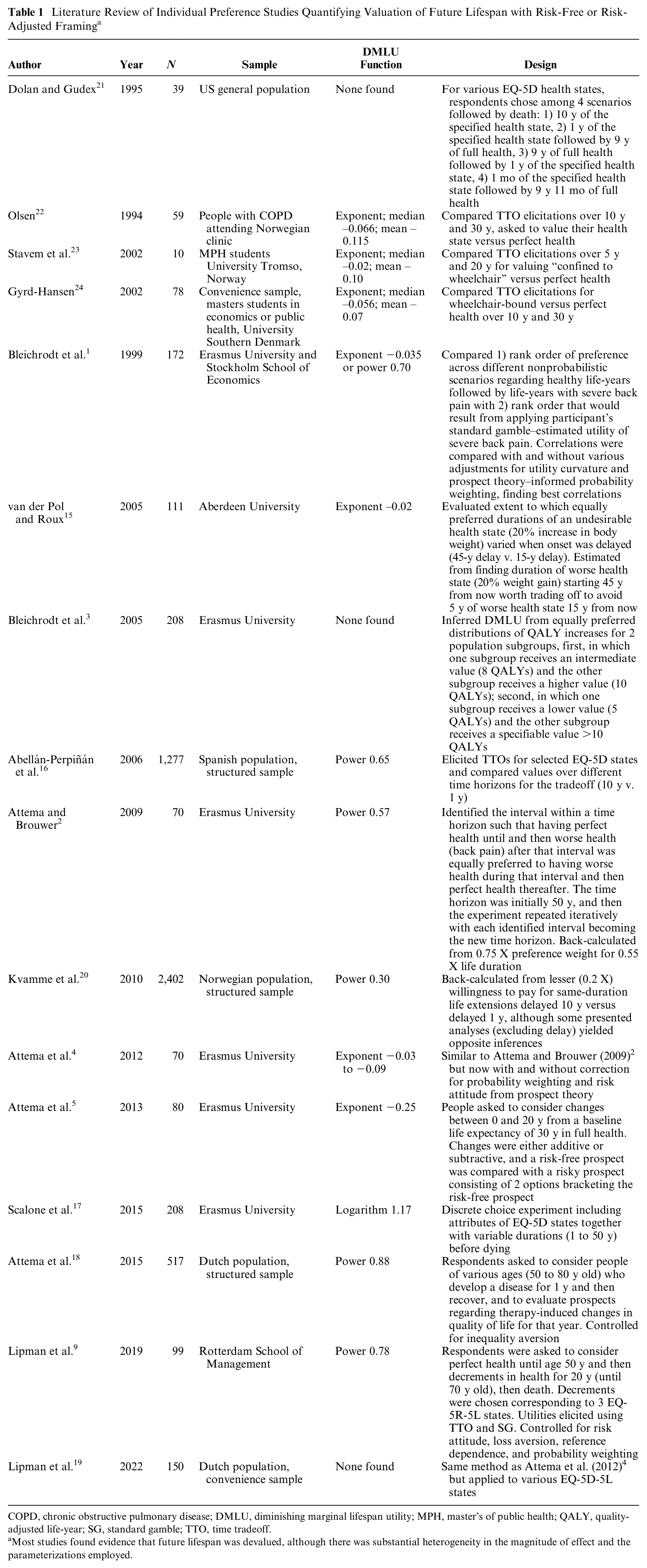
COPD, chronic obstructive pulmonary disease; DMLU, diminishing marginal lifespan utility; MPH, master’s of public health; QALY, quality-adjusted life-year; SG, standard gamble; TTO, time tradeoff.
Most studies found evidence that future lifespan was devalued, although there was substantial heterogeneity in the magnitude of effect and the parameterizations employed.

DMULD, diminishing marginal utility of lifespan duration.
