
Abstract
Highlights
This is a visual representation of the abstract.
Each year in the United States, the parents of approximately 40,000 children are told that their child has congenital heart disease (CHD). 1 Although most children with a CHD diagnosis are now expected to live long and active lives,1–3 diagnoses of clinically complex CHDs (e.g., hypoplastic left heart syndrome or a single ventricle with heterotaxy) remain associated with poorer mortality, morbidity, and life expectancy.4,5 Given the severity and uncertainty of these outcomes, termination, comfort-directed care, and surgery may be presented as potential treatment options for parents to consider.
There has been increasing recognition that the diagnosis and experience of complex CHD in the fetus can have a significant impact on parental well-being.2,6–18 Numerous studies have shown that parents report high levels of emotional and psychological distress as they come to terms with the diagnosis and their role in making difficult treatment decisions for their fetus (possible decision options available to parents include termination, comfort-directed care, or surgery).2,6–10 Participation in this decision making has also been shown to be challenging for parents given the quantity and complexity of information (e.g., regarding diagnosis, treatment, and prognosis), the uncertainty surrounding the outcome of certain treatments (e.g., surgical or catheter-based treatments), the impact of their decision on the health and well-being of the child and the family, and the limited time frame in which these processes occur.2,11,12,15,16 Moreover, the negative outcomes associated with these experiences may continue after diagnosis, as studies have shown increased parental distress presents 6 to 12 mo after diagnosis13,14 and decreased parental well-being is documented as long as 3 y after birth. 10
Establishing a comprehensive understanding of parents’ emotional and psychological distress while making and reflecting on their decisions is critical to inform and develop effective interventions to assist in parental decision making and support their coping and well-being. Research examining differences in the needs and experiences of parents based on factors such as the timing13,14,19 and severity of the diagnosis10,20,21 has offered valuable insights for developing supportive interventions for parents and their families specific to these situations. However, most studies have included only parents who have chosen a particular treatment (e.g., either surgery or comfort-directed care). In addition, parents’ feelings of conflict or regret regarding their decisions may also have a significant impact on their psychological well-being22–24 but remain understudied in this context. Thus, we have a limited understanding of potential differences in parents’ psychological and decision-making outcomes that may arise based on their treatment approach (i.e., whether they chose termination, comfort-directed care, or surgery). There is also a gap in the literature, in the case of surgical intervention, on how parents’ psychological and decision-making outcomes may differ depending on whether or not the child survived following surgery.
A better understanding of how parents’ reported psychological and decision-making outcomes differ based on their approach to their child’s treatment and the treatment outcome would provide further opportunities for tailoring care and contribute to more optimal support for parents. The key objective of this exploratory study was to compare reported psychological distress, grief, conflict, and regret among parents whose fetus was diagnosed with a complex CHD based on their treatment decision and the survival outcome for the child.
Methods
This study was approved by the Institutional Review Board at the University of Utah (IRB_0010394). Between September 2018 and December 2020, we prospectively recruited parents with a fetus or neonate diagnosed with a complex life-threatening CHD (whether prenatally or postnatally) at a quaternary children’s hospital in the Intermountain West (Figure 1). Parents were considered eligible if the diagnosing provider and care team felt the severity of the CHD (e.g., hypoplastic left heart syndrome) warranted consideration of options such as termination, comfort-directed care, or intervention (this primarily entailed postnatal surgical intervention, although those eligible for an initial fetal intervention were also included). Comfort-directed care encompassed focusing on providing care to relieve suffering and improve quality of life, without prolonging life in those with a life-limiting or life-threatening diagnosis. Parents were enrolled after diagnosis and prior to their definitive treatment decision.

Flow diagram of the recruitment for the study sample.
