
Abstract
Highlights
This is one of the first studies to assess decision regret among caregivers of older adults receiving home and community care services and to identify their most frequent difficult decisions.
Difficult decisions were most frequently about housing and safety. Most caregivers of older adults in all 10 provinces of Canada experienced decision regret.
Factors associated with less decision regret included higher caregiver age, the involvement of other family members in the decision-making process, wanting to receive information about the options, considering organizations interested in the decision topic, and health care professionals as trustworthy sources of information. Factors associated with more decision regret included mismatch between the caregiver’s preferred option and the decision made, the involvement of spouses in the decision-making process, higher decisional conflict, and higher burden of care.
This is a visual representation of the abstract.
Keywords
Background
In Canada, people aged 65 y or older (older adults) have outnumbered children younger than 14 y since 2016.1,2 The need for health services and independence support services provided at home will thus increase significantly because of the burden of chronic conditions and loss of personal autonomy. The current trend in Canadian health services is to promote aging at home for as long as possible and especially since 2020–2021, when long-term care facilities were disproportionately affected by COVID-19. Canada had the highest proportion of deaths in long-term care of all Organisation for Economic Co-operation and Development countries.3–6
Aging at home will require improving home and community care services (henceforth referred to as “home care”) for older adults. Home care services are public and private services delivered in people’s homes (including in seniors’ private residences) by regulated health and social care professionals (e.g., nurses, dietitians, social workers) and nonregulated workers (e.g., personal support workers). 7 The goal is to help people stay at or return home and receive needed treatment, rehabilitation, or palliative care.
However, even in households already receiving home care services, informal caregivers provide much of the care. In 2018, 25% of Canadians aged 15 y and older defined themselves as caregivers, and 40% of people receiving home care services were older adults. Nearly 9 of 10 care recipients received care from family or friends.1,8,9 Caregivers provide practical help in daily living activities and also help with complex medical and nursing tasks that elsewhere are performed by trained professionals. 9 Caregivers may thus be involved in difficult decisions, with or on behalf of a dependent older adult, related to their health and social care. 10 We have little information about the proportion of caregivers who are routinely involved in decisions, but in a systematic review on caregivers of older adults, the caregivers indicated that there are gaps in the support they receive for making informed decisions and that these gaps lead to negative emotions, including decision regret. 10
Decision regret is a negative emotion experienced when one realizes or imagines that the current situation would have been better if a decision made in the past had been different.11,12 A study evaluating regret compared with other emotions (e.g., love, shame, guilt, fear) concluded that people put much more emphasis on regret than on other negative emotions. 13 Indeed, one study found that regret was the most common emotion in daily life. 14 Inadequate decision-making processes often precipitate expressions of regret,15,16 and regret, in turn, may translate into negative outcomes such as lower satisfaction with treatment, complaints, and a reduced quality of life.17–19 Some studies show links between decision regret among caregivers and decision-making processes such as being clear about values, playing the role desired in the decision making, sharing decision making, and feeling informed and supported.20,21 Other factors associated with regret were caregiver characteristics (e.g., age, civil status, level of education), decisional conflict, burden of care, and caregiver role.18,22 Regarding the kind of decisions caregivers may regret, numerous studies show caregiver regret as associated with end-of-life decisions23–27 and decisions about housing.20,28 However, none of these studies focused exclusively on caregivers of older people receiving home care services.
In the context of home care, identifying decisions caregivers consider most difficult and measuring decision regret and the factors that influence regret could help determine whether existing programs meet decision-making needs, establish priorities, and develop new programs. 29
For home care clients and their caregivers, the most difficult decisions can change, not only because of changing health status but also external circumstances. During the COVID-19 pandemic, caregivers faced unprecedented challenges when they found they were no longer able to provide care for their loved one at home.9,30,31 In planning a decision to move them into a seniors’ residence, they had to consider that residents were dying or were confined to their rooms and allowed no visitors. In fact, many caregivers moved their loved ones back into their own homes if they were able to.9,32,33
Informed by an adapted conceptual framework (Figure 1) and the literature on predictors of regret, we hypothesized that higher decisional conflict, higher burden of care, unfavorable socioeconomic characteristics, and lower caregiver age would be associated with more decision regret.15,18,22

Conceptual framework of shared decision making with caregivers of older adults receiving home care, adapted from Sepucha and Mulley. 15
Therefore, we aimed to identify the most frequent difficult decision caregivers had to make for older adults receiving home care services, measure decision regret, and identify factors associated with decision regret.
