
Abstract
Highlights
UNICEF and more than 200 other international organizations endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child; yet this study is one of the first to quantify the cost-effectiveness of family-based care environments serving some of the world’s most vulnerable children.
This health economic modeling analysis found that family-based environments would prevent 422 HIV infections and 298 deaths in a cohort of 1,000 orphaned and separated children over a 10-y time horizon.
Compared with street-based “self-care,” family-based care resulted in an incremental cost of $2,528 per DALY averted (95% CI: 1,798, 2,599) and $2,355 per quality-adjusted life year gained (95% CI: 1,667, 2,413) after 10 y.
Annual per-child expenditures for children living in family-based care environments in sub-Saharan Africa could potentially be increased by at least 25% and remain highly cost-effective.
Keywords
In 2015, approximately 140 million children worldwide were classified as orphans, including 52 million children living on the African continent.1,2 These include single orphans who have lost either a mother or father due to death associated with any cause, double orphans whose both biological parents are deceased, and separated children for whom at least 1 parent is completely absent from the child’s life.2–4 Of the 16.6 million children who were orphaned because of parental deaths attributable to HIV/AIDS, 90% live in sub-Saharan Africa.1,5 As 87% of the world’s lowest-income population is estimated to be living in sub-Saharan Africa by 2030, 6 it is likely that the region’s orphan population will continue to grow in the coming decade.
A key policy response to the physical and psychosocial needs of orphaned and separated children in low-income countries has been to promote family-based care above all other care environments. 7 Family-based care includes settings that allow a child to remain with an immediate family member (such as a surviving parent), extended family members, or in informal foster care. In December 2019, some 250 international organizations and global health institutions including UNICEF endorsed efforts to redirect services toward family-based care as part of the 2019 UN Resolution on the Rights of the Child. 8 Global interests in strengthening family-based care over other alternatives cite unfavorable physical and mental health outcomes among children living in non–family-based environments (e.g., orphanages, charitable institutions), including deficits and delays in physical growth and neurocognitive development.9,10
Communities that choose to prioritize and scale up family-based care for orphaned and separated children will need up-to-date information on budget demands to be able to sustain these environments with limited resources. Yet evidence on the cost-utility of family-based care environments remains sparse. Available estimates of annual per-child costs of informal family-based settings range from $100 to $660 USD. 11 In terms of alternative care environments, institutional care in sub-Saharan Africa can cost more than 8 times per child than family-based or foster care, while evidence of the societal cost of allowing children to remain on the street is almost not existent.12–14 Although these and other studies 11 indicate that family-based settings cost less per child per year than other alternatives, they solely estimate costs and do not account for the physical or mental health impacts of supporting children within a family-based setting. Providing cost information on its own without accounting for cost-effectiveness prevents decision makers from gauging whether familial care can offer a good value for money over time.
The aim of this economic analysis is to estimate, from a societal perspective, the cost utility of family-based care environments compared with street-based “self-care” for orphaned and separated children and adolescents (OSCA) in East Africa. This analysis builds on evidence from our prior work demonstrating a lower hazard of incident HIV and death among OSCA living in family-based care compared with those on the street. 15 Our hypothesis is that annual costs per child will be higher for orphans living in family-based care than for those living on the street but that family-based environments will be cost-effective for preventing HIV and death among this population in the medium term.
