
Abstract
Highlights
Stressors in hospital settings such as the complexity and uncertainty of tasks create stress among physicians, potentially leading to decision conflicts.
Team support plays a fundamental role in mitigating the negative effects of stressors such as time pressure and uncertainty.
Implementing stress management and team support interventions such as cognitive-behavioral therapy and mindfulness may enhance decision making among Obs and Gynae physicians.
Keywords
Introduction
Decision-making research in high-risk settings 1 has extensively investigated the individual influences of uncertainty, time pressure, perceived stress, and team support. However, a significant research gap exists in understanding their combined impact in influencing decision outcomes. This study uniquely addresses this gap by investigating the perceptions of obstetrics and gynecology (Obs and Gynae) physicians in the context of provider decision process assessment. Obs and Gynae deals with a broad range of intrinsically complex clinical situations and illnesses. These intricacies frequently result in complex decision-making processes that are affected by a number of variables, including patient characteristics, medical record, and contextual circumstances.2,3 Critical and time-pressured situations in Obs and Gynae demand accurate and prompt decisions for the well-being of mothers and unborn children. With an emphasis on high-risk pregnancies, this profession includes handling complications during labor, such as emergency cesarean sections,4,5 as well as prenatal screening, monitoring, and interventions for gestational diabetes, preeclampsia, and fetal abnormalities.
The study employs the naturalistic decision-making (NDM) theory, 6 which offers valuable insights into the decision-making processes of obstetricians and gynecologists under complex and demanding conditions, such as high-risk pregnancies. We also used structural equation modeling (SEM), 7 since it enables the simultaneous modeling of the distinct contributions of predictors, mediators, and outcome variables. Moreover, SEM addresses measurement errors in observed variables, enhancing analysis accuracy and evaluating model-data fit, ensuring validity in representing decision-making processes.
Theoretical Framework
The theory of NDM8,9 provides a paradigm for comprehending decision making in high-stress settings, including the medical field. Dolan’s work on provider decision process assessment, 10 which emphasizes the importance of decision-task elements including uncertainty and time pressure, is in line with NDM concepts. Within the framework of Dolan’s methodology, the study intends to investigate how these factors—in accordance with NDM principles—collectively affect decision outcomes, emphasizing the complex interactions among stress, team support, and decision process assessment.
In the field of Obs and Gynae, health care providers often encounter uncertain situations with no clear plan of action.11,12 NDM suggests that in order to effectively traverse unpredictable and dynamic situations, decision makers rely on their knowledge, experience, and intuition.8,9 Health care professionals must constantly evaluate the mother’s and the infant’s health, foresee any problems, and modify their course of action as necessary. Managing women’s reproductive health and pregnancy-related care can be complex, which may lead to decision conflict in various situations. For instance, in situations in which a pregnant woman is dealing with multiple medical conditions or complications, such as pre eclampsia, gestational diabetes, or placental abnormalities, health care providers may need to make tough choices. 13 Conflicts can arise from discrepancies between competing goals. These conflicts may affect decision quality and the ability to reach consensus within a team, highlighting the importance of understanding and managing conflict in decision-making contexts. Physicians may employ various coping mechanisms, such as consulting with colleagues, seeking additional information, or relying on past experiences to navigate uncertainty and make informed decisions. Effective teamwork can help mitigate the negative impact of stress and uncertainty on decision outcomes, 14 promoting collective sensemaking and adaptive decision-making strategies.
Provider Decision Process Assessment
Provider decision process assessment is divided into 2 types: satisfaction with decision process and conflict with decision process. In the realm of Obs and Gynae, decision makers frequently choose the course of action that will be sufficient to satisfactorily resolve the situation rather than always choosing the best or optimal approach. 15 These desired outcomes set a rule that stops further searching and act as guiding principles in decision making under uncertainty. 16 In addition, obstetricians and gynecologists rely on evidence-based methods, best practice standards, and decision-making algorithms on a daily basis. 17 Guidelines may suggest a systematic strategy in eclampsia situations, for example, which involves monitoring the woman and baby closely, administering anticonvulsant drugs, and, if necessary, considering emergency treatments like cesarean sections. These recommendations, which support practitioners in making well-informed decisions to maximize outcomes for mother and child, are based on extensive research and clinical expertise.