Methods
Study Design
We conducted a cross-sectional online survey across the 10 Canadian provinces of adults who identified themselves as caregivers of older adults who had received home care services in the past year.
We report the results according to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 34 This project is part of the initial phase of a 7-y program, funded by a Canadian Institutes for Health Research peer-reviewed grant, whose overarching goal is to ensure that more Canadian older adults receiving care at home and their caregivers become fully engaged as partners in their care. 35
Participants and Recruitment
We used a pan-Canadian Web panel (Leger Marketing) to conduct our survey. With 400,000 individuals from the 10 provinces (the 3 territories are excluded from the sampling frame), the Leger Marketing panel is the largest Canadian online panel representative of the Canadian population. 36 To ensure the quality of the panel, Leger Marketing uses several internal control measures such as a double-consent process and regular update of panelist profiles every 6 mo. For this voluntary survey, a nonprobability sampling method was used to invite 97,568 panelists aged 18 y and older (that year) to participate. Eligible participants were caregivers of older adults receiving or having received home care services over the past year. Ethical approval was obtained from the Research Ethics Board of the Integrated University Health and Social Services Center of the Capitale-Nationale, Quebec, Canada. Consent to participate in the study was indicated by answering the question at the beginning of the survey. All information collected in this survey remains confidential, anonymous, and will be used only for scientific purposes. Data are stored on secure servers.
Measures
We adapted a self-administered questionnaire to identify the most difficult decision and the decision regret of caregivers of older adults receiving home care as well as other characteristics of the decision-making process (Figure 1) potentially associated with regret such as information format and trusted sources of information (see Appendix 1, Questionnaire). The questionnaire also included 4 validated scales for measuring regret, decisional conflict, burden of care, and preferred decision-making role.17,37–40 The questionnaire was based on the Ottawa Decision Support Framework, 41 the Decisional Needs Assessment in Populations Workbook, 29 and a conceptual framework for shared decision making adapted from a framework by Sepucha and Mulley. 15 The latter framework presents 3 phases of decision making: decision antecedents, decision-making processes, and decision outcomes. We adapted the framework by applying these phases to the theoretical relationship between health care professionals, older adults, and caregivers during the process of shared decision making in the context of home care (Figure 1). We also used the framework to formulate hypotheses about factors that might be associated with decision regret among family caregivers of older adults receiving home care.
We considered as decision antecedents the sociodemographic characteristics of caregivers that could influence the decision-making process and their choices when faced with difficult decisions. The study questionnaire included 11 sociodemographic variables.
To identify difficult decisions for caregivers of older adults, we consulted a preliminary study conducted with older adults and caregivers within a large Canadian home and community care organization as well as expert opinion. 42 Based on these data, we proposed a list of 15 potentially difficult decisions faced by older adults and their caregivers over the past year. From these, caregivers were asked to select the most difficult decision they had made regarding their relative during the past year, such as, “Should my relative stay at home or move?” (e.g., nursing home, family member’s home, private senior’s residence) or “Should my relative get surgery or not?” (see Appendix 1, Questionnaire).
