
Abstract
Highlights
The modeling framework is a starting point for assessing the health and cost impacts of antibiotic resistance on surgeries in England.
Formulating a framework and synthesizing evidence to parameterize data gaps provides targets for future research.
Once data gaps are addressed, this modeling framework can be used to feed into overall estimates of the health and cost burden of antibiotic resistance and evaluate control policies.
Antimicrobial resistance (AMR), the ability of microbes to survive treatment with antimicrobial agents, is recognized as one of the top 10 global public health threats by the World Health Organization. 1 With an estimated 4.95 million global deaths associated with bacterial AMR alone in 2019, AMR poses a large health burden and we may benefit from policies to mitigate the emergence and spread of resistant organisms. 2 Worldwide, it is estimated that up to 100 trillion USD of economic output could be lost by 2050 if AMR continues to rise. 3 To address these challenges, the UK government has set aims around reducing both resistant infections and antibiotic use.4,5
Antibiotic resistance (ABR) is a subset of AMR: the resistance of bacteria to antibiotics. Antibiotic-resistant bacteria can be found in multiple environments and continue to evolve. 6 In the context of surgery, antibiotics are used preventatively (prophylaxis) or as treatments for patients who develop bacterial infections. One of the direct effects of ABR is the difficulty in treating infections caused by resistant bacteria. Indirectly, the emergence of ABR threatens the viability of medical and surgical interventions that have a high risk of infectious complications in the absence of effective prophylaxis. These challenges are exacerbated by the stagnation in the discovery of new antibiotics in recent decades, leading to fewer treatment options to manage antibiotic-resistant infections, 7 as well as other complications due to ABR being infectious and thus having onward consequences for other patients, hospitals, and populations.
Surgical site infections (SSIs) are postoperative infections caused by the presence of bacteria in the surgical site during or after invasive surgeries. 8 While the risk and severity of an SSI are influenced by a variety of factors,9,10 ABR acts through 2 mechanisms:
it reduces the effectiveness of prophylactic antibiotics, increasing the occurrence of SSIs
it reduces the effectiveness of empirical and targeted antibiotics, leading to unresolved and more serious SSIs9,10 and thus worse health outcomes.
Ultimately, rising ABR may lead to restrictions in current routine surgical procedures. 11 SSIs that are adequately treated with antibiotics alone today may need adjunctive invasive treatment if caused by resistant bacteria in the future. Other infections may be refractory to treatment, causing long-term morbidity or death from sepsis. 12
Despite the potential costs of ABR on surgical procedures, the cost and health impacts of this are, to date, largely unknown. There is a lack of empirical data to suitably estimate the magnitude of these impacts and a lack of studies that have collected relevant outcomes. 13 To develop appropriate policies to efficiently tackle the threat of ABR on surgical procedures, the potential costs and health impacts need to be better understood.
The main objective is to produce an economic modeling framework that could be used to enable the estimation of the cost and health burden of ABR on surgical procedures through the 2 mechanisms explained above. We demonstrate the utility of this framework on specific surgical procedures as a proof of concept. The framework focuses on the average impact at a cohort level from a National Health Service (NHS) perspective. Any onward consequences from increased resistance, changes in transmission risks, and subsequent population effects are not captured within the framework. However, exploring the simplified impact is a key prerequisite for further research on the wider impact of ABR and the evaluation of policies targeted to reduce ABR infections. While the framework can be used to provide quantitative estimates of the impact of ABR, the numerical outputs have an illustrative purpose only, with the focus being on the framework itself.
Methods
We constructed an economic modeling framework to assess the aggregate impact of increasing ABR rates on surgical procedures for a simulated cohort. We developed a model structure that could address the following: 1) the implications of ABR on the effectiveness of both prophylaxis (to avoid SSIs) and treatment of SSIs when they occur and 2) the likely short- and long-term implications of ABR for health and cost outcomes for a wide range of surgeries.