In emergency situations, decision outcomes can be used as a criterion to judge the effectiveness of decisions. We consider Obs and Gynae physicians’ perceptions of decision making including satisfaction, conflicts, and uncertainty, as these elements are intertwined and influence decision processes. The decision uncertainty creates stress 15 among physicians, which affects the overall decision process assessment. Physicians proactively engage in adaptive responses to cope with perceived stress, a dynamic process influenced by the specific stressors they encounter.18,19
Sources of Perceived Stress
Uncertainty
In Obs and Gynae, uncertainty always accompanies critical, stressful, and dynamic scenarios. Therefore, it has a multifaceted impact on decision making. 20 According to Klein, 9 if the inevitableness of uncertainty is recognized, decision makers can use their knowledge in a better way to concentrate and work on the task. Within the NDM paradigm, the recognition that uncertainty is an inherent part of the Obs and Gynae landscape allows physicians to navigate uncertainty with a refined skill set. This recognition, however, also introduces stress among physicians and has the potential for conflict in decision making. In Obs and Gynae scenarios such as managing a ruptured uterus, physicians encounter rapidly changing situations requiring decisions to improve the overall situation. This involves action feedback loops, 21 in which actions are taken, feedback on consequences is received, and future decisions are informed by this feedback. For example, during a ruptured uterus emergency, a physician adjusts their approach based on patient response, integrating outcomes into their ongoing management plan. This iterative process is essential for effective decision making in unpredictable situations, in which inherent uncertainty introduces stress and potential conflicts. 22 Based on these observations, we propose the following hypotheses.
H1: There is a direct relationship between uncertainty and conflict with decision.
H1a: There is an indirect relationship of uncertainty on conflict with decision through perceived stress.
Time Pressure
Time pressure, often overlooked in Obs and Gynae decision-making studies, is crucial in uncertain situations. For instance, sudden complications during childbirth require immediate intervention. Factors such as event duration, complications, delays in obtaining critical information, and the need for swift data processing contribute to heightened time pressure.23,24 This pressure leads to less cognitive processing, increasing the risk of misinterpretation and conflict. 25 Hence, it is proposed that:
H2: There is a direct relationship between time pressure and conflict with decision.
H2a: There is an indirect relationship of time pressure on conflict with decision through perceived stress.
Understanding the interplay between perceived stress, sources like uncertainty and time pressure, and adaptive responses is crucial for comprehending how individuals cope with challenges and make decisions in demanding situations. Research in this field enhances our understanding of stress management and resilience, offering insights into strategies for effectively addressing uncertainty’s impact on well-being and decision making. One notable coping strategy that emerges is the team support.
Team support
Collaboration among Obs and Gynae professionals is crucial for handling complex and uncertain cases, improving diagnostic skills through team-based decision making and diagnostic tools using electronic health record data. 26 This teamwork is influenced by interpersonal relationships, power dynamics, and quality management practices. Despite its importance, there is a lack of thorough studies linking team training programs to patient outcomes. The current approach focuses on improving team dynamics through targeted training. 27 While collaboration among senior physicians reduces uncertainty and enhances decision satisfaction, there remains a gap in linking these efforts to tangible patient outcomes. 28 Based on the literature, the following can be proposed:
H3: There is a direct relationship between uncertainty and satisfaction with decision.
H3a: There is an indirect relationship of uncertainty on satisfaction with decision through team support.
Teams can mitigate time pressure by efficiently organizing work and limiting tasks per individual. High time pressure can dampen enthusiasm and hinder action, emphasizing the need to manage it effectively ensuring that motivation and productivity remain intact. Under time pressure, teams may experience stress leading to passivity, decision conflicts, or avoidance. Fostering a collaborative team culture with fair task distribution eases time constraints, fostering teamwork and a sense of togetherness that alleviates stress. 29 Thus, it is proposed that:
H4: There is a direct relationship between time pressure and satisfaction with decision.