Without discounting or adjusting for diminishing marginal lifespan utility (DMLU), results are similar. With discounting but without adjusting for DMLU, benefits are noticeably larger for non-Black Hispanics than for White persons, yet the differences are still comparatively modest. However, adjusting for DMLU yields benefits that are substantially larger for non-Black Hispanics than for Whites, more reflective of the underlying health inequalities. Because discounted life-years and DMLU-adjusted life-years are sometimes far smaller than unadjusted years, comparisons between unadjusted years, discounted years, and DMULD-adjusted years are facilitated by converting them into their corresponding net monetary benefits through multiplication by their respective willingness-to-pay values ($159,000 per life-year, $303,000 per discounted life-year, and $1,110,000 per DMULD-adjusted life-year, adjusted to 2023 US$).
Adjusted to 2023 $ US.
Because the studies in Table 1 are too heterogeneous for quantitative pooling and results may reflect discounting together with DMLU, they do not yield a definitive inference for the best parameterization of DMLU. However, they inform a plausible range of DMLU parameterization choices with selected examples graphed in Figure 1, alternatively as a power function (with exponentiations ranging from 0.30 to 0.88, with 0.65 as a mid-range estimate), a declining exponential function (with exponents ranging from −0.02 to −0.25, with −0.05 as a mid-range estimate), or a logarithmic function (with 1.172 from a single estimate). For purposes of illustration, I arbitrarily parameterize DMLU with a power function of 0.65 for the remainder of this article; however, other choices based on Table 1 may be equally suitable.
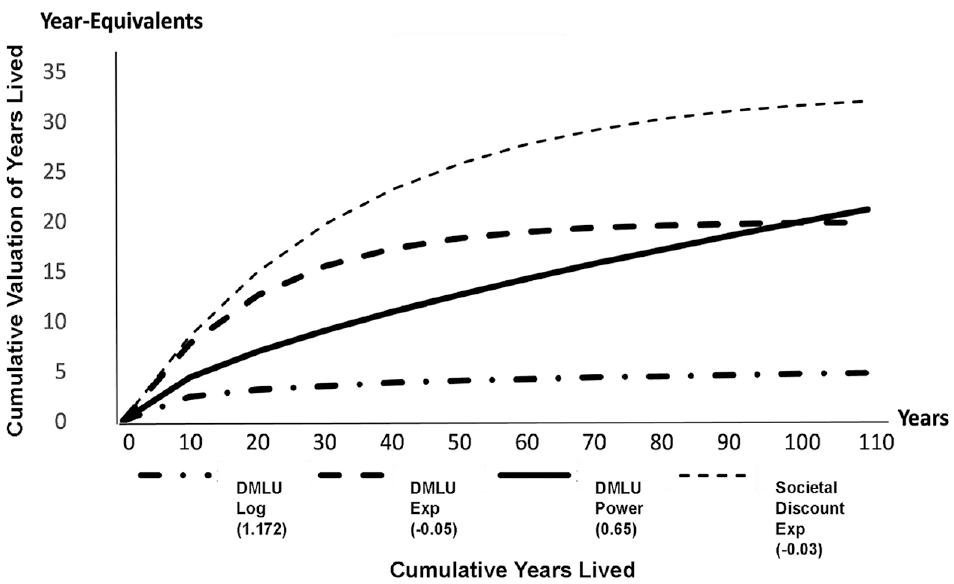
Relationship of alternative DMLU parameterizations to the societal discount rate of 3%.
Implications of DMLU for Valuing Equity
While awareness of the possibility of DMLU is not new, it can be argued that DMLU is becoming increasingly important given the imperative to value equity in CEA, for several reasons that I will explicate in the subsections that follow. First, when it is appropriate to perform CEA over time horizons sufficiently long to bridge different generations in a society, it has been argued that lower discount rates may be required. These lower rates are less likely to incidentally absorb the effects of DMLU. 25 Second, DMLU is incompatible with the use of absolute measures of inequality aversion. Third, CEAs increasingly include measures of societal inequality aversion, and DMLU may bias their interpretation by inflating the apparent level of prioritarianism. 26 Finally, DMLU creates an implicit antiequity bias in life-year–based metrics, potentially reinvigorating the question of whether to consider alternative forms for CEA metrics. While DMLU is just one component of the many forms of inequalities that ought to be considered when conducting economic evaluations, it has important implications that are not otherwise considered. These points are considered sequentially using an illustrative example (Box).