The development of the framework had 3 key components:
In consultation with experts on ABR and SSIs, we developed a conceptual map to quantify the impact of rising ABR on surgical procedures (see Supplementary Material A).
By using the available empirical evidence identified while developing the conceptual map and assessing the quality and applicability of these data, we developed a model structure reflecting the prophylactic and infection treatment care pathway, making simplifying assumptions where necessary (Figure 1).
We applied the final framework to 2 case studies (emergency fractured neck of femur procedure and elective colorectal resection due to cancer), which formed the development of 2 economic models. The procedures were chosen after conducting a targeted literature review and a discussion with experts on ABR and SSIs to identify 2 surgical procedures where increasing rates of ABR could have a large detrimental impact on population health and NHS costs. However, the framework was developed for it to be applied to any procedure providing data are available. We developed a formal approach to elicit judgments from clinical experts to support the estimation of model parameters for which available evidence was absent, sparse, or of limited relevance to the context of interest.

Conceptual framework structure. SSI, surgical site infection. *Thirty-day postoperative mortality. **Surgical site infection treated with antibiotics alone or a salvage procedure with antibiotics. ***Length of time horizon varies with case study (15-y emergency repair of neck of femur and 30-y for elective colorectal resection). One-year cycle length. Dotted line = the split between the decision tree and the Markov structure. SSIs include both deep and superficial infections. People can die immediately after the procedure from postoperative mortality and, following that, as a consequence of SSI or background mortality if no SSI.
Developing the Modeling Framework
Treatment Pathway
The modeling framework was based on the treatment pathway for SSIs. Treatment is dependent on whether the infection is superficial (at the incision) or deep (below the incision; see Supplementary Material B for full definitions):
If a superficial infection is suspected, or if a deep infection is misidentified as a superficial infection, patients are treated with antibiotics and drainage alone. Patients then require 1 or more salvage procedures (defined as surgical procedures to cut away infection) if the antibiotics do not work or if a deep infection is suspected.
If a deep infection is suspected patients are simultaneously treated with antibiotics and 1 or more salvage procedures.
If the antibiotic treatment and/or salvage procedure do not resolve the SSI, then the patient eventually exhausts pharmacologic and surgical treatment options and would have a chronic infection and/or die.
Model Structure
The modeling framework (Figure 1) consists of 2 parts:
An initial 90-d decision tree (left side of Figure 1), which determines the number of individuals who have no SSI, a resolved SSI (with no salvage procedure), a resolved SSI (with a salvage procedure), or a chronic infection. This starts with an index procedure, from which patients who survive the procedure either contract an SSI or do not. The SSI rate is partly influenced by the prophylactic antibiotic efficacy.
This is followed by a Markov model (right side of Figure 1), capturing the lifetime consequences based on outcomes at 90 d (no SSI or with resolved/unresolved SSI).
People who are alive after the 90-d decision tree move into the Markov model. The Markov model captures 5 health states that are associated with different clinical management following the index surgery, long-term morbidity, and potential mortality:
(1) Patients who do not contract an SSI following the index surgery are assumed to be alive without SSI-related complications for the remainder of their lifetime.
People who do contract an SSI either have a resolved or unresolved infection after the 90 d following the index surgery. Infections may be resolved either from antibiotics alone (2) or after a salvage procedure (3). Different health-related quality of life (HRQoL) scores are applied depending on how the infection is resolved (salvage procedures may have lasting effects that are associated with long-term HRQoL decrements). (4) If unresolved, a person is assumed to be chronically infected for the remaining duration of life.
(5) Finally, all people in all health states face a risk of death in the model.
The model simultaneously captures the implications of ABR by allowing for higher rates of SSIs as the effectiveness of antibiotic prophylaxis wanes and by allowing for worsened outcomes following SSIs to reflect reduced antibiotic treatment effectiveness.