H4a: There is an indirect and positive association of time pressure on satisfaction with decision through team support.
In hospital settings, physicians value team support and the quality of services from team members as crucial aids in decision making. However, in Obs and Gynae, limited research investigates the links between stress, team support, and provider decision process assessment among physicians. Therefore, the primary research question of the study is: How do perceived stress and team support explain the relationship between predictors (uncertainty, time pressure) and outcome variables (satisfaction with decision/conflict with decision).
Method
Research Design and Sample
We employed a cross-sectional study design, using correlational analysis to examine variable relationships. Data were gathered from Obs and Gynae physicians across various hospital settings, including labor rooms, maternity wards, outpatient departments, obstetric emergency departments, and doctors’ offices. Purposive convenience and snowball sampling methods were used, targeting individuals with diverse work experience and employment functions. We used personal networks and existing contacts, leveraging snowball sampling to reach physicians who were otherwise difficult to access.
The suggested sample size
30
for SEM was 137, but we collected data from 347 physicians across public, private, and semi-public sectors. Their ages ranged from 24 to 60 (
Measures
Given that English is the official language of Pakistan and physicians possess strong English proficiency, all measures were administered in English, eliminating the need for translations. Participants were informed that they regularly encounter complex cases and were asked to recall recent cases, such as managing a patient with eclampsia or performing a hysterectomy, to respond to questionnaire items based on their experiences.
Our selection of measures was guided by various considerations aimed at capturing key constructs relevant to our research objectives. We conducted a thorough analysis of research literature and theoretical frameworks, including the NDM theory, to identify major variables influencing decision making in Obs and Gynae. We prioritized measures with established validity and reliability in similar settings to ensure the quality of our results. Practicality and feasibility were also considered, taking into account factors such as responder burden, ease of administration, and relevance to the intended audience.
Perceived Stress Scale
Cohen et al. 32 developed the Perceived Stress Scale, which was recently validated by Lee and Jeong. 33 The scale is a 10-item measure used to assess stress levels among the population of physicians. The scale measures how much a person feels that life is overwhelming, unpredictable, and uncontrollable. It is rated from never (0) to very often (5) on a 5-point Likert-type scale. The scale has adequate psychometric properties, in which the Cronbach alpha value is 0.87 with an established cutoff of 0.70.
Team Support
Team Support was developed by Batorowicz and Shepherd 34 to measure teamwork as a support in decision-making process. We used a 5-item subscale of team decision-making support. The scale is scored using a Likert-type scale with a range of 1 (not at all) to 7 (to a great extent). Strong internal consistency and reliability of the scale are reported, as the Cronbach alpha lies within 0.83 to 0.91.
Provider Decision Process Assessment
Dolan 10 developed a 12-item questionnaire called the Provider Decision Process Assessment (PDPA), which assesses a health care professional’s level of comfort in making medical decisions. The usefulness of using the PDPA depends on whether it is appropriate to evaluate a decision in light of the process involved in its formation. The scale has sufficient alpha reliability (α = 0.79), and participants rated their responses on a 5-point Likert-type scale, ranging from strongly agree (5) to strongly disagree (1). It has 2 subscales: Satisfaction with Decision and Conflict with Decision. There are 5 reverse-scored items, and the maximum possible score range is 12 to 60.
Decision-Making Questionnaire
In this study, we used the Decision-Making Questionnaire (DMQ) task factor, as developed by Lizarraga et al., 35 to assess the significance of variables influencing individuals’ decision-making processes. Specifically, we focused on variables related to the actual nature of the decision, such as time pressure (α = 0.78) and uncertainty (α = 0.76) associated with each alternative. The DMQ task factor underwent adaptation for our study through both exploratory and confirmatory factor analyses. Given that the questionnaire was not originally tailored for Obs and Gynae physicians, its suitability was ensured via rigorous validation encompassing content, construct, and criterion validity assessments.