Illustrative example: Allocating resources to improve inequities in cystic fibrosis outcomes

Their respective WTPs can be estimated by a benchmarked comparison that is common to all three, such as “modern medical care” versus “no modern medical care,” a counterfactual that is sometimes used to infer a lower bound for WTP in the United States.36,* In that comparison, the incremental lifetime cost of modern medical care ($509,000 undiscounted and $135,000 discounted) was divided by its incremental life expectancy gains (4.6 y, undiscounted; 0.65 y, discounted) to yield WTP lower bounds ($159,000 per life-year and $303,000 per discounted life-year, equivalent to $1,110,000 per DMULD-adjusted life-year).
Discounting Is Unlikely to Incidentally Absorb the Effects of DMLU
It can be argued that DMLU has more academic than practical importance because the use of societal discounting already overlaps with DMLU. However, incorporating societal discount rates does not avert the need to consider DMLU. Through time horizons typical of CEAs, a societal discount rate of 3% overvalues (Figure 1) future lifespan compared with a 0.65 power function parameterization of DMLU. In addition, DMLU and discounting are conceptually distinct even though both are constructs describing the interaction of time and preferences. DMLU reflects a time-related preference that does not require envisioning various times in the future but rather requires considering only past and current circumstances (e.g., the utility of living an additional time increment, considering time already lived). On the other hand, discounting reflects a time-related preference that can be ascertained not through considering past or current circumstances but rather through envisioning various times in the future (e.g., utility of living an additional time increment at future times). Further, discounting also includes considerations beyond time preference, in particular expectations regarding future wealth, future health, and their marginal rate of substitution.27,28 Accordingly, DMLU can theoretically be parsed from discounting empirically. For example, it may be possible to envision scenarios in which people of various ages (e.g., a 90-y-old with mild disease or a 40-y-old with severe disease) but with the same LE (e.g., 5 y) and the same quality-of-life impairment (e.g., wheelchair bound) consider what portion of a 5-y lifespan they would tradeoff to live in perfect health.2,4,19