Methods
Study Design
We performed a model-based economic evaluation to estimate, from a societal perspective, the cost-effectiveness and cost utility of family-based care environments compared with street-based self-care for preventing HIV and death among OSCA in western Kenya. The model was developed using published data from the Orphaned and Separated Children’s Assessments Related to their (OSCAR’s) Health and Well-Being longitudinal cohort study and other published literature. The OSCAR study comprised participants from communities within 8 administrative locations in the predominantly (61.4%) rural Uasin Gishu County in Kenya16–18 and included 300 randomly selected households caring for OSCA orphaned from all causes (family-based settings) and a convenience sample of 100 street-connected children and youth in self-care on the streets. One hundred percent of the 300 family-based settings enrolled in the OSCAR cohort were located in rural or periurban districts. 19 Additional details regarding the OSCAR study and its cohort have been previously reported.15,18
Analyses and findings from this economic evaluation are reported according to the Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement. 20
Model Framework
We constructed a Markov model to simulate incident HIV infections and deaths in a designated initial cohort of 1,000 orphaned and separated children over 5-, 10-, and 15-y time horizons. The model includes 3 health states: healthy, HIV positive, and deceased. All children were assumed to start in the healthy state, and the model cycle length was 1 y. Outcomes and costs were discounted at a rate of 3% per year. 21 The mean age of children entering the model was 10.4 y to align with that of the OSCAR cohort. 15
Intervention strategies
For this analysis, we chose to compare 2 care environments for which we previously found statistically significant differences in health effectiveness outcomes. 15 We defined no availability of care, either in a family-based environment or other setting (e.g., orphanage), as the status quo in Kenya because expenditures on street connected youth in the country is close to nil and data on the cost of providing health-related or other services to these children are almost nonexistent. 22 We defined the intervention as care provided in an informal, family-based setting. The target population for family-based care was OSCA, 18 y of age and younger.
Data analysis
Model parameters are summarized in Supplementary Table 1. The probabilities of annual transitions between the 3 health states were sourced from the literature based on the incident number of HIV infections and deaths that occurred among the OSCAR cohort at the end of the study’s follow-up period. 15 Transition probabilities were normalized per 1,000 children to account for differences in the number of children in the OSCAR cohort living in family-based settings or on the street. We assumed no new HIV infections or deaths occurred during the initial year of care and, after the first year, that probability of HIV infection or death was constant at each annual time step.
Costs were estimated directly from OSCAR study data using a prospective, micro-costing approach capturing all costs of care provision. 21 For family-based care environments, cost information was collected from October 2016 through September 2019 from 225 of the 300 participating households using a modified version of the Kenyan Household Health Expenditure and Utilization Survey. 23 Surveys were administered in person at the household level by trained research personnel with experience conducting economic evaluations. Due to generally limited access to any health care or HIV screening for street-connected youth in this setting, 22 we assumed that there were no costs associated with street-connected youth.
For family-based settings, annual recurrent costs included food and clothing, utilities and grounds maintenance, education fees, and health care expenditures (Table 1). Annual capital costs were collected on aggregate, with the purchase of cell phones cited as the most common capital cost. Donations to the household were not included in the total annual cost because donated funds were assumed to have been used to pay for items already captured in a household’s expenses.
Annual per-Child Expenditures for Family-Based Care Environments Included in Costing Assessment, by Expense Category (2018 US$)

Amounts are mean annual expenditures with standard deviations in parentheses. P values reflect statistically significant differences in annual per-child expenditures between cash-transfer and non–cash-transfer households for the relevant expense category. Cost data were collected for 225 households caring for n = 1,120 orphaned and separated children and adolescents participating in the OSCAR study. Of the 225 households for which cost data were collected, 149 households did not receive government cash transfers and 76 received cash transfers. Annual per-child costs were calculated as the household’s total annual expenditures for a given cost category divided by the maximum number of children and adolescents who were meant to be cared for by the household, inclusive of both orphaned and separated children as well as biological nonorphaned children. The mean maximum number of children who were meant to be cared for by a given family-based care environment in the OSCAR study was n = 5.4. Costs were collected in Kenyan Shillings and converted to USD using the 2018 World Bank Exchange Rate (2018 was the last year cost activites were conducted). 24
We computed the mean annual cost per child living in a family-based setting by dividing the household’s total annual expenditures by the maximum number of children and adolescents who were meant to be cared for by the household, which was inclusive of both orphaned and separated children as well as biological nonorphaned children. Costs were collected in Kenyan shillings (KES) and transformed into constant 2018 US dollar (USD) using the international exchange rate. 24 Capital costs were annuitized assuming a 10-y life expectancy for all items, an annual 3% discount rate, and no maintenance costs. 21 The mean annual per-child expenditures for family-based care environments was inclusive of both rural and periurban households; per-child costs were not stratified by household location given that, in prior work, household poverty (as measured by cash transfer status of the family) did not statistically significantly differ by rural versus periurban location. 19 To estimate quality-adjusted life years (QALYs), we used health state utilities from prior interventions that aimed to prevent HIV and death among youth in lower-middle income countries.25,26 To estimate disability-adjusted life years (DALYs), the disability weight from the 2013 Global Burden of Disease Study 27 was applied to the HIV disease state in the model as in previous studies. 28 We assumed that patients in the healthy state were free of disability.