Procedure
Parents enrolled in the study were asked to complete a self-administered survey 3 mo after their treatment decision as part of the observational control group for a larger survey-based evaluation study of a decision aid. 25 Parents decided whether they preferred to receive a paper survey by mail or complete a redcap online survey. Full descriptions of all study procedures, outcome measures, and time points of data collection are detailed in the protocol paper associated with this study. 25 For this study, we focused on 8 validated outcome measures (psychological distress, 26 perinatal grief, 27 depression, anxiety, hostility, interpersonal sensitivity, decisional conflict, 22 and decisional regret 23 ).
Measures
To measure overall psychological distress, we used the Global Severity Index from the Brief Symptom Inventory (BSI), 26 a validated scale of 53 items answered on a 5-point Likert-type scale (0 = not at all to 4 = extremely). The BSI measures 9 domains, but for the purposes of this study, we focused on 4 domains: depression (e.g., “Feeling hopeless about the future”; α = 0.90), anxiety (e.g., “Nervousness or shakiness inside”; α = 0.68), hostility (e.g., “Temper outbursts that you could not control”; α = 0.67), and interpersonal sensitivity (e.g., “Feeling inferior to others”; α = 0.81). We used the short Perinatal Grief Scale, which measures symptoms of grief after perinatal loss on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree; α = 0.94). Items on the grief scale were adapted for the present study to query parents whose child survived (27 items: e.g., “I am grieving because of the health of my child”; α = 0.96). 27
To better understand parents’ reflections about their treatment decisions, we also measured decisional conflict, which captures feelings of uncertainty about decisions associated with risky and uncertain outcomes as well as outcomes that may yield significant benefits or harms (16 items: e.g., “I am clear about the best choice for me”; α = 0.97), 22 and decisional regret, which captures feelings of remorse-related distress following health care decisions (5 items: e.g., “I regret the choice that was made”; α = 0.93) 23 using previously validated measures. Conflict and regret questions were answered on a 5-point scale (1 = strongly disagree to 5 = strongly agree). To align with the scale user manuals,28,29 responses were reversed so that higher scores correspond to greater conflict and regret, then transformed to range from 0 to 100.
Statistical Analysis
Analyses were conducted in R Studio Version 1.4.1106. 30 Due to the small sample size, formal statistical comparisons of between-group effects would provide limited informational value. Instead, using the rstatix package, 31 we report estimated mean differences between groups with 95% confidence intervals and describe the direction of the difference as well as whether or not the accompanying confidence intervals are consistent with no effect (i.e., whether or not the confidence intervals include zero). These are exploratory analyses from a larger survey-based evaluation study of a decision aid 25 and were not conceived a priori.
We made 4 comparisons for each of the 8 outcome measures: 1) comfort-directed care versus surgery, 2) comfort-directed care versus surgery (child survived), 3) comfort-directed care versus surgery (child did not survive), and 4) surgery (child survived) versus surgery (child did not survive).
Results
Sample Characteristics
Of the 35 parents who were enrolled in the study, 24 parents (including 5 parent pairs) completed the survey (completion rate = 69%). Only 1 case recruited was diagnosed postnatally; the parents decided on surgery, and the child survived. Since their experiences likely differ from prenatally diagnosed families (e.g., there was a much shorter duration of time between diagnosis and decision), 14 they were not included in the analyses, leaving a final sample of 23 parents. None of the families enrolled were eligible for fetal intervention. Of the 11 parents enrolled who were lost to attrition, their treatment decisions were distributed as follows: palliative care (n = 3), surgery (n = 7), and fetal demise (n = 1).
The mean age of the parents in our sample was 27 y (s = 4 y), with a median age of 26 y (range: 21–37 y) (Table 1). Most parents completing the survey were women (n = 18, 78%), non-Hispanic White (n = 20, 87%), and married (n = 21, 91%). Most parents decided on surgery (n = 16, 70%); in 11 cases, the child was alive at time of the 3-mo follow-up survey, and in 5 cases, the child had not survived. The remaining 7 parents (30%) decided on comfort-directed care, and in all cases, the child was not alive at the time of the 3-mo follow-up survey. None of the parents in the study chose termination.