Decision regret was measured using the validated Decision Regret Scale (DRS). 19 This scale consists of 5 items, each with a Likert-type response scale ranging from 1 = strongly agree to 5 = strongly disagree.17,19 The respondent must indicate agreement or disagreement with the following statements by choosing what best corresponds to their opinion as a result of a decision made: 1) It was the right decision, 2) I regret the choice that was made, 3) I would go for the same choice if I had to do it over again, 4) The choice did me a lot of harm, and 5) This decision was a wise one. To obtain a score, scores from items 2 and 4 are reversed, all items are summed, and the total is divided by 5. To ease interpretation, the global score is converted to a 0 to 100 scale (0 = no regret to 100 = high regret) by subtracting 1 from each item and multiplying by 25. The items are summed and the mean calculated. Scores thus ranged from 0 (no regret) to 100 (high regret). The literature suggests that a DRS score of 1 to 25 is mild, and a score of greater than 26 is moderate to strong.18,43–45 However, there is currently no consensus on cutoff points for the scale and no guideline to indicate what scores should be considered clinically significant.18,44 DRS has good internal psychometric properties (Cronbach α = 0.76) and correlates with decision satisfaction, decision conflict, and the overall quality of life.17,19
In accordance with our conceptual framework, we assessed other variables with 3 other scales and items (Appendices 1 and 2):
Decisional conflict: uncertainty about what to do when choosing among options. Items relate to discomfort with the decision to be made, questioning personal life values, uncertainty, feeling uninformed, feeling unclear about personal values, and feeling unsupported in decision making. Decisional conflict was measured using the multidimensional validated Decision Conflict Scale (DCS), 16 items rated on a 5-point scale (strongly agree, agree, neither agree nor disagree, disagree, and strongly disagree). The DCS score ranges from 0 to 100. Scores lower than 25 are associated with implementing decisions, and scores exceeding 37.5 are associated with decision delay or feeling unsure about implementation.
Burden of care among caregivers: caregiver’s perception of activities performed for the older adult and emotions connected with these tasks. It is measured using the validated 22-item Zarit Burden Interview scale (ZBI). Questions are evaluated using 5 statements with 4 possible responses (0 = never, 1 = rarely, 2 = sometimes, 3 = quite often, 4 = almost always). For each question, respondents are asked how often they feel this way. The total score represents the sum of the scores obtained for all 22 items, ranging from 0 to 88. A score ≤20 indicates little or no burden, a score between 21 and 40 indicates a light burden, a score between 41 and 60 indicates a moderate burden, and a score >60 indicates a severe burden. In addition, the multidimensional ZBI reveals 3 dimensions of the burden on caregivers: the direct impact of caregiving on the lives of caregivers and feelings of guilt and frustration (or embarrassment).46,47
Participation in the decision: the people involved in the decision, the caregiver’s preferred decision-making role, and the role they assumed in the decision making was measured using the validated Preference Control Scale (a 5-point response scale).48,49
Questionnaire Administration
The final questionnaire (available on request) was pretested with a random sample of 13 eligible panelists before data collection began. From March 13 to 30, 2020, we conducted a cross-sectional survey (coinciding with the beginning of a COVID-19 lockdown in most of the country). A unique URL link to the closed survey was sent by email to participants, allowing them to access the survey in English or French. Respondents logged in using their panel member account, which allows only 1 validation per member to prevent duplication. The questions appeared in the same order for all participants: there was no randomization of questions or alternations. Participants had to answer all the questions on one page to move to the next one and had to click on the “Finish” button on the last page to validate their answers. Each page included a “Back” button to change the answer and a button with a list of older adult helplines for each province. There was no summary of participants’ responses asking if they wished to correct them. The survey was voluntary, and $1 compensation was offered to participants.