Extending the line of reasoning parsing DMLU from discounting, if life-years gained through a CF improvement program are not discounted and not adjusted for DMLU, their corresponding net monetary benefits would be similar for both resource investments in clinics serving largely White persons and those serving largely non-Black Hispanic persons, failing to reflect the corresponding health inequalities (Figure 2). If life-years gained are discounted and not adjusted for DMLU, benefits are noticeably larger for non-Black Hispanics than for White persons, yet the differences are still comparatively modest. However, if life-years gained are adjusted for DMLU, benefits are substantially larger for non-Black Hispanics than for Whites, more reflective of the underlying health inequalities (Figure 2).
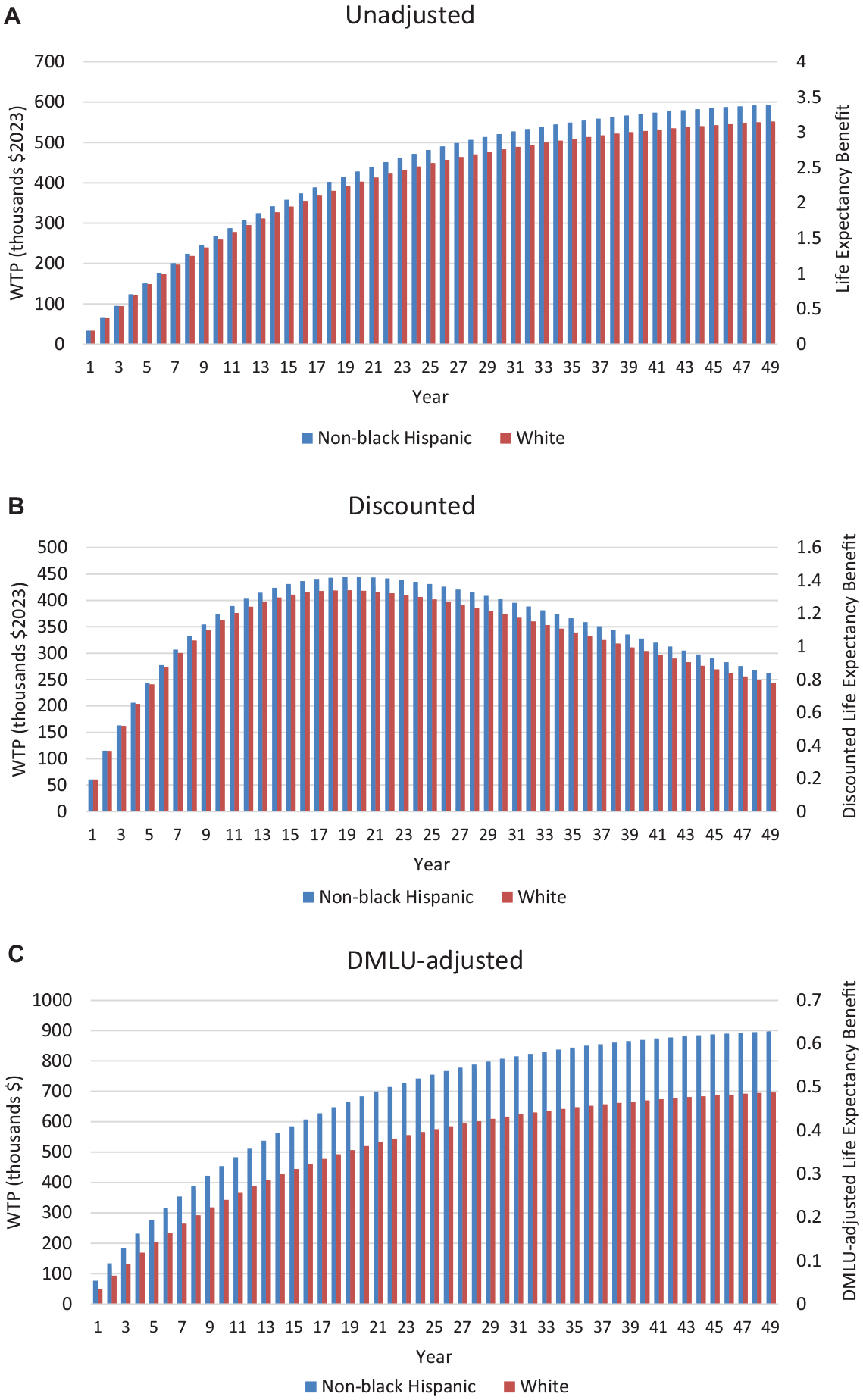
Results from a population-based model of survival in persons with cystic fibrosis, comparing life expectancy gain from additional resource investment in centers serving mostly non-Black Hispanic patients versus centers serving mostly White patients.
Incompatibility with Absolute Inequality Aversion
It is important to note that DMLU is inconsistent with any absolute inequality aversion measure (e.g., the Kolm index). DMLU implies that the value of an absolute difference in lifespan duration grows smaller as lifespan increases, whereas the use of an absolute inequality index presumes that this value remains constant. For example, any absolute inequality measure would similarly value a 3.5-y increase in the LE gap between non-Black Hispanic CF LE and White CF LE, whether produced by subtracting 3.5 y from non-Black Hispanic persons or adding 3.5 y for White persons. However, these alternatives should be valued differently if DMLU exists; subtracting 3.5 y from the baseline LE for non-Black Hispanics lowers their utility by 0.70 DMLU-adjusted life-years, substantially more than the 0.58 DMLU-adjusted life-years gain in utility for Whites if 3.5 additional life-years are added.
Biased Interpretation of Relative Inequality Aversion
Inequality aversion may occur for different reasons when a valued entity is distributed unequally, including both aversion to an unequal distribution of utility from that entity (e.g., prioritarianism) and aversion to a loss in aggregate utility if that entity is both distributed unequally and has diminishing marginal returns (i.e., utilitarianism). For example, it has been often noted that the most utilitarian distribution of income is one that is equal because money exhibits diminishing marginal return. 29 For this reason, if DMLU exists, empirical elicitations of inequality-aversion of lifespan gains may reflect a utilitarian aversion to loss of aggregate lifespan-related utility as well as a prioritarian aversion to unequally distributed lifespan-related utility.