The expected number of discounted HIV infections, deaths, QALYs, and DALYs and total discounted costs for each strategy (street-based self-care and family-based care) were obtained from the model. We calculated the incremental costs and incremental effects for individuals in family-based care environments compared with street-based self-care over the 3 time horizons: 5-, 10-, and 15-y horizons. We identified the cost-effectiveness frontier and calculated the incremental cost-effectiveness ratio (ICER), defined as the incremental cost per HIV infection averted, per death averted, per QALY gained and per DALY averted to identify the more cost-effective strategy. We adopted a definition of cost-effectiveness from the WHO-CHOICE thresholds 29 (highly cost-effective, cost-effective, or not cost-effective with an ICER < 1, 1–3, or >3 times the per-capita gross domestic product [GDP]; Kenya’s per-capita GDP was $1,708 in 2018).
We explored the sensitivity of ICERs to uncertainty in key model parameters in univariate analysis by constructing a tornado diagram of ICER estimates at 10 y after entry into care. Parameter values were varied either by a fixed percentage above and below the base-case value or by reasonable parameter ranges as informed by data sources (Supplementary Table 1). Uncertainty in ICERs was expressed as 95% credible intervals (CrIs) that were generated using probabilistic, multivariate sensitivity analysis by sampling each parameter 1,000 times from their predefined probability distributions and with the 2.5 to 97.5th percentile range of all generated results.
The model was coded in R version 4.0.5 using the Markov Models for Health Economic Evaluations Modelling heemod package, 30 and additional data cleaning and figure generation were conducted in StataSE 15 (StataCorp LLC, College Station, TX).
Role of the Funding Source
This research was fully supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R01HD060478). The funders of the study had no role in the study’s design; in the collection, analysis, or interpretation of data; or in writing of the report. All authors had access to all study data, and the corresponding author had final responsibility for the decision to submit for publication.
Results
The estimated mean annual cost per child in family-based settings was $645 (95% CrI: 614, 677). Under base-case assumptions, after 10 y, family-based care environments averted 422 new HIV infections and 298 deaths that would have otherwise occurred under the status quo of street-based self-care. Incident HIV infections and deaths are high among street-connected youth during the first 5 and 10 y after entry into care due to all individuals beginning in the healthy state (Table 2). However, this effect decreases over time, because individuals who become HIV positive cannot return to the healthy state, and the model assumes no new individuals enter the respective care environments over time.
Estimated Benefits and Cost-Effectiveness of Family-Based Care Reached by 5, 10, and 15 y after Entry into Care, under Baseline Assumptions.

DALY, disability adjusted life year; QALY, quality-adjusted life year. Simulated cohort of n = 1,000. Numbers in parentheses are 95% credible intervals: the 2.5 to 97.5th percentile range of incremental cost-effectiveness ratios generated through probabilistic sensitivity analysis, varying model parameters through the ranges shown in Supplementary Table 1. All costs are in 2018 US$. Costs, QALYs, and DALYs are discounted at a base-case value of 3% per year.