Sample Size
Web surveys typically have a response rate that varies from 10% to 20%, depending on the respondents’ occupations.50–53 The average response rate among the active Leger panelists was around 20%, and ours was approximately 52%. The sample size was estimated using the central limit theorem formula
Data Analysis
First, the variables of age, decisional conflict, and burden of care were analyzed as continuous variables. The other independent variables were analyzed as categorical variables. After discussion, authors chose to organize the difficult decisions into 3 categories for statistical analysis with the DRS: housing and safety, management of health conditions, and end-of-life. Housing and safety were grouped together, as housing decisions are often provoked by safety concerns at home, the need for supervision in case of falls, or the older person’s inability to take care of himself or herself in the judgment of their families or home care staff.55–57 We also grouped them together as they are not necessarily medical decisions, unlike decisions about medication or pain management, for example. We used descriptive statistics to summarize the variables. For the DRS, DCS, and ZBI, we verified internal consistency by calculating Cronbach alphas. We performed the Kolmogorov–Smirnov test to evaluate the distribution of DRS scores and other variables and verify the postulate of normality. 58 The DRS was analyzed as a continuous variable using general linear models. This is common in studies whose principal outcome is evaluating decisional regret. 18 A continuous scale allows a better understanding of the event, and the statistical treatment of the continuous variable is respected.