Baseline Parent Characteristics Overall and according to Treatment Decision and Outcome a

CHD, congenital heart defect.
Plus-minus values are means ± standard deviation.
Comfort-Directed Care (n = 7) versus Surgery (n = 16)
Parents who decided on comfort-directed care reported higher levels of psychological distress (mean difference estimate = 0.77; 95% confidence interval [CI] = 0.05–1.48), perinatal grief (difference = 27.18; 95% CI, 6.20–48.16), and interpersonal sensitivity (difference = 1.12; 95% CI, 0.08–2.17) compared with parents who decided on surgery (Figure 2 and Table 2). The CIs for the differences in reported depression (difference = 0.73; 95% CI, −0.20 to 1.65), anxiety (difference = 0.65; 95% CI, −0.19 to 1.49), hostility (difference = 0.16; 95% CI, −0.36 to 0.69), decisional conflict (difference = 8.58; 95% CI, −6.35 to 23.51), and decisional regret (difference = 14.55; 95% CI, −0.04 to 29.15) between parents who decided on comfort-directed care and those who decided on surgery were consistent with no effect.
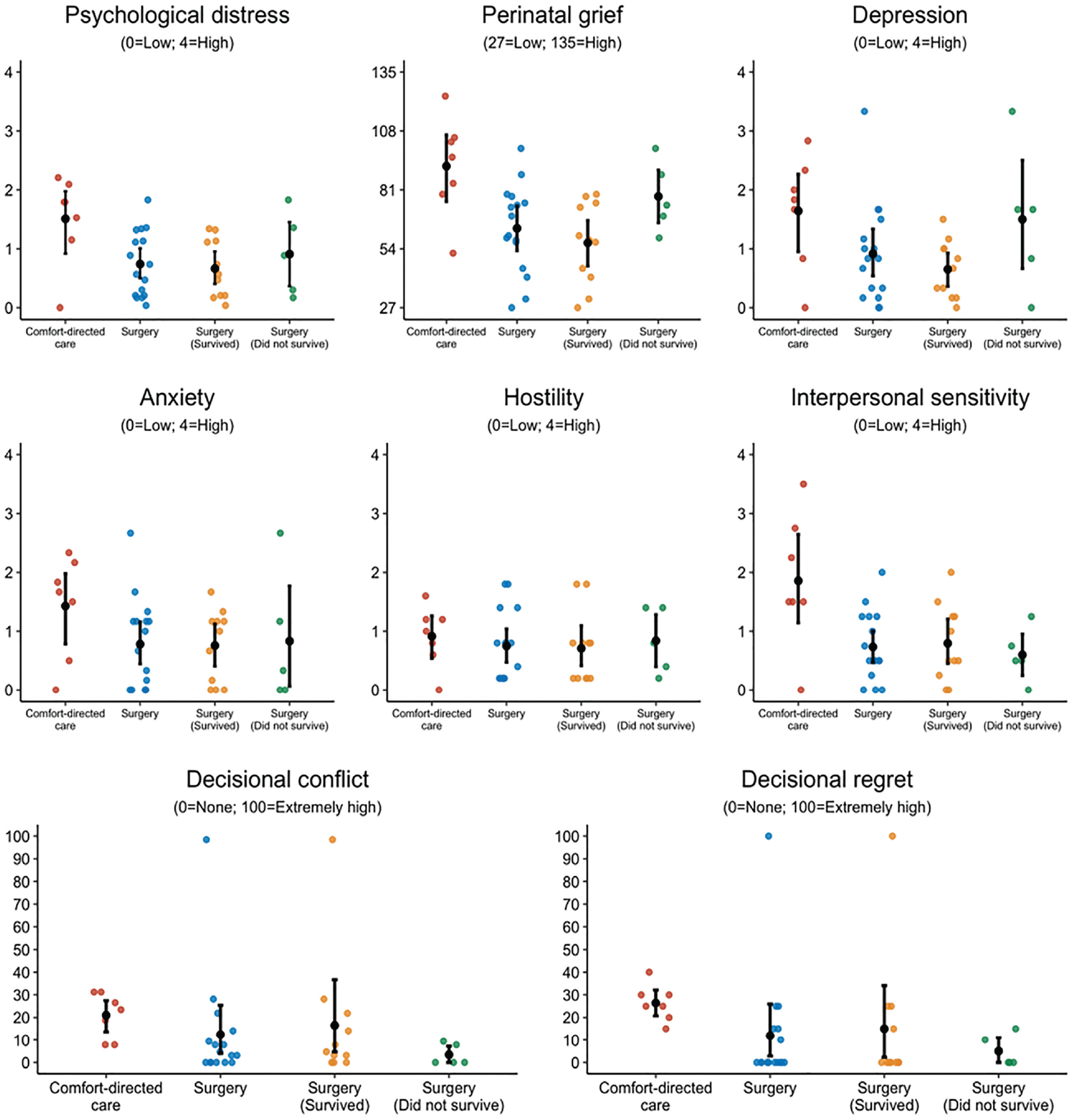