A multidisciplinary steering group chosen on the basis of their expertise in the topic of ABR and/or surgery (clinicians, microbiologists, hospital pharmacists, mathematical modelers, epidemiologists, and health economists, among others) validated both stages of the economic model. The focus of the validation was to ensure that the impact of rising ABR rates would be captured in the model structure, especially under worst-case scenario conditions.
Use of Structured Expert Elicitation
To model ABR, we need to predict both how ABR rates may change in the future and how this might influence the effectiveness of antibiotic prophylaxis and treatment. However, there is a lack of empirical evidence to inform these, complicated further by multiple treatment lines and heterogeneity in antibiotics used. To address these uncertainties, we developed a formal approach to elicit judgments from clinical experts on the implications of ABR for SSI risk and SSI outcomes.
To inform model parameters included in the framework, we elicited expert opinions using a structured process to reduce the potential for bias. 14 We also captured the uncertainty associated with the estimated values to parameterize the uncertainty within the economic model. As the elicited estimates related to clinical practice and treatment outcomes, we targeted orthopedic and colorectal consultants and surgeons for this exercise.
Clinical experts were asked for their estimates of:
current and future (in 10 y) SSI rates resulting from prophylactic antibiotic failure, and
current and future (in 10 y) 90-d outcomes resulting from SSIs (mortality, chronic infection rates, and the use or not of salvage surgeries), and
how i) and ii) might change due to rising levels of ABR.
These estimates were provided assuming all else remained equal (e.g., no new antibiotics, procedures, or protocols). The elicitation is not designed to be a forecast or a prediction but a hypothetical scenario of what could happen in approximately 10 y absent any change in practice. Further details of the methods of the elicitation process can be found in Supplementary Material C.
Equivalent Loss in Health Care Expenditure
To measure the impact of ABR, we developed the concept of the equivalent loss in health care expenditure (ELHE). The ELHE is a variation of the net monetary benefit concept 15 and estimates both health care costs or savings and the monetary equivalent of net health lost or gained based on an assumed opportunity cost of £20,000 per quality-adjusted life-year (QALY; representing the opportunity cost to the NHS) plus any additional costs. 16
We considered the ELHE to be more appropriate than the net monetary benefit or loss, as we are estimating the loss in expenditure that would be equivalent to both the loss in health and the increase in costs to the NHS. This means that, all else being equal, the decision maker would be willing to pay up to the ELHE for intervention(s), or policies, that can avoid this scenario. Different policies or interventions were not being compared in this analysis, and so incremental cost-effectiveness ratios were not calculated.
In a real-world context, the ELHE would indicate the estimated limit the NHS could spend on an intervention aimed at reducing the risk of ABR, based on a £20,000 per QALY opportunity cost. See Supplementary Material D for a worked example.
Applying the Modeling Framework
We applied the modeling framework to 2 surgical case study examples. These were emergency repair of neck of femur surgery (neck of femur) and elective colorectal resection surgery due to cancer, representing distinct populations and surgery types (old v. young, emergency v. elective surgeries). The procedures were selected based on a targeted review of the literature and clinical opinion from the Steering Group, who thought that increasing ABR in these 2 procedures would have a particularly detrimental impact on population health and NHS costs. For simplicity, only the neck of femur case study is presented here to provide an example of applying the framework itself. See the Supplementary Material for further details on colorectal resection case study.
The model takes the perspective of the English NHS and includes a hypothetical cohort with a starting age of 84 y, representing the average age of a person undergoing a neck of femur procedure. 17 Short-term outcomes (contracting an SSI, antibiotic treatment, salvage procedures, SSI-related mortality) are assumed to occur within 90 d (decision tree component). A lifetime horizon of 15 y is applied because this is assumed to be the maximum life expectancy for this population. The cycle length of the Markov model is 1 y, deemed sufficient due to people staying in the same health state until death. We apply discount rates of 3.5% and 1.5% to costs and QALYs, respectively, to align with the Green Book recommendations (typically used in public health models). 18
Evidence Used to Inform the Model
The structured elicitation process was used to derive the SSI rates and 90-d outcomes. These were compared with the estimated outcomes of SSIs (caused by ABR) currently (Table 1).