Regression modeling included only participants with complete data on all potential factors. The “prefer not to answer” choice for the variables was considered as missing data for simple and multiple regression analyses. Simple linear regressions with decisional regret as outcomes were performed for each independent variable. Variables estimated as significant (i.e., P < 0.20) in the bivariable linear regression models were entered in the multivariable linear regression model.59,60 Factors associated with decision regret were identified using a stepwise selection 61 based on Schwarz’s Bayesian information criterion. 62 Correlations were performed between the variables. All analyses were performed using SAS. 63
Results
Characteristics of Participants
A total of 932 participants completed the survey (Figure 2). The view rate (ratio of unique survey visitors/unique receiver of survey invitation) was 13.6%, the participation rate (ratio of users who agreed to participate/unique survey visitors) was 8.6%, and the completion rate (ratio of users who completed the survey/users who agreed to participate) was 82.2% (Figure 2). The mean time to complete the questionnaire was 15:13 min, and the median time was 10:17 min. No data were missing, as the Web-based questionnaire did not accept unanswered items.

Flow chart of participant recruitment.
Most participants were male (58.4%), and their mean (SD) age was 42.2 (15.6) y (Table 1). Most were Caucasian (68.1%), university educated (59.9%), legally married (48.3%), and lived in central Canada (65.5%). The most common relationship of caregivers to the older adults in their care was child–mother (34%). Most caregivers had assumed an active role in the decision-making process (n = 858, 92.1%) and preferred to play an active role in the future (n = 865, 92.8%; Table 2). Also, 389 participants (41.8%) felt a moderate to severe burden of care when taking care of their relative (Table 2).
Caregivers’ Sociodemographic Characteristics (N = 932)
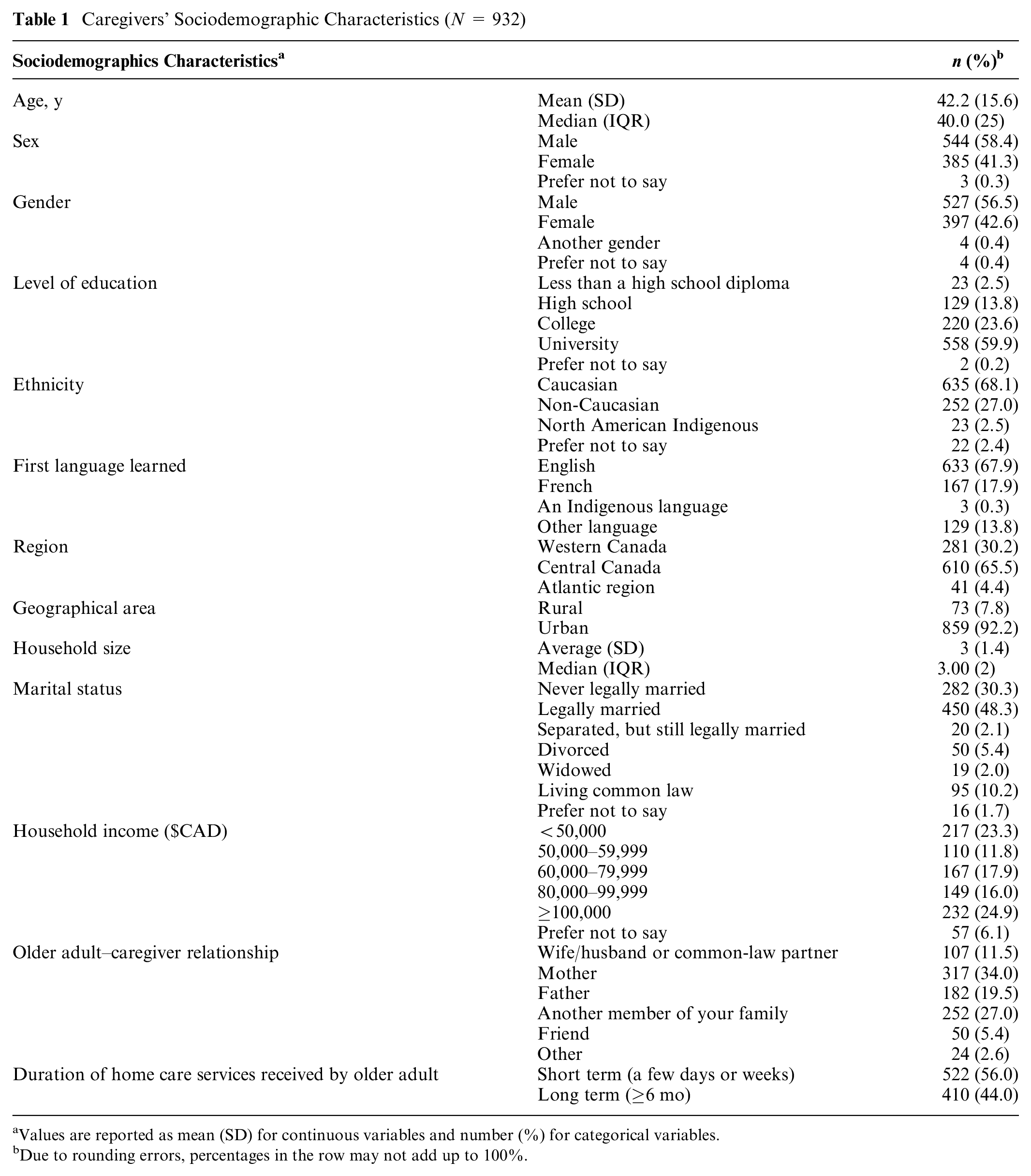