Parents’ responses to the study outcome measures according to treatment decision and outcome. The middle black point represents the mean, with error bars representing 95% confidence intervals.
Outcome Measures at 3-mo Follow-up, according to Treatment Decisions and Outcomes a
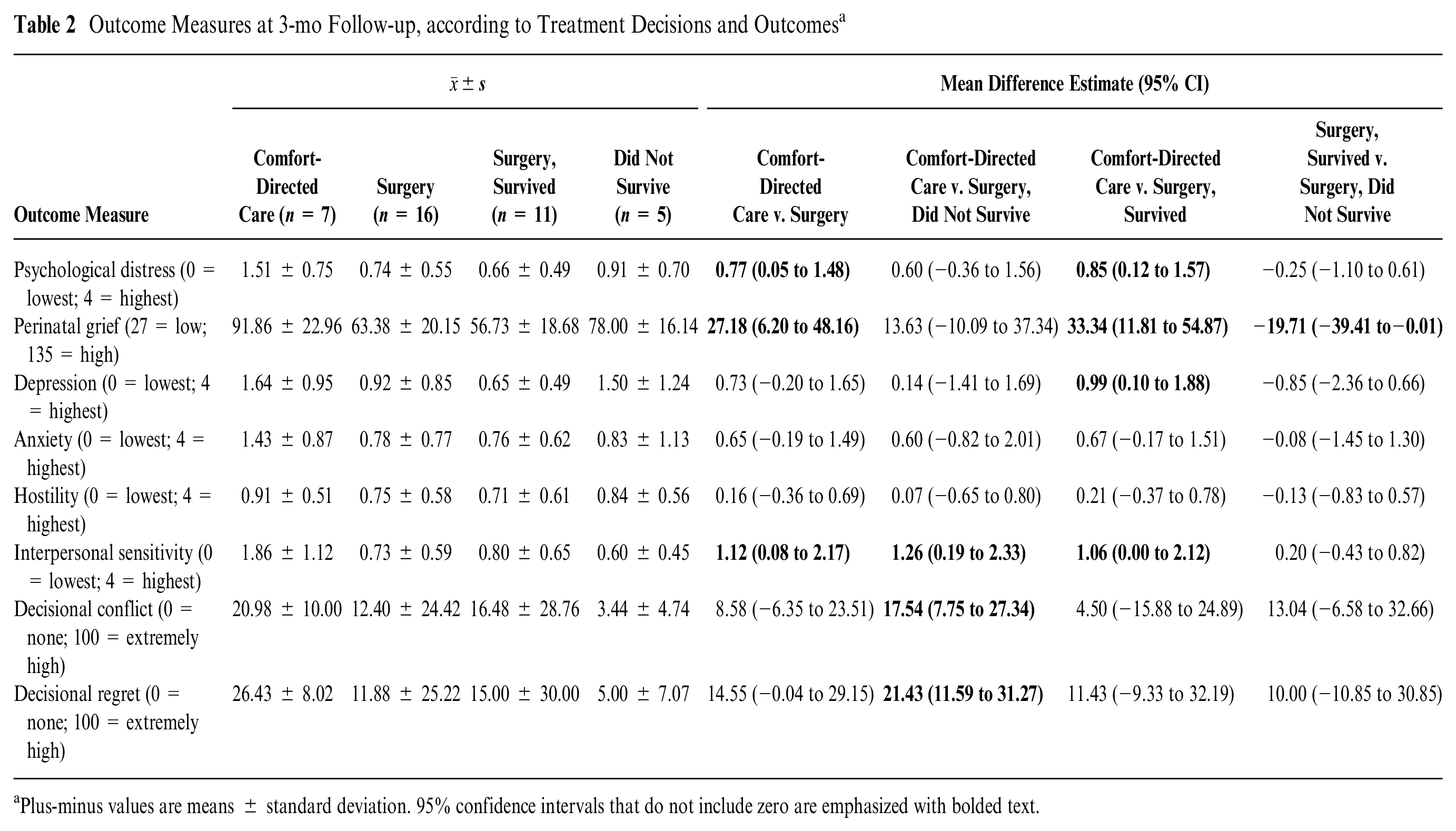
Plus-minus values are means ± standard deviation. 95% confidence intervals that do not include zero are emphasized with bolded text.
Comfort-Directed Care (n = 7) versus Surgery (Did Not Survive) (n = 5)
As shown in Figure 2 and Table 2, parents who decided on comfort-directed care reported higher interpersonal sensitivity compared with parents whose child did not survive following surgery (mean difference estimate = 1.26; 95% CI, 0.19–2.33) and higher decisional conflict (difference = 17.54; 95% CI, 7.75–27.34) and regret (difference = 21.43; 95% CI, 11.59–31.27). Confidence intervals for the differences in reported psychological distress (difference = 0.60; 95% CI, −0.36 to 1.56), perinatal grief (difference = 13.63; 95% CI, −10.09 to 37.34), anxiety (difference = 0.60; 95% CI, −0.82 to 2.01), depression (difference = 0.14; 95% CI, −1.41 to 1.69), and hostility (difference = 0.07; 95% CI, −0.65 to 0.80) between parents who decided on comfort-directed care and those whose child did not survive following surgery were consistent with no effect.
Comfort-Directed Care (n = 7) versus Surgery (Survived) (n = 11)
Parents who decided on comfort-directed care reported higher levels of psychological distress (mean difference estimate = 0.85; 95% CI, 0.12–1.57), perinatal grief (difference = 33.34; 95% CI, 11.81–54.87), depression (difference = 0.99; 95% CI, 0.10–1.88), and interpersonal sensitivity (difference = 1.06; 95% CI, 0.00–2.12) compared with parents who decided on surgery and their child survived (Figure 2 and Table 2). The CIs for the differences in reported levels of anxiety (difference = 0.67; 95% CI, −0.17 to 1.51), hostility (difference = 0.21; 95% CI, −0.37 to 0.78), decisional conflict (difference = 4.50; 95% CI, −15.88 to 24.89), and decisional regret (difference = 11.43; 95% CI, −9.33 to 32.19) between parents who decided on comfort-directed care and those who decided on surgery and their child survived included no effect.