Expert Elicitation Outputs (Mean with 80% Credible Interval Where Available)
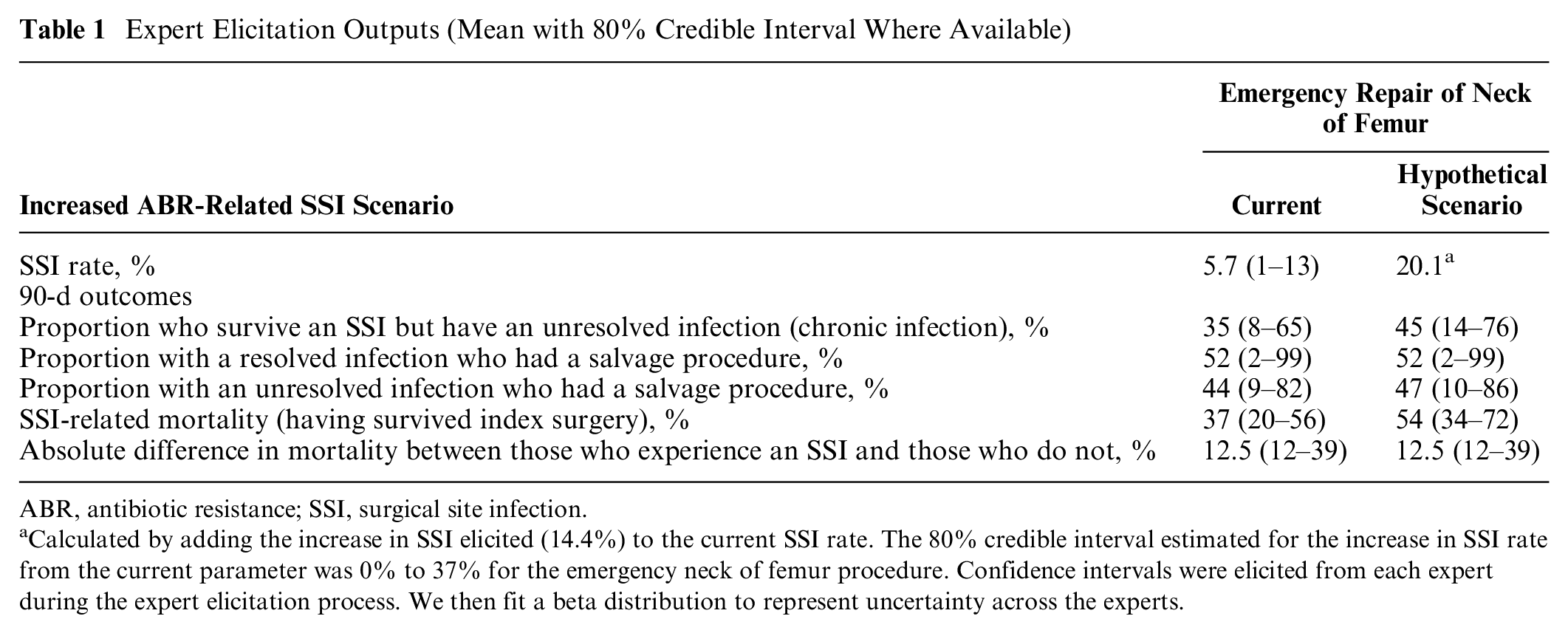
ABR, antibiotic resistance; SSI, surgical site infection.
Calculated by adding the increase in SSI elicited (14.4%) to the current SSI rate. The 80% credible interval estimated for the increase in SSI rate from the current parameter was 0% to 37% for the emergency neck of femur procedure. Confidence intervals were elicited from each expert during the expert elicitation process. We then fit a beta distribution to represent uncertainty across the experts.