Using base-case model parameters over a 10-y time horizon, ICERs were $15,593 per HIV infection averted (95% CrI: 11,161, 16,129), $22,082 per death averted (95% CrI: 15,785, 22,798), $2,355 per QALY gained (95% CrI: 1,667, 2,413), and $2,528 per DALY averted (95% CrI: 1,798, 2,599; Table 2). After 15 y, family-based care environments still did not surpass the upper WHO-CHOICE cost-effectiveness threshold (∼$5,100 per DALY averted; Figure 1a, b).

(a) Cost-effectiveness plane for incremental costs and effects. Bootstrapped replications: 1,000; time horizon: 15 y. Incremental costs represent the difference in annual per-child expenditures (2018 US$) between family-based care environments and street-based self-care. Incremental effects represent the difference in DALYs averted between family-based care environments and street-based self-care. (b) Cost-effectiveness acceptability curve for WTP per DALY averted. Bootstrapped replications: 1,000. Vertical dashed lines represent 1 and 3 time(s) Kenya’s gross domestic product per capita in 2018 ($1,708 and $5,124, respectively). DALYs, disability adjusted life years; WTP, willingness to pay.
Predictions of the 15-y ICER of $/DALY averted by family-based care were most sensitive to the probability of new HIV infections and deaths occurring among children in street-based self-care and to the recurrent cost(s) associated with providing care to children in family-based settings (Supplementary Figure 1). Modeled ICER predictions over 15 y were not substantively affected by assumptions regarding reductions in the probability of adverse outcomes among street-connected youth; family-based settings were still cost-effective at 2 times Kenya’s GDP per capita even after decreasing the probability of HIV infection and death in street-connected youth by 20% (Figure 2). Increasing the annual per-child costs for residents of family-based care environments by 25% similarly had a minimal impact on the ICER. However, after increasing the annual cost per child in family-based care to the equivalent mean annual cost per child in institutional settings (∼$2,100 per child per year based on our prior estimates for the OSCAR cohort 31 ), family-based care was no longer cost-effective compared with the status quo (Figure 2).
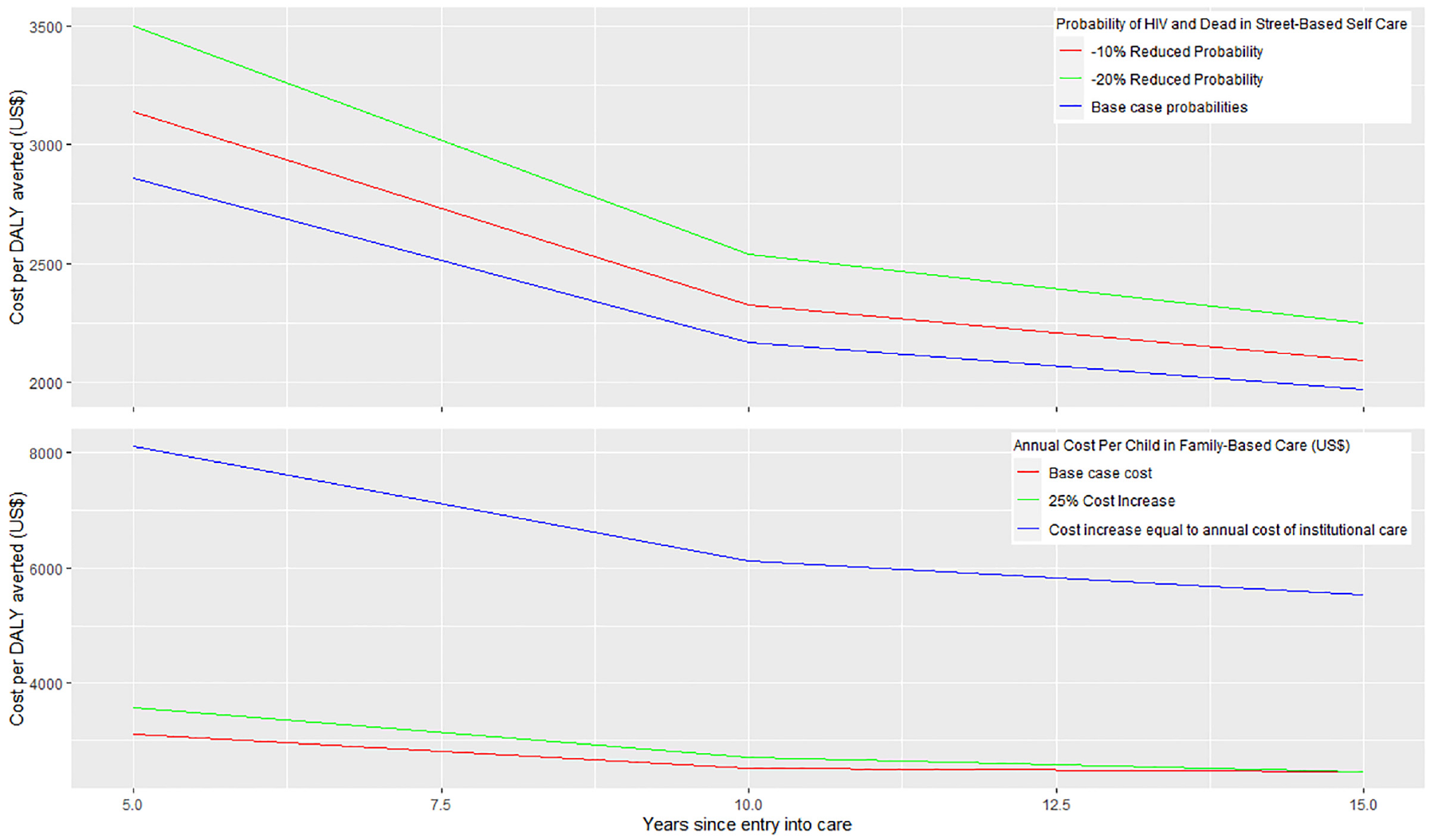