Surgery (Survived) (n = 11) versus Surgery (Did Not Survive) (n = 50
Parents whose child had survived following surgery reported lower levels of perinatal grief (mean difference estimate = −19.71; 95% CI, −39.41 to −0.01) compared with parents whose child had not (Figure 2 and Table 2). The CIs for differences in reported psychological distress (difference = −0.25; 95% CI, −1.10 to 0.61), depression (difference = −0.85; 95% CI, −2.36 to 0.66), anxiety (difference = −0.08; 95% CI, −1.45 to 1.30), hostility (difference = −0.13; 95% CI, −0.83 to 0.57), interpersonal sensitivity (difference = 0.20; 95% CI, −0.43 to 0.82), decisional conflict (difference = 13.04; 95% CI, −6.58 to 32.66), and decisional regret (difference = 10.00; 95% CI, −10.85 to 30.85) were consistent with no effect.
Additional Analyses
We also examined the 5 subscales within the decisional conflict scale: feeling informed, clarity of values, support from others, choice uncertainty, and effective decision making to determine how the treatment decision affected each. 22 These analyses suggest that parents who decided on comfort-directed care reported greater uncertainty about their decision as compared with parents who decided on surgery, regardless of the child’s survival outcome (Supplementary Table 1). In addition, parents who decided on comfort-directed care reported greater disagreement on the effective decision subscale (e.g., greater dissatisfaction with their decision) as compared with those whose child did not survive following surgery. There were no other differences between groups on any other subscales.
While there may be significant differences between groups, it is also important to examine whether there were clinically meaningful outcomes. These were defined as scores ≥1.59 for males and 1.39 for females for psychological distress, 26 perinatal grief scores >91, 34 decisional conflict scores >25, 28 and decisional regret scores ≥25. 29 Aligned with the previous pattern of results, we found that a greater proportion of parents who decided on comfort-directed care reported clinically meaningful levels of psychological distress (57% v. 20%), perinatal grief (57% v. 20%), decisional conflict (43% v. 12%), and decisional regret (71% v. 19%) as compared with those who opted for surgery, regardless of outcome. The number and percentage of parents who reported clinically meaningful scores for each scale is reported in the Supplement (Table 2).
Discussion
Prior research has shown that parents of children diagnosed with complex CHD often experience significant negative psychological outcomes, which can have a substantial impact on their well-being and health.2,6–17 The aim of this exploratory study was to contribute to better understanding of how parents’ psychological and decision-making outcomes differ as a function of their treatment decision and the survival outcome of their child.
We found that parents who decided on comfort-directed care reported the highest levels of overall psychological distress, grief, depression, and interpersonal sensitivity. No differences were observed between parents on reported anxiety or hostility regardless of their treatment decision or outcome. While high levels of psychological distress and other negative psychological outcomes have been documented across parents of children diagnosed with complex CHD regardless of treatment choice,2,6–17 these findings suggest that those who decide on comfort-directed care may be at an especially increased risk of psychological distress and grief. Prior work has found comfort-directed care to be associated with low parental self-efficacy (i.e., feeling a lack of control) 35 and misconceptions that they and the medical team “gave up” on their child,36,37 which could be important drivers of the heightened psychological distress and grief experienced by these parents. We also found that parents whose child had not survived following surgery reported higher distress than those whose child survived, which corroborates prior research showing that bereaved parents are at higher risk of psychological distress. 38 Qualitative studies that are able to further explore these differences in negative emotions experienced by parents based on their treatment decision are needed to help inform efforts to provide better counseling to families.
Parents in our study who decided on comfort-directed care reported higher decisional conflict and regret than parents who decided on surgery. Supplemental analyses of the decisional conflict subscales suggest that the difference in reported decisional conflict was largely driven by higher decisional uncertainty about their treatment choice (i.e., feeling unsure about what to choose) among parents who decided on comfort-directed care (Supplementary Table 1), which was particularly clear when comparing parents who decided on comfort-directed care with parents whose child did not survive following surgery. One explanation for the lower conflict and regret scores among parents whose child did not survive following surgery could be that the emotional impact of this event may have motivated parents to reflect more positively on their decision as one that they had to make.