Values are reported as mean (SD) for continuous variables and number (%) for categorical variables.
Due to rounding errors, percentages in the row may not add up to 100%.
Distribution of Decision Regret Scores and Characteristics of the Process of Shared Decision Making (N = 932)
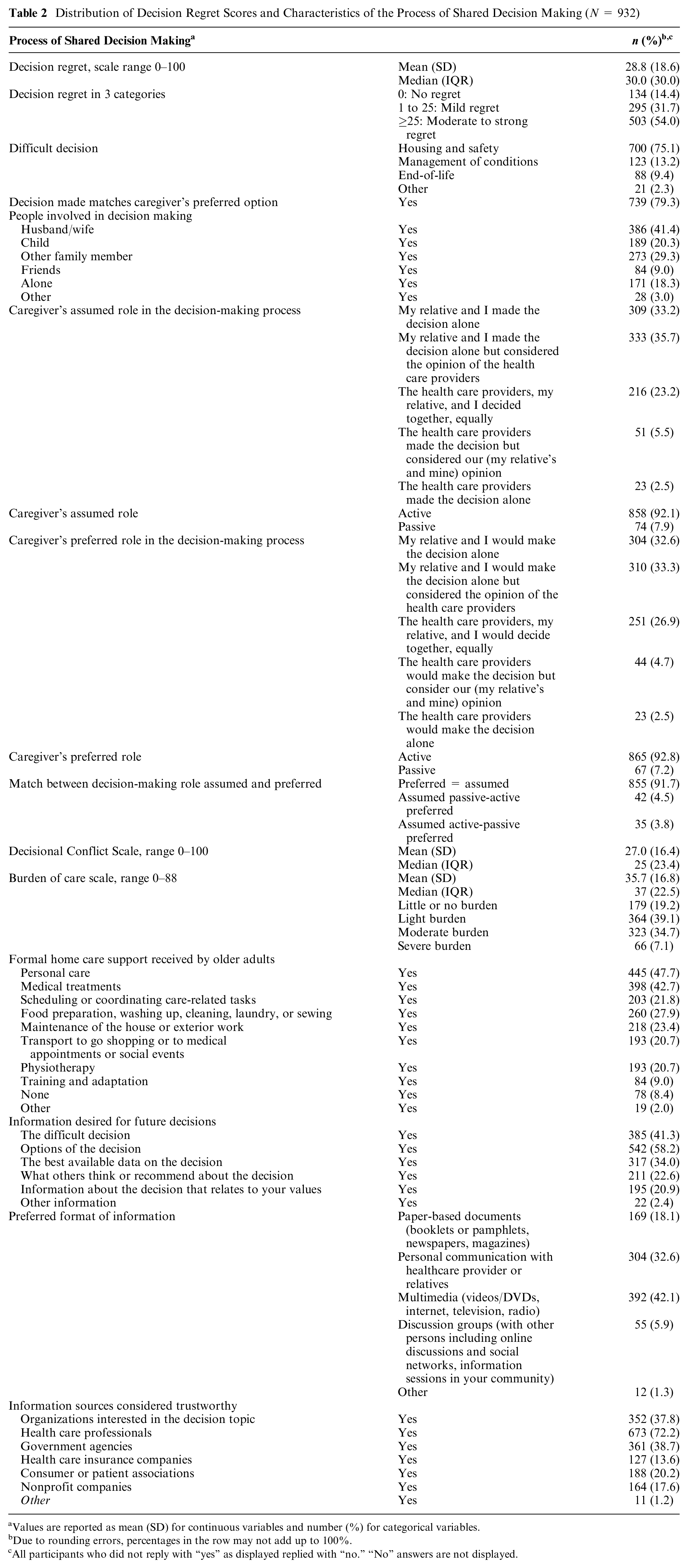
Values are reported as mean (SD) for continuous variables and number (%) for categorical variables.
Due to rounding errors, percentages in the row may not add up to 100%.
All participants who did not reply with “yes” as displayed replied with “no.” “No” answers are not displayed.
Of the 198 eligible participants who did not complete the questionnaire, only 45 gave their consent and answered the sociodemographic questions. Of the 45 withdrawn participants, 73.2% were women, with an average (SD) age of 47.7 (15.9) y. Their sociodemographic characteristics were similar to those of the participants: mostly Caucasian, university educated, English as the first language learned, coming from central Canada, and caring for their mother. Most participants who did not complete the questionnaire or dropped out of the study without giving their consent were women and people with a low level of education.
Difficult Decisions
The 3 most frequently reported difficult decisions over the past year were “should my relative stay at home or move?” (n = 326, 35.0%), “what is the best option for my relative for staying safe at home?” (n = 142, 15.2%), and “what is the best option for my relative for preventing falls?” (n = 97, 10.4%; Table 3). All 3 related to the category of housing and safety. The frequencies of the most difficult decisions reported per category were 75.1% relating to housing and safety, 13.2% relating to management of health conditions, and 9.4% relating to end of life. “Other” decisions (2.3%) related to a variety of themes (data available on request).