Participants rated the importance of the task variable on a Likert-type scale ranging from 1 to 9, with 1 indicating the lowest importance and 9 indicating the highest importance. The reliability of the adapted DMQ task factor was assessed using Cronbach alpha coefficients, with values of 0.78 for time pressure and 0.76 for uncertainty.
Procedure
Data collection occurred from September 2022 to January 20, 2023, in both private and public sector hospitals. Permission to collect data was sought from the head of the obstetrics and gynecology department at each hospital. Prior to data collection, participants were provided with informed consent and briefed on the study’s objectives. Voluntary participation was ensured, with participants given the right to withdraw if they felt uncomfortable. Confidentiality of responses was guaranteed, and collected data would be used solely for educational and research purposes. Institutional ethical approval was obtained before data collection (Ref. No. 0988/Ethic/01/S3H/070/DBS).
Data Analysis
The study rigorously addressed multicollinearity using Variance Inflation Factor (VIF) analyses, ensuring values remained below the threshold of 5. Correlation analyses assessed variable relationships, while advanced SEM in AMOS software investigated the indirect effects of perceived stress and team support on decision outcomes.
Results
Table 1 presents the mean, standard deviation, coefficient of skewness, coefficient of kurtosis, values of range, and Cronbach alpha reliability of the study’s scales and subscales. The table indicates that all of the scales and subscales have adequate reliabilities greater than 0.70. The appropriate dispersion of scores is indicated by skewness and kurtosis values within the range of +1 to −1.
Descriptive Statistics and Reliabilities of the Sample for the Main Study Variables (N = 347)
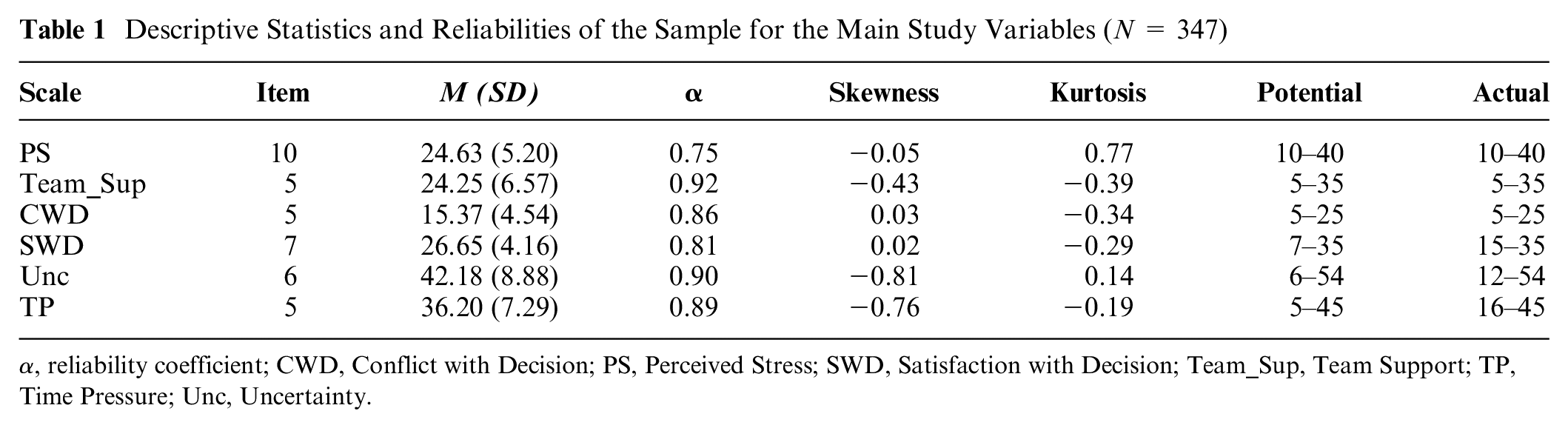
α, reliability coefficient; CWD, Conflict with Decision; PS, Perceived Stress; SWD, Satisfaction with Decision; Team_Sup, Team Support; TP, Time Pressure; Unc, Uncertainty.