Inequality aversion can be empirically elicited by identifying the tradeoff people are willing to make to reduce inequality, even if efficiency is reduced. For example, Robson et al. 26 found that respondents would accept a loss of 1.75 life-years to reduce the lifespan gap between lower and higher socioeconomic populations quintiles from 16.0 y to 11.5 y, a result that corresponds to an inequality-aversion parameter (ε) of 10.95.


Here, EDE is the equally distributed equivalent value of outcome y distributed across N measurements indexed by i, given a level of inequality aversion ε. When ε is zero, the EDE is simply the mean of the distribution. As ε increases, the EDE decreases from the mean of the distribution toward its minimum value.
However, it is unclear whether respondents making this tradeoff favored a utilitarian transfer of life-years from a group deriving lower marginal utility to a group deriving higher marginal utility, thereby increasing overall utility and/or they were averse to the unequal distribution of utility, favoring a prioritarian transfer of life-year–based utility from a group with higher baseline utility to a group with lower baseline utility. Accordingly, Robson et al.’s empirical elicitation (ε = 10.95) may reflect both utilitarianism and prioritarianism, rather than only one or the other. Indeed, it can be shown that the utilitarian component of the Robson tradeoff would produce an ε of 0.35, if DMLU is parameterized by a power function of 0.65.
Applying analogous thinking to the CF example, the existence of DMLU implies that adding 3.5 y to the lower LE of non-Black Hispanics would be valued more than adding 3.5 y to the higher LE of Whites. If DMLU is parameterized as a power function exponentiated to 0.65, it would be necessary to add only an additional 2.6 y to non-Black Hispanics to be valued similarly to adding 3.5 y to Whites, because both would add 0.58 DMLU-adjusted years. While these equivalent valuations correspond to an ε of 0.42 using equation (1), this ε would reflect only utilitarianism rather than prioritarianism, because it stems from a desire to raise aggregate health-related utility rather than from a desire to make the distribution of health-related utility more equal. On the other hand, levels of ε greater than 0.42 would reflect a prioritarian desire to make the distribution of health-related utility less unequal in addition to a utilitarian desire to maximize aggregate health-related utility.
For these reasons, empirically derived values of ε may not always be transportable. For example, it may be incorrect to transport Robson et al.’s empirically derived ε of 10.95 to the CF decision because the utilitarian component of ε in the Robson et al. scenario (0.35) differs from the utilitarian component of ε in the CF scenario (0.42).
DMLU Reinforces Questions about CEA Metrics That Employ Life-Years
While there is extensive literature on the suitability of life-year–based metrics for CEA, this literature has focused on QALYs rather than life-years and in particular has focused on the validity of the proportional tradeoff assumption37,38 (i.e., similar proportioned tradeoffs in life duration to avoid a utility decrement, regardless of lifespan duration). Considering DMLU broadens the discussion on the suitability of life-year–based CEA metrics beyond QALYs to encompass life-years, it may not make sense to use life-year, QALY, or any adjusted life-year metric if the time linearity implicit in these metrics is itself inconsistent with DMLU.