Model sensitivity to key assumptions surrounding (1) probability of HIV and death among street-connected youth and (2) annual per-child costs of family-based care. The top figure shows the impact of reducing the probability of both HIV infection and death by 10% and 20% among street-connected youth on the incremental cost-effectiveness ratio over 15 y. The bottom figure shows the impact of increasing annual per-child expenditures among family-based care environments on the incremental cost-effectiveness ratio over 15 y. DALY, disability-adjusted life year.
Households that received 2,000 Kenyan Shillings (∼US$ 20) per month as participants of the Kenya Cash Transfer for Orphans and Vulnerable Children (CT-OVC) social protection program spent $658 (95% CrI: 603, 713) per child per year on average compared with $637 (95% CrI: 599, 676) in non–cash-transfer households. The additional per-child expenditures did not correlate with improved outcomes; cash-transfer households had moderately higher ICERs compared with non–cash-transfer households (ICERs of $2,666 and $2,102, respectively, over 10 y). However, both cash-transfer and non–cash-transfer households remained highly cost-effective in terms of $/DALY averted compared with street-based self-care (Supplementary Table 2 and Supplementary Figure 2a, b).
Results from additional sensitivity analyses did not meaningfully change our inferences. Specifically, family-based care was still cost-effective at twice Kenya’s GDP per capita even after assuming an additional annual societal cost of $319 per pediatric patient residing in family-based care and newly initiating HIV treatment (including antiretroviral medication 32 ; Supplementary Table 3). As expected, assigning additional costs to provide care to street-connected youth (e.g., meals, voluntary medical male circumcision, HIV prevention training) reduced the modeled ICERs at all time points (Supplementary Table 4).
Discussion
Supporting family-based care for orphaned and separated children costs $645 (95% CrI: 614, 677) per child per year in Kenya and is highly cost-effective in settings where the probability of HIV and death is high among children who are left to care for themselves on the street. Our model-based predictions were most sensitive to assumptions regarding the probability of adverse physical health outcomes occurring among street-connected youth and to the recurrent cost(s) associated with providing care to children in family-based settings. The total annual cost to provide care to a child in an informal, family-based environment can potentially be increased by at least 25% and still remain cost-effective over a 15-y horizon.