We conducted a targeted review of the literature for costs and resource use, effectiveness data, mortality, and HRQoL values. See Table 2 for details on the key inputs used, with further details in Supplementary Material E and F.
Other Key Case Study Inputs for Emergency Repair of Neck of Femur a

SSI, surgical site infection
The cost of hospital stay was not applied to length of stay, as this is expected to be captured in the cost of an SSI applied in the model. Length of stay is included only to calculate differences in hospital stay as a consequence of different health outcomes following surgery.
A Girdlestone procedure was the salvage procedure used in the neck of femur case study.
Main Model Outcomes
The main model outcomes are incremental costs, incremental QALYs, and ELHE.
We used the £20,000 threshold instead of the £60,000 per QALY threshold seen in the Green Book (often used in public health models) as all the costs and benefits measured in the model accrue in the health system and not widely across other sectors.
Description of Sensitivity Analysis
Univariate and Probabilistic Sensitivity Analysis:
We conducted univariate deterministic sensitivity analysis in the form of a tornado plot. The parameters of the expert elicitation outputs were varied between the upper and lower values of the 80% credible intervals from the expert elicitation process (see Supplementary Material G and Table 1), with a cap introduced to avoid increased ABR scenarios resulting in counterintuitive outcomes (e.g., increased ABR leading to lower chronic infection rates or lower mortality). Where upper and lower parameter values could not be sourced, they were assumed to be ±25% of the base case.
A probabilistic sensitivity analysis was also conducted in which the model was run for 1,000 iterations to calculate average estimates. All inputs for the probabilistic sensitivity analysis and deterministic sensitivity analysis can be found in Supplementary Material H.
Further Sensitivity Analyses
We ran 2 further sensitivity analyses. In the first analysis, the inputs derived from the expert elicitation were changed to the lower or upper values of the 80% credible intervals (CIs) to represent optimistic (all lower CIs) and pessimistic (all higher CIs) scenarios. The CIs were used for the following current and hypothetical 10-y scenario parameters: the increase in SSI rate (10-y parameter only), chronic infection rates, and mortality (see Table 1 for the CIs). Furthermore, the inputs representing the current SSI rates caused by ABR were altered to reflect the SSI rates reported in the Public Health England (now UKHSA) SSI report (1%). 27
Another sensitivity analysis using 3.5% discount rates for both costs and QALYs was also conducted.
Funding
Financial support for this study was provided entirely by Public Health England Funding from both the Health Economics Commissioning Framework, for undertaking the analysis, and the Statistics, Modelling and Economics Department for publication of this manuscript.
Case Study Results
Summary
The full results are presented in Supplementary Material I for both case studies. For the emergency repair of neck of femur procedure, using the scenario inputs presented in Table 1, total QALYs could decrease by 11% (reduction of 0.34 QALYs), and total costs could increase by 39% (from £11,000 to £15,000), per patient, over their remaining lifetime (assumed to be 15 y). These results come with high levels of uncertainty. The 95% CI for the incremental QALYs is −62% to −0.4%, and the 95% CI for the incremental costs is −2% to 108%. The −2% lower bound is explained by the population being elderly, saving costs due to an increase in SSI-related mortality (and so fewer have the chance to go on to have a chronic infection).
The reduction in QALYs reflects a higher proportion of people acquiring an SSI, with subsequent chronic infections or salvage procedures reducing long-term quality of life. The cost increases are also driven by a higher proportion of chronic infections along with the increase in SSI rate.
The monetary impact to the NHS of these projected changes could be an ELHE per person of £11,000 (CI £250 to £42,000). This represents the maximum the NHS could usefully spend on a new intervention per patient to reduce the risk of ABR. These losses are driven evenly by health losses and additional costs.