However, at the same time that DMLU challenges linear, life-year–based CEA metrics, it offers a way to reconceptualize them. A CEA metric incorporating DMLU could be normalized to an entire lifespan rather than to a particular number of years. I will illustrate one among many possible approaches. The distribution of life expectancies in a particular society at a particular time (T1) can be adjusted for DMLU, and then the EDE of their distribution can be calculated. This EDE of DMLU-adjusted life-years can be anchored to “1.” Subsequent changes in the health of that society will affect the distribution of life expectancies, which will then affect the distribution of their DMLU-adjusted life expectancies and ultimately their EDE of DMLU-adjusted life-years. This new EDE of DMLU-adjusted life-years at a later time (T2) can be compared with the prior value to determine whether health is improved, and that comparison will consider both DMLU and inequality aversion. However, this health improvement would no longer be conveyed by an EDE-adjusted life-years–gained metric, in units of years, but rather through an EDE-adjusted lives-gained metric, in units of lives. Analogous procedures could be applied to QALYs if the proportional tradeoff assumption is accepted. Because it may be argued that an equivalent-lives metric should not be anchored arbitrarily by the LE distribution and EDE of a particular society at a particular time, a more objective anchor could be chosen, such as the greatest health in a human population that is currently foreseeable, equally distributed (for example, perfect quality of life over a lifespan of 110–115 y, the asymptotic LE when extrapolating forward historical trends in age-adjusted mortality). 39
Other Considerations
It may be argued that societal valuations of lifespan extension have already been empirically assessed, for example, by differentially assessing willingness to pay for gains in survival, gains in quality of life, or both.20,38,40–45 According to this reasoning, because empirical assessments of lifespan extension encompass DMLU, it is unnecessary to further study or characterize DMLU. However, this reasoning omits insights that arise from identifying the unsuitability of using absolute inequality measures in distributive CEAs or from identifying the relative importance of prioritarian and utilitarian components of inequality aversion.
DMLU could further animate long-standing debates about whether QALYs are insufficiently ageist or too ageist,46–49 as lifespan extensions for older persons would be valued less than equivalent lifespan extensions for younger persons. Relatedly, many who view QALYs as insufficiently ageist also argue that nonwelfarist approaches to health valuation (e.g., fair innings or capacity theory) may be preferable to further modifications of CEA-based metrics,50–52 particularly since QALYs are sometimes presented as a generic measure of health divorced from the concept of utility. However, DMLU is of intrinsic importance to quantify the benefit of lifespan duration, which will always be a relevant input for CEAs. Further, scholars who are revising QALYs within a utility context, such as by incorporating descriptive insights from prospect theory, may find it useful to incorporate DMLU-adjusted lifespan.5,9,18 Finally, it is notable that inequality aversion is being incorporated into CEA within a welfarist framework and that fair innings has recently been formulated within a prioritarian welfarist framework. 53
Limitations
It may be argued that studies (Table 1) have not adequately parsed DMLU from individual discounting, and individual discounting may comprise the bulk of observed consequences I am attributing to DMLU. However, the implications for valuing equity in CEA would be the same because those individual discount rates would far exceed rates typically used in CEA. Accordingly, they would be incompatible with the low discount rates warranted by intergenerational CEAs, contradict the use of absolute inequality aversion measures, bias interpretation of relative inequality aversion parameters, and potentially create an implicit antiequity effect in CEAs.
This explication of DMLU has notable limitations. First, the literature review (Table 1) yielded studies that were too heterogeneous for quantitative pooling. Accordingly, it is uncertain whether and when the particular DMLU parameterization I chose (power function of 0.65) is better than others. Future studies may increase certainty regarding appropriate functional forms for DMLU parameterization. The approach outlined here does not harness rank-dependent approaches that more fully extricate DMLU from discounting, inequality aversion, and other phenomena.3,54 Finally, the practical value of this work would be greatly facilitated by future research 1) distinguishing DMLU from discounting, 2) studying plausible DMLU parameterizations, 3) estimating how DMLU adjustment affects willingness-to-pay thresholds, and 4) consideration of incorporating DMLU into CEAs in addition to the incorporation of discounting.
Conclusion
DMLU is likely to exist and has implications for valuing equity in CEA. When inequality aversion is not included in an analysis, omitting consideration of DMLU will have an implicit antiequity effect. When inequality aversion is considered, absolute indices of inequality should be avoided. Finally, empirical estimates of inequality aversion may be biased, making societies seem more prioritarian than they really are.
Footnotes
Acknowledgements
Mark S. Roberts, Distinguished Professor of Health Policy and Management at the University of Pittsburgh, offered valuable insights and ideas on how to improve the revision.
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The article was not generated from human subjects research and requires no ethical review/approval.
Consent to Participate
The article was not generated from human subjects research and requires no ethical review/approval. Research participants were not part of the process, and no consent was applicable.
Data Availability
The scientific literature reviewed for this article is publicly available. Excel code will be made available upon request to Dr. Braithwaite.