Our results are similar to available cost estimates for orphaned and separated children receiving informal care in sub-Saharan Africa. A systematic review by Santa-Ana-Tellez et al. 11 found that the annual cost per child in foster care settings in sub-Saharan Africa ranged from $614 to $1,921 (2010 USD). Care programs for orphans and vulnerable children in Eritrea and Benin have an annual cost per child of $100 for family integration, 14 while similar informal fostering and home-based care programs in South Africa carry a monthly cost of US$ 55 per child.12,13 In the current study, we found that family-based settings spent the greatest proportion of annual expenditures on food and education, suggesting that family-based settings have the capacity to simultaneously provide for both immediate basic needs and longer-term development.
In general, our ICER estimates are higher than those of other HIV prevention interventions specific to OSCA in SSA. Two studies estimated ICERs as low as US$6/QALY gained to provide economic school support (e.g., fees, books, uniforms) for orphan girls in Zimbabwe 33 and US$267/DALY averted through combined medical male circumcision with HIV education for street-connected youth in Kenya. 34 However, these studies differ in several key features from the OSCAR Health and Well-Being study, most notably in their frequency and duration of intervention delivery for a maximum of 3 y 33 or over 30 d during a one-off period 34 (v. daily family-based support for a median of 6.9 y among participants of the OSCAR cohort 15 ). Furthermore, our 10-y ICER estimates of $15,593 per HIV infection averted are comparable with those for daily PrEP implementation strategies targeted to adolescent males and females in SSA, which range from $5,723 to $67,970 per HIV infection averted over 10-y horizons, 35 as well as to longer-term community-based and combination HIV prevention packages for adults, which produce median ICER values up to $22,000/HIV infection averted. 36
Our study has a number of strengths. To our knowledge, ours is the first health economic modeling study to incorporate real-world longitudinal cost and effectiveness data from more than 1,300 OSCA living in randomly selected households or practicing self-care on the streets in Kenya. In addition, our model incorporates a full uncertainty analysis involving tornado plots for univariate analysis and probabilistic sensitivity analysis to provide 95% CrIs for primary ICERs to characterize the uncertainty in our model parameters. Our study also includes additional scenario analyses exploring how different assumptions for the most influential parameters affect the primary cost-effectiveness metric ($/DALY averted). Lastly, our study estimates the cost-utility of family-based care over 15 y, which is longer than most orphaned and separated children remain in a care environment before aging into adulthood. Thus, our model includes a long enough time interval to be able to capture that majority of new HIV infections and deaths expected to occur in this population and to inform longer-term cost-effectiveness of familial care after children transition out of care.