Of the 7 parents who decided on comfort-directed care, 3 (43%) reported clinically meaningful decisional conflict scores (>25), and 5 [71%] reported clinically meaningful decisional regret scores (≥25). In contrast, scores were clinically meaningful for only 2 (18%) of the 11 parents whose child survived following surgery for decisional conflict and 3 (27%) for decisional regret. Among parents whose child did not survive following surgery, none reported clinically meaningful levels of decisional conflict or regret. Thus, these findings are suggestive of clinically meaningful differences between parents who decided on comfort-directed care and those who decided on surgery.
The higher levels of decisional conflict and regret in parents who decided on comfort-directed care are a concerning signal as they can lead to substantial deterioration of health and well-being.24,39 We did also note that one parent whose child survived following surgery reported extremely high levels of both decisional conflict and regret. Exploring whether these parents would benefit from receiving tailored decisional support 40 or coaching, 41 which have shown positive results in reducing parental conflict and regret across other domains, therefore represents an important area for future work.
Qualitative studies suggest that over time, parents of children who survive following surgery may experience a positive emotional transition from grief to relief. 42 In prior work, the impact of psychological outcomes has been shown to persist for more than 1 y and to vary during that time.10,13,14 Given the limited follow-up and cross-sectional nature of our study, we cannot conclude whether the observed findings persist or vary over time. To this end, further studies with a longer follow-up time would be beneficial. In addition, it is also worth noting that the wording introducing the decisional conflict items asked parents to “think about the decision you are about to make,” even though the survey was given 3 mo after parents had made their treatment decision. While this could have potentially resulted in some confusion in how to respond, no such concerns were raised by parents, and we do not expect this wording to have notably influenced their responses.
It is also possible that parental expectations regarding the likelihood of the surgery being successful could have influenced their reactions to the outcome of the surgical intervention, this but was not assessed in this study. Parents often experience greater distress and grief when they perceive the death to have been unexpected. 43 Therefore, overly optimistic parental expectations might exacerbate negative psychological outcomes associated with the death of a child following surgery. 44 It is also possible that the low levels of decisional conflict and regret reported by parents whose child did not survive surgery may reflect greater concordance between their expectations of the treatment and the outcome. Further studies are needed to better understand how parental expectations might interact with the surgical outcome for their child’s complex CHD and influence parental psychological and decision-making outcomes. In addition, research should explore methods for informing parents about the uncertainty associated with treatment outcomes and strategies to help parents manage this uncertainty, 45 which may be particularly helpful for reducing decisional conflict and regret.
Taken together, the findings from this exploratory study suggest that there may be important differences in parents’ psychological outcomes following a diagnosis of complex CHD for their child that appear to hinge both on their treatment approach and the treatment outcome (for surgical intervention). Further research is needed to replicate these findings to determine whether it may be suitable for tailoring psychological support to parents based on these factors
The present findings should be viewed in light of certain limitations. As the study was conducted at a single site, findings could be specific to the unique contexts of the health care center and region. Multisite studies would provide valuable data on whether these findings are replicable and may yield further insights on potential center and geographic factors that influence parental distress and decision-making outcomes.
Given the small sample sizes, we did not have sufficient power to make strong statistical inferences or adjust for possible confounders (e.g., nonindependence of parent pairs). Thus, confirmatory studies with preregistered hypotheses and analytical strategies are needed to confirm the reliability and validity of the present findings. There was also underrepresentation in several potentially important domains that may limit generalizability. For example, as almost all parents were married, the findings do not extend to single parents who are likely to encounter additional barriers and challenges and have different experiences to those captured in this study.46,47 Furthermore, although the study was inclusive to all parents, most parents in our study were women; thus, the experiences of other parents may not be represented in our findings. 48
It is also important to note that we had difficulties recruiting (46% enrollment rate) and retaining (34% lost-to-follow up) study participants. This is a particularly distressful time for parents, and for some contexts (e.g., postnatal diagnosis and termination), there is a very short time frame to effectively recruit parents before a decision is made. In addition, the COVID-19 pandemic has significantly affected normal clinic flow in hospitals and other health facilities as well as the ability to recruit participants for studies. This caused significant delay in recruitment, particularly over the winter months when COVID-19 cases were very high.