Descriptive Statistics of Decision Points (N = 932)

Decision Regret
The DRS showed a Cronbach’s coefficient of 0.76. DRS scores ranged from 0 to 100. The mean (SD) DRS score was 28.8 of 100 (18.6), and the median was 30.0 (Table 2). Of the 932 caregivers, 134 (14.4%) reported no decision regret (DRS scores of 0), whereas 798 (85.6%) reported some level of decision regret. More than half of participants (n = 503, 54.0%) experienced moderate to strong regret, with DRS scores greater than 25. Among the 3 categories, decisions relating to end of life had the highest mean (SD) decisional regret score (30.2 [18.1]), followed by those relating to housing and safety (28.7 [18.6]) and to the management of health conditions (28.3 [17.5]). Among all 3 categories, the decision with the highest mean decision regret score was “what is the best option for advance care planning?” (31.7 [14.2]; Table 3). Those identified as “other” difficult decisions had a higher mean decision regret score (32.4 [24.1]).
Factors Associated with Decision Regret
Factors significantly associated with decision regret when examined individually in bivariable linear regression with the statistical significance threshold of P > 0.20 are shown in Appendix 3. Analyses showed no collinearity between decision regret and other variables. Factors associated with less decision regret included higher caregiver age (P < 0.001), the involvement of other family members in the decision-making process (P = 0.005), wanting to receive information about the options (P < 0.001), considering organizations interested in the decision topic (P = 0.001), and health care professionals as trustworthy sources of information (P < 0.001). Factors associated with more decision regret included mismatch between the caregiver’s preferred option and the decision made (P < 0.001), the involvement of spouses in the decision-making process (P = 0.001), higher decisional conflict (P < 0.001), and higher burden of care (P < 0.001; Table 4). Contrary to one of our hypotheses, lower socioeconomic status was not associated with more decision regret.
Multivariable Factors Associated with Decision Regret among Caregivers of Older Adults Receiving Home Care Based on Stepwise Selection with Schwarz’s Bayesian Information Criterion (N = 932) a

The estimates β for each covariate and its 95% CI are presented. β = mean difference; CI = confidence interval. Adjusted R 2 = 43.44%.
Discussion
We identified difficult decisions, measured decision regret, and identified factors associated with decision regret among caregivers who had made decisions for older adults receiving home care in all 10 provinces of Canada. Housing and safety decisions were the most frequently reported as most difficult. More than half of participants reported moderate to strong regret, with end-of-life decisions showing the highest level of regret. The factors associated with most regret were mismatch between the caregiver’s preferred option and the decision made, the involvement of spouses in the decision-making process, higher decisional conflict, and higher burden of care. The factors associated with the least regret were higher caregiver age, the involvement of other family members, wanting to receive information about the options, and considering organizations interested in the decision topic and health care professionals as reliable information sources. These results led us to make the following observations.
First, to the best of our knowledge, this is among the first studies focusing exclusively on caregivers of older adults receiving care at home to identify which decisions they most frequently experience as difficult. Under the category of housing and safety, decisions about moving, home safety, and fall prevention were most frequently reported. Decisions about social determinants of health such as those associated with housing and safety clearly superseded more biomedical decisions such as those about drugs and tests. Having to leave one’s home can be a highly distressing experience of loss and displacement.16,64–68 A systematic review found that the experience of falls and feelings of insecurity or fear were among the factors influencing housing decisions among frail older adults. 57 It is worth noting that as this survey was rolled out at the end of March 2020, it is likely that our results were affected by the COVID-19 pandemic. In Canada, the difficulty in making decisions about housing and safety was compounded by the fact that in 2020, more than half of all COVID-19–related deaths were nursing home residents.3,4 During the pandemic, 2 decision aids designed to support families making decisions about moving their relative were downloaded more than 10,000 times in 3 wk, indicating the urgent need for effective decision support in this area. 69 As the COVID-19 experience may propel an increase in preference for aging at home rather than in nursing homes or private senior residences, decisions about safety at home will only increase in importance. 56 Caregivers should be kept up to date on new options to help older adults stay safe. 56 This would allow them to better address the issue of safety and make informed decisions.55,56
Second, in our study, the average score of caregiver decision regret (28.8) was slightly higher than in other studies on decision regret among caregivers (12.5).20,22 Previous studies focused on different populations such as future mothers, caregivers of children, caregivers of adults, and older adults with a loss of autonomy. Also, other studies have mostly only dealt with one decision at a time, while our analysis made it possible to measure decision regret for several types of decision. Nevertheless, some of our results do confirm these individual-decision studies. For example, in our study, the highest levels of decision regret were in relation to end-of-life decisions, a finding consistent with results of other studies conducted in the end-of-life context.18,22,24,70
Third, as we expected, we found that caregiver’s higher age was associated with less decision regret. Age of relatives can be found as predictors elsewhere in the literature on decision regret.18,22,24,71 As caregivers age, they have more experience of dealing with the restrictions of old age, and they may have acquired health experiences that reduce their anxiety.