Correlation Analysis
According to Gignac and Szodorai’s guidelines, 36 effect sizes between 0.10 and 0.29 are considered small. In our analysis, we found small effect sizes among positive and negative constructs such as perceived stress and satisfaction with decision. However, a medium effect size was observed among positive constructs such as satisfaction with decision and team support.
Table 2 outlines associations among all study variables. Stress showed a significant positive relationship with uncertainty (r = 0.14**) and satisfaction with decision (r = 0.13*), indicating that physicians experiencing higher stress perceive situations as more uncertain or ambiguous. Perceived stress had a significant negative relationship with decision process assessment (r = −0.23*) and conflict with decision (r = −0.44**), suggesting that higher stress levels were associated with a less favorable assessment of the decision-making process. However, the magnitude of the effect was small. Perceived stress had a nonsignificant relationship with team support (r = 0.08) and time pressure (r = 0.09).
Coefficient among all Variables of the Study (N = 347)

CWD, conflict with decision; PS, perceived stress; SWD, satisfaction with decision; Team_Sup, team support; TP, time pressure; Unc, uncertainty.
P < 0.05, **P < 0.01. All correlations greater than 0.14 are significant to the P < 0.01 level, unless specified otherwise.
Conflict with decision showed a significant positive relationship with decision process assessment (r = 0.74**) and time pressure (r = 0.16**), indicating that higher conflict was associated with a less favorable assessment of the decision-making process. However, the effect size was small. Conversely, satisfaction with decision showed a significant positive and moderate relationship with decision process assessment (r = 0.68**), uncertainty (r = 0.36**), and time pressure (r = 0.36**), suggesting that physicians who were more satisfied with their decisions still operated under moderate uncertainty and time pressure. Decision process assessment had a significant positive relationship with uncertainty and time pressure.
Structural Model Assessment
The relationships among variables were examined by using a structural model equation created with AMOS (see Figure 1). The model assessed the mediating role of perceived stress and team support on the relationship between 1) uncertainty and conflict with decision, 2) time pressure and conflict with decision, 3) uncertainty and satisfaction with decision, and 4) finally time pressure and satisfaction with decision, respectively.

Structural equation model showing the indirect effect of perceived stress and team support on uncertainty, time pressure, conflict, and satisfaction with decision.
Results reveal sufficient values of the model’s fit indices (comparative fit index [CFI] = 0.94, Tucker-Lewis index [TLI] = 0.97, incremental fit index [IFI] = 0.98, and root mean squared error of approximation [RMSEA] = 0.053). Moreover, the squared multiple correlation was 0.239 for conflict with decision, demonstrating that uncertainty and time pressure account for 24% of the variance in conflict with decision. This highlights the significance of these factors in predicting and understanding the level of conflict experienced in the decision-making process. However, the squared multiple squared correlation was 0.268 for decision satisfaction; this demonstrates that uncertainty and time pressure account for 27% of the variance in decision satisfaction. The summary of the mediation analysis is shown in Table 3.
Mediation of Perceived Stress and Team Support between Uncertainty, Time Pressure, Conflict with Decision, and Satisfaction with Decision (N = 347)

Note: Unc = Uncertainty; PS = Perceived stress; TP = Time pressure; Team_Sup = Team support; CWD = Conflict with decision; SWD = Satisfaction with decision; β = coefficient (effect size); *p < 0.05; **p <.01: ***p < 0.001
Hypothesis (H1a) is supported as results show a significant indirect relationship of perceived stress between uncertainty and conflict with decision (b = −0.033, P < 0.001). This suggests that the relationship between uncertainty and conflict with decision is influenced by the mediating role of perceived stress, with the observed relationship being small in magnitude. Moreover, the presence of a mediator does not diminish the significant direct relationship of uncertainty on conflict with decision.
Furthermore, H1 is also supported as the direct relation of uncertainty on conflict with decision in the presence of mediator is also significant (b = 0.108, P < 0.05). Therefore, the relationship between uncertainty and conflict with decision is partially mediated by perceived stress.