Postnatal diagnoses are becoming less common nationally, 49 and ∼80% of cases requiring neonatal surgery are diagnosed prenatally at this institution. As only 1 parent in our study received a postnatal diagnosis and was not included in the analyses, our findings cannot speak to the experiences of parents diagnosed postnatally or of those who decide on termination as no parents in our sample pursued this option. Thus, continued efforts and larger multisite studies are required to identify and better understand the unique needs of these parent populations not captured in the present study in order to provide effective support.
In conclusion, while parents who received a prenatal diagnosis of complex CHD experience distress, the findings from this exploratory study illuminate potentially important differences in parents’ levels of psychological distress and negative emotions regarding their decision-making outcomes, which seem to vary based on their treatment approach (comfort-directed care v. surgical intervention) and, in the case of surgical intervention, the treatment outcome (i.e., whether or not the child survives). Most notably, in the present exploratory study, parents who decided on comfort-directed care experienced higher levels of psychological distress, whereas parents who decided on surgery experienced greater decisional regret and conflict, particularly when the child did not survive surgery. We believe that it is crucial for additional and larger multisite studies to replicate this exploratory work to assess the validity and reliability of these findings. This confirmatory evidence is necessary to inform the development and testing of support strategies and decision aids tailored to parents’ treatment choice and the child’s survival outcome to provide better support for all parents during this difficult and challenging period.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683231204551 – Supplemental material for Parents’ Psychological and Decision-Making Outcomes following Prenatal Diagnosis with Complex Congenital Heart Defect: An Exploratory Study
Supplemental material, sj-docx-1-mpp-10.1177_23814683231204551 for Parents’ Psychological and Decision-Making Outcomes following Prenatal Diagnosis with Complex Congenital Heart Defect: An Exploratory Study by Alistair Thorpe, Rebecca K. Delaney, Nelangi M. Pinto, Elissa M. Ozanne, Mandy L. Pershing, Lisa M. Hansen, Linda M. Lambert and Angela Fagerlin in MDM Policy & Practice
Footnotes
Acknowledgements
We are very grateful to the parents who completed this study during a very difficult time in their lives. We would also like to thank our parent collaborators Ms. Natalia Anderson, Mr. Johnny Anderson, and Ms. Tammy Shepherd. We are also grateful to Karina Pritchett, BA (Spencer Fox Eccles School of Medicine at University of Utah, Salt Lake City, UT) for her assistance with the design of the graphical abstract. Karina was not compensated for this work beyond her typical employment compensation.
Author Contributions
Dr. Thorpe substantially contributed to the conception and design, data analysis and interpretation, and the drafting and revising of the manuscript. Dr. Delaney substantially contributed to the conception and design, acquisition and interpretation of data, and revised the manuscript for critically important content. Dr. Pinto and Ms. Pershing substantially contributed to the conception and design, acquisition of data, and revised the manuscript for critically important content. Ms. Hansen and Ms. Lambert substantially contributed to the acquisition of data, and critically revised the manuscript. Dr. Ozanne substantially contributed to the conception and design and critically revised the manuscript. Dr. Fagerlin substantially contributed to the conception and design, acquisition of data, acquisition of funding for the study, and critically revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Clinical Trial Registration NCT04437069
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: American Heart Association’s Strategically Focused Research Network – Children’s grant (17SFRN33660465) to Dr. Fagerlin. Dr. Thorpe was supported by grant No. 51300302 from the American Heart Association Children’s Strategically Focused Research Network fellowship awarded to Dr. Fagerlin. Dr. Delaney’s effort was supported by the National Institutes of Health under Ruth L. Kirschstein National Research Service Award T32HL007576 from the National Heart, Lung, and Blood Institute. The American Heart Association had no role in the design or conduct of the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.