Our study also has limitations. Our Markov model assumes that transition probabilities between health states do not change with time. However, it is likely that the probability of HIV infection or death will change over time as children age into and out of adolescence or by differences within household environments. Another limitation is that our model uses effectiveness data from the OSCAR cohort, which is solely concerned with tracking primary HIV infections as opposed to all HIV transmissions. Given that our model was sensitive to the probability of new HIV infections occurring among street-connected youth, it is possible that including secondary and tertiary transmissions would affect our cost-effectiveness ratios. In addition, we used the most commonly cited threshold for determining cost-effectiveness but acknowledge that other cost-effectiveness thresholds may be more appropriate in some instances.29,37 Lastly, this analysis was concerned with estimating the cost-effectiveness of family-based care in terms of the ability of these settings to prevent HIV and death among orphans and vulnerable children who would otherwise be on the street. The ICERs from this analysis would likely change if nonclinical outcomes (e.g., educational attainment38,39) were considered. Our ICER estimates are also limited by the data available related to the costs of the growing number of street-connected youth in Kenya. ICERs from this analysis would likely have been reduced if we had included additional societal costs associated with street-connected youth, such as the cost(s) of crime and physical abuse that can occur within and against this population due to their state of homelessness.40–42
Estimates from this economic modeling analysis hold national and regional implications. At the national level, Kenya’s most recent Child Budget Analysis indicates that overall budget allocations to child protection programs—including the Cash Transfers to Orphans and Vulnerable Children program and alternative family care services—are decreasing despite national policy ambitions of cushioning vulnerable children (9% decrease in the Ministry of Labour, Social Security & Services’ total child budget from 2014–2015). 43 Estimates from this analysis could therefore help guide resource reallocation from less effective, costlier child protection programs to evidence-based family care services. At the regional level, this analysis directly responds to calls from UNICEF and other global health advocates7,8 for new evidence that can inform a pragmatic scale up of family-based settings for orphans and vulnerable children. Our findings add to and update the evidence base supporting family-based care as a cost-effective option for vulnerable children that countries should prioritize over the status quo.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683221143782 – Supplemental material for Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model–Based Simulation
Supplemental material, sj-docx-1-mpp-10.1177_23814683221143782 for Cost Utility of Supporting Family-Based Care to Prevent HIV and Deaths among Orphaned and Separated Children in East Africa: A Markov Model–Based Simulation by Marta Wilson-Barthes, Paula Braitstein, Allison DeLong, David Ayuku, Lukoye Atwoli, Edwin Sang and Omar Galárraga in MDM Policy & Practice
Footnotes
Acknowledgements
We gratefully acknowledge the Chiefs, Assistant Chiefs, and Village Elders of the Locations of Pioneer, Kapsoya, Koisagat, Ol’Lenguse, Olare, Tarakwa, Kipsinende, and Kapyemit for their support and leadership. We also wish to acknowledge all the residents of these Locations and particularly the many households caring for vulnerable members of their community, notably orphaned and separated children and children with physical and mental disabilities. We particularly want to acknowledge the County and District Children’s Officers for their dedication to protecting the children of Uasin Gishu County, as well as the Uasin Gishu Children’s Services Forum. We thank Elsie Mugonyole and Allan Kamanda for their hard work and excellent research assistance.
This study would not have been possible without the willing participation of the children and youth participants and their guardians, and we would like to acknowledge and thank them. The enthusiasm and commitment of the staff and volunteers of the OSCAR project have not gone unnoticed, and we, the authors, wish to thank them for their efforts and engagement with this project.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award No. R01HD060478. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Author Contributions
P.B. obtained the funding to support this analysis. P.B. and O.G. were responsible for the concept and design of this economic evaluation and oversaw all data acquisition. D.A. and L.A. provided expert feedback on study design and culturally appropriate methods for data acquisition. M.W.B., A.D., E.S., and O.G. were responsible for the data analysis and interpretation. M.W.B wrote the first draft of the paper. All authors discussed results, reviewed the manuscript critically for important intellectual content, and approved the final version of the article for submission. All authors had full access to the data on which the reported findings are based.
Ethics Approval
The Orphaned and Separated Children’s Assessments Related to their (OSCAR’s) Health and Well-Being Project was approved by the Moi University College of Health Sciences and the Moi Teaching and Referral Hospital Institutional Research and Ethics Committee, the Indiana University Institutional Review Board, and the University of Toronto Research Ethics Board. Written informed consent for participation was provided by the head of household or, in the case of street-connected youths, by the district (now county) children’s officer. Individual written informed assent was provided by each child 7 y or older. Fingerprints were used for children and guardians who were unable to sign or write their names.
Supplemental Material
Data Availability
The R code for the Markov model(s) is publically available in the following digital repository: ![]() . All other analytic code (e.g., used for data cleaning or formatting the figures and tables in this paper) and the original deidentified data sets will be made available by the first author (
. All other analytic code (e.g., used for data cleaning or formatting the figures and tables in this paper) and the original deidentified data sets will be made available by the first author (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.