Univariate Sensitivity Analysis
The results of the univariate sensitivity analysis show that the SSI rate increase caused by ABR, the cohort age, the proportion of patients with a chronic infection, and the 90-d mortality risk are key drivers of the results (Figure 2). Cohort age is a key driver due to younger individuals accumulating increased costs and health losses by naturally living longer with the consequences of an SSI when compared with someone older.

Key drivers of the case study results: univariate sensitivity analysis. ABR, antibiotic resistance; SSI, surgical site infection. All mortality risks are absolute. Parameters labeled “baseline” represent the currently estimated situation. Parameters labeled “scenario” represent a future hypothetical scenario.
Further Sensitivity Analyses
The optimistic and pessimistic analyses using the upper and lower credible estimates from the expert elicitation interview (Table 1) are shown in Figure 3. The upper and lower bars represent where the base case value would move if the upper and lower credible limits, estimated via the expert elicitation process, represented the average value for SSI rate increase and 90-d outcomes.
The ELHE ranged from approximately £31,000 (pessimistic) to £600 (optimistic) per person over 15 y in the neck of femur population. The wide range in results of this scenario analysis highlight the uncertainty the experts had faced when estimating SSI rate changes and outcomes.
Discussion
Brief Synopsis of Key Findings
This research presents a novel economic modeling framework that captures the impact of ABR on surgical procedures in terms of health outcomes and economic costs. We applied the framework to 2 case studies: emergency repair of neck of femur procedures and elective colorectal resection, using evidence from the literature and experts’ opinion. These case studies provide examples of how the framework can be applied to generate insights into the potential impacts of ABR for surgical procedures and what may be observed if no new practices to combat ABR are implemented through the scenarios conducted. There is substantial uncertainty associated with the numerical outputs of the case studies, but they are able to indicate the possible magnitude of the impact of increasing ABR levels.
Through the modeling framework, it was estimated that as the SSI rate increases due to ABR (affecting the antibiotic efficacy of both prophylaxis and treatment), total costs increase while the health benefits decrease for both case studies. In a real-world context, this could generate large economic and health losses. Simple estimates for neck of femur indicate that, per 10,000 people, over the patient’s assumed remaining lifetime (15 y), a 14% increase in SSI rate may lead to an ELHE (the loss in health care expenditure as defined previously) of approximately £111 million (CI £2.6 million to £418 million). Effectively, this suggests that the NHS could spend up to £111 million in new policies to avoid the health and cost losses per 10,000 people undergoing neck of femur procedures. With more than 70,000 hip fracture procedures conducted each year across England, Wales, and Northern Ireland, 17 this could mean substantial increases in costs and health loss, although not all hip fracture procedures would relate to the neck of the femur. Similarly, for colorectal resection, per 10,000 people, over 30 y, a 12% increase in SSI rate is estimated to result in an ELHE of £134 million (CI 33 million to £299 million). These analyses highlight the large impact of increased SSI rates and the variability of impact between different surgeries.
Explanations for the Findings
The framework highlights the issues with both reduced prophylaxis and reduced treatment efficacies. In addition, it has been useful in identifying key parameter
Although effectiveness of prophylaxis is a key concern across populations, treatment effectiveness against SSIs increases in importance in populations who are likely to live longer after surgery.
Comparing Results with Published Work
This work presents the first attempt to quantify the health and economic impacts of ABR, using 2 case studies, in England. Teillant et al. 11 previously estimated the potential consequences of ABR on surgery in the United States but did not estimate the economic impacts nor study the impact of reduced antibiotic treatment effectiveness (only prophylaxis). In the study, the authors estimated that a 30% reduction in antibiotic prophylaxis efficacy could lead to more than 20,000 additional infections per year in colorectal surgery. They used scenarios of differing prophylactic antibiotic efficacy due to the absence of evidence of the correlation between ABR rates and SSIs. A benefit of the expert elicitation we conducted is that it helps fill these data gaps.