Hypothesis (H2a) is not supported as a nonsignificant indirect relationship of perceived stress is found between uncertainty and satisfaction with decision (b = 0.005, P > 0.05). Furthermore, the nonsignificant indirect relation of perceived stress between time pressure on conflict with decision (b = −0.028, P > 0.05) and time pressure on satisfaction with decision (b = 0.005, P > 0.05) is found. Hence, H2 is also not supported. Based on the findings, it can be inferred that there is no mediation of perceived stress in the relationship between time pressure and conflict with decision as well as time pressure and satisfaction with decision.
Hypotheses H3a and H4a are supported as team support has a significant indirect relationship between uncertainty and satisfaction with decision (b = 0.082, P < 0.05) as well as between time pressure and satisfaction with decision (b = 0.086, P < 0.05). As uncertainty or time pressure increases, team support becomes a crucial factor influencing higher satisfaction with decision. This suggests that a supportive team environment can mitigate the negative impact of time pressure and uncertainty, contributing to increased satisfaction with decision-making processes.
Moreover, hypotheses (H3 and H4) are also supported as a significant direct relationship of uncertainty on satisfaction with decision (b = 0.086, P < 0.05) as well as between time pressure and satisfaction with decision (b = 0.108, P < 0.05) also exists in the presence of a mediator. This demonstrates the complexity of decision-making processes and emphasizes how crucial it is to take into account both direct and indirect relationships when analyzing the variables that influence decision satisfaction within the context of the study. Moreover, the path between uncertainty and conflict with decision (b = −0.004, P > 0.05) as well as time pressure and conflict with decision (b = −0.008, P > 0.05) is also not mediated by team support.
Discussion
The study investigated the mediating role of perceived stress and team support between uncertainty, time pressure (predictors), conflict with decision, and satisfaction with decision (outcomes) through SEM. The study initially examined relationship patterns among variables through bivariate correlations, revealing moderate associations among positive constructs and smaller associations with opposing constructs such as team support and decision conflict. These findings guided further investigation into predictors and mediators. SEM was then conducted to assess model fit, using indices such as the CFI, TLI, IFI, and RMSEA. Adequate fit was confirmed (see Supplementary Table).
The major findings of the study indicated that the higher the uncertainty, the higher the perceived stress will be, which is also supported by previous studies. 37 Moreover, in the presence of team support, the results revealed a significant mediation effect between uncertainty and satisfaction with decision and time pressure and satisfaction with decision (see Table 3). Hence, H3a and H4a are supported. Our findings illuminate the pivotal role of fostering a supportive team support 38 in mitigating the negative effects of uncertainty and time pressure on decision satisfaction. This highlights the importance of fostering a supportive workplace environment, not only for the well-being of health care professionals but also for enhancing decision-making effectiveness. Our research not only enriches existing knowledge but also addresses critical gaps by investigating the combined influence of uncertainty, time pressure, stress, and team support within a single model. This comprehensive approach provides a clearer understanding of how these factors interact to affect decision outcomes in health care. Previous studies39,40 also complement our findings that have found a positive influence of multidisciplinary teams on individuals’ decision making in health care settings.
It is important to mention that we obtained significant but small to negligible effect sizes in our model. Despite the theoretical basis within NDM, the relationships among perceived stress, uncertainty, conflict with decision, satisfaction with decision, and team support may be influenced by numerous interacting factors. The complexity of human cognition, behavior, and the dynamic nature of decision-making processes 41 can lead to nuanced interactions that may not be fully captured by traditional statistical models. NDM suggests that decision making is influenced by complex situational factors and interactions between variables.6–8 This complexity may result in smaller effect sizes, as the direct relationships between variables may be overshadowed by indirect relationships that are not adequately captured by traditional linear modeling approaches. The observed small effect sizes in our results may be attributed to collinearity and the influence of confounding factors. Collinearity, arising from high correlations among predictor variables, can inflate standard errors and diminish the precision of parameter estimates. This can obscure the true magnitude of relationships between variables. In addition, confounding factors, unaccounted for in our analysis, may have influenced the observed associations, leading to attenuated effect sizes. Addressing collinearity through techniques such as multicollinearity diagnostics and variable selection, and controlling for confounding through statistical methods such as stratification or regression adjustment, could mitigate these issues in future studies.