Key Considerations of the Study
The implication of ABR is captured in the framework by allowing for higher SSI rates and worsened outcomes following SSI. Wider consequences, such as altered clinical management (with subsequent downstream impact) and spread of resistance between individuals (both in the hospital and community), are not captured in this framework. However, this framework could potentially be used to facilitate further work to explore these outcomes.
Limitations of this study included the inability to estimate ABR rates for specific pathogens and drugs and link these to clinical outcomes and the assumption that there would be no changes in clinical practice. Evidence gaps were also apparent. These are described below.
Estimating ABR rates for specific pathogens and drugs
We could not estimate the impact of individual pathogen resistance to a specific antibiotic. If increases in pathogen resistance could be modeled, by considering surgery-specific pathogens and pathogen-specific resistance rates, this would allow a more accurate estimation of current ABR and potentially ABR trends over time. However, this remains a challenging exercise due to geographical variation in pathogen resistance rates across England and the associated variation in choice of antibiotic prophylaxis and treatment across England. It is also difficult to find an appropriate method to link the direct effect of ABR on SSI rates and outcomes.
No changes in clinical practice
We assumed that there would be no changes in clinical practice as ABR increased, which could lead to an overestimation of the impact of ABR on surgeries. This was done to enable us to model the causal impact of ABR on surgical procedures. However, this may not be the case, with decision varying by surgical area.
Clinical opinion deemed that emergency repair of neck of femur procedures would go ahead regardless of a rise in ABR, primarily due to the high mortality risk in this population if left untreated. For colorectal resection, one clinical expert outlined potentially changing practices. Reduction in antibiotic efficacy could lead to alternatives being used so that surgery can proceed, such as using irrigation devices (as in orthopedic surgery) to wash out pathogens in a colorectal setting 28 or using bacteriophages.29,30 Alternatively, ABR may lead to certain procedures being forgone to avoid the development of SSIs and potentially untreatable infections.
A recent study by Naylor et al. 31 highlighted how existing data on AMR’s health impacts in England could be combined with expert elicitation to explore how AMR could affect treatment pathways for individuals requiring surgery. The modeling framework developed here is intended to be a building block to support future evaluations of the cost-effectiveness of alternative policies to reduce the impact of ABR on surgeries. It could also support research in estimating the point at which forgoing surgery may be considered, by estimating the health and cost impact of 2 different pathways, capturing the continuation of standard practice with the given SSI rate compared with the consequences of providing nonsurgical management.
Evidence gaps
A 2019 literature review of studies evaluating the economic burden of SSIs due to AMR, conducted across countries, highlighted various methodological gaps. 32 These include gaps in epidemiological data, inconsistency in SSI definitions and differences in SSI surveillance across locations. Overall, the authors recommended choosing appropriate methodologies for both surveillance and quantifying the burden of SSI. We came across similar issues when designing and conducting our study. As this is a modeling framework, there is scope for further development should data to inform the evidence gaps become available. The main evidence gaps are described below.
Empirical and targeted treatment success rates could not be accurately estimated due to evidence gaps in pathogen-antibiotic combination data separated by line of treatment and data linking the line-specific effectiveness to patient outcomes. To overcome this, we evaluated an overall 90-d success rate of SSI treatment (combining both empirical and targeted treatment). This single value embodied the range of ways in which patients could be treated (including single or multiple lines of antibiotics, with or without salvage procedures). However, the 90-d outcomes were largely informed by the expert elicitation. The elicitation results highlighted the large uncertainty clinical experts have with regard to quantifying the impact of ABR on surgical procedures and how these may change over time (as shown in Table 1 and Figure 3).
Data on long-term chronic infection outcomes were literature based and limited to costs and morbidity impacts, since evidence on mortality was not identified. Where costs could be sourced, these were not always procedure specific (e.g., for chronic infection; Table 2).

Further sensitivity analysis—equivalent loss in health care expenditure (ELHE): optimistic and pessimistic analysis.
Future research directions
Estimating the health and economic implications of ABR on surgical procedures is complex and largely underexplored. However, the patient costs and benefits are important to consider given the consequences if left unaddressed and could be an informative tool for clinicians, hospital managers, and policy makers (among many other stakeholders). In the future, it would be important to investigate the implications of wider effects of increasing ABR at the individual level, such as increased spread of infections in the hospital and community. This framework could be a useful tool in supporting further research that could help inform decision making to address ABR.
The robustness of the evidence base could be improved by designing long-term studies for those undergoing salvage procedures due to SSI and those who are untreatable (remain with chronic infection). This would allow a more accurate mapping of the full care pathway and would enable more granular estimates of the cost and consequences of ABR.
Conclusion
With improved data, the modeling framework could be applied to further case studies. This could help inform clinicians about the potential consequences of increasing ABR if no measures are put in place. Future modeling work could integrate emerging evidence into the framework and explore how estimates of the link between ABR and SSI burden can be incorporated into the overall estimates of ABR burden. As it stands, this framework can be used as a key starting point to evaluate interventions that reduce the threat of ABR for surgeries.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683231152885 – Supplemental material for Developing a Modeling Framework for Quantifying the Health and Cost Implications of Antibiotic Resistance for Surgical Procedures
Supplemental material, sj-docx-1-mpp-10.1177_23814683231152885 for Developing a Modeling Framework for Quantifying the Health and Cost Implications of Antibiotic Resistance for Surgical Procedures by Heather Davies, Joel Russell, Angel Varghese, Hayden Holmes, Marta O. Soares, B. Woods, Ruth Puig-Peiro, Stephanie Evans, Rory Tierney, Stuart Mealing, Mark Sculpher and Julie V. Robotham in MDM Policy & Practice
Footnotes
Acknowledgements
We thank the following people who provided valuable input into the piece of work: Abtin Alvand, Nuffield Orthopaedic Centre, Oxford University Hospitals; Annalisa Belloni, World Health Organization and formally Public Health England (at the time the work was conducted); Antony Palmer, Nuffield Orthopaedic Centre, Oxford University Hospitals; Brian Ferguson, National Institute for Health Research; Charalambos P. Charalambous, Blackpool Teaching Hospitals NHS Foundation Trust and School of Medicine, University of Central Lancashire; David Dodwell, University of Oxford; David Jenkins, University Hospitals of Leicester NHS Trust; Koen Pouwels, University of Oxford; Lisa Pickering, Royal Marsden NHS Foundation Trust; Louise Dunsmure, Oxford University Hospitals; Michael Fleming, Department of Health and Social Care; Neil Hawkins, University of Glasgow; Alicia Demirjian, UK Health Security Agency; Farhan Alvi, Glan Clwyd Hospital, Bodelwyddan; Mirza Baig, Western Sussex Hospitals NHS Foundation Trust; Mohammad Mobasheri, Western Sussex Hospitals NHS Trust; Pavel Akimau, Worcestershire Acute Hospitals NHS Trust; Shaun Donaghy, Office for Health Improvement and Disparities; Syed Hassan, King’s College Hospital NHS Foundation; Theresa Lamagni, UK Health Security Agency; Catherine Bowe, York Health Economics Consortium (assisted in proofreading the manuscript following the draft). Any data or other study materials will be made available upon request to Stephanie Evans at
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YHEC was commissioned by Public Health England to create the economic framework and write the manuscript. UoY was subcontracted by YHEC for assistance with this work. Beth Woods sits on the Board of Directors for YHEC. There are no further conflicts of interest. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by Public Health England Funding from both the Health Economics Commissioning Framework, for undertaking the analysis, and the Statistics, Modelling and Economics Department for publication of this manuscript. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. Almost all was conducted remotely except one meeting. Work leading up to this publication was presented at ISPOR 2020 (poster), International Health Economics Association (IHEA) 2021, European Health Economics Association (EuHEA) 2022 (oral presentation), and Spanish Health Economics Association 2022 (oral presentation).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.