Moreover, time pressure does not predict perceived stress; hence, there existed no mediation between time pressure, perceived stress, and decision process assessment. Therefore, hypothesis (H2) is not supported. The reason could be that health care professionals are resistant to stress and other unfavorable psychological effects due to their high resilience. 42 The other reason is that Obs and Gynae physicians may have learned the art of decision making under stress. Studies have reported43,44 that physicians working in emergency departments are prone to stressful cases on a daily basis; hence, they become immune to perceived stress. However, some studies show they do not become immune to but rather are more prone to developing mental health problems. 45 Most of the tasks involve time pressure; therefore, working under stress has become their professional task. They make decisions in time-constrained naturalistic settings without getting affected by stress. This may be the reason that no mediation of perceived stress is found between time pressure, perceived stress, and decision-process assessment.
In addition, there existed no mediation between uncertainty, perceived stress, and satisfaction with the decision. The reason is obvious that challenging situations and a stressful environment promote more conflict rather than satisfaction with decision. Hence, a significant effect was not found. Furthermore, there existed no mediation between uncertainty, team support, and conflict with decision. Similarly, there existed no mediation between time pressure, team support, and conflict with decision.
Implications
The findings of the present study suggest that implementing psychological interventions focused on stress management and team support could significantly enhance the decision-making process among Obs and Gynae physicians. Specifically, interventions aimed at reducing perceived stress levels, such as cognitive-behavioral therapy techniques or mindfulness-based stress reduction programs, may help mitigate the negative impact of uncertainty on decision making and decrease conflict with decision. Moreover, fostering a supportive team environment through initiatives such as regular debriefing sessions, communication training, and team-building exercises could strengthen the positive effect of team support on decision satisfaction, specifically in the face of time pressure and high workload demands. In addition, providing opportunities for mentorship and peer support within the specialty could further enhance team collaboration and cohesion.
Limitations
The study collected data from only Obs and Gynae physicians due to limited resources and personal constraints. However, for more conclusive evidence on team support as a mediator, it is necessary to include physicians from other departments such as surgery, medicine, and so forth. In addition, we used snowball sampling, which may not provide a representative sample, limiting the applicability of study results to broader populations. Furthermore, SEM can reveal associations between variables but cannot determine causal relationships, limiting the ability to draw definitive conclusions about cause and effect. The small effect sizes may not be practical and limit implications to real-world contexts. Moreover, the study found time pressure and uncertainty explain a notable portion of both decision conflicts (24%) and satisfaction (27%). However, most remaining variances (76% and 79%, respectively) suggest the presence of other influential factors. This underscores the need for further research to comprehensively understand these additional components and their role in the decision-making process.
Conclusion
The study found the potential mediating role of perceived stress team support between uncertainty, time pressure, and satisfaction with decision among Obs and Gynae physicians. The findings have the potential to guide future interventions and initiatives targeted at strengthening decision-making procedures and raising the standard of care in high-stress medical environments.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241273575 – Supplemental material for Examining the Role of Stress and Team Support in Decision Making under Uncertainty and Time Pressure
Supplemental material, sj-docx-1-mpp-10.1177_23814683241273575 for Examining the Role of Stress and Team Support in Decision Making under Uncertainty and Time Pressure by Sana Younas and Saeeda Khanum in MDM Policy & Practice
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval Statement
The Institutional Review Board of the Department of Behavioral Sciences, School of Social Sciences and Humanities, NUST, has permitted to conduct this study (Ref. No. 0988/Ethic/01/S3H/070/DBS). Participants were fully informed and consented to investigate and publish the findings of the study.
Consent to Participate
Informed consent was obtained from all participants included in the study.
Consent for Publication
Participants gave their consent for the publication of their data, provided that their identity will not be revealed.
Data Availability Statement
Data could be provided on request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.