While other studies showed the presence of spouses or common-law partners as reducing decision regret, our results showed that their involvement in the decision-making process increased decision regret among caregivers.20,22 This may be because, as spouses, they are closer witnesses to the distress felt by the older person. However, our research indicated that having another family member involved in the decision-making process reduced decision regret, suggesting that if caregivers have additional family support, their regret may be relieved. 16 A 2018 survey found that children, spouses, extended family, friends, and the community represent the most common sources of support received by caregivers. Being a caregiver of an older adult is a common role among extended family members.72,73 The more other people are involved in caring for the older person, the more the caregiver can share the responsibilities and the burden of care and thus ultimately experience less decision regret.
Fourth, contrary to our expectations, we found no association between decision regret and unfavorable socioeconomic characteristics, such as having no more than a primary education. In the literature, higher regret is often observed in people with lower educational attainment.20,44 People with lower educational attainment or low health literacy may experience difficulty understanding the information necessary for making informed decisions. 74 This finding may be attributable to the fact that only 2.5% of our sample had less than a high school diploma and were therefore underrepresented in our sample.
Fifth, as expected, our study indicated that higher decisional conflict and higher burden of care increased decision regret. The literature confirms that these 2 factors are strongly associated with decision regret.17,20,75 Burden of care is associated with depression and anxiety, and anxiety breeds regret and dwelling on missed opportunities. 20 However, unlike sociodemographic factors such as age or education levels, decisional conflict and burden of care are factors that can be modified by the implementation of decision support interventions76,77 as well as by providing mental and financial resources for caregivers.78–81 Also, our data support our hypothesis that a match between the preferred option and the decision made would decrease decision regret. This reinforces how important it is to invite caregivers to express themselves on their preferred options and needs to better include them in the decision process. It also indicates how important it is for clinicians to become more competent in assessing the values and preferences of patients and of caregivers and also in assessing what options are indeed feasible. 82 The match between choice preferred and decision made could have been out of the control of caregivers due to a lack of options. For example, if a clinician offers the choice to an elderly person to move out or stay home, but their caregiver is no longer able to support the person at home, that option no longer exists, whatever they would have preferred. However, a choice that is regretted can later turn out to be the best choice, and support for seeing and acknowledging this can alleviate the pain of regret. Nevertheless, a real lack of options for this population also needs to be addressed at a system level, such as by improving home care.
Finally, our data showed that people who wanted to receive information about the options for future decisions, as well as those who considered relevant organizations interested in the decision topic and health professionals as trustworthy sources of information, were statistically less likely to experience decision regret. These results are congruent with those of other studies that have shown the importance of formal decision support and the utility of decision support tools. 83 A recent systematic review on the experiences of families caring for older adults showed that negative experiences reflected lack of information, while positive experiences were linked to formal as well as well as informal support. 57 Our results can inform the design of tools and programs for supporting caregivers with loved ones aging at home and for health care professionals and organizations who need the interprofessional SDM skills to support difficult decisions. An interprofessional SDM approach is particularly appropriate for home care, in which care may be provided by health care teams as well as caregivers. With our results, for example, interprofessional teams can collaborate with caregivers to better assess the risks of decision regret in terms of the decision types faced, the age of decision makers and family involvement in decision making.84,85
Limitations
Our study has a few limitations. The results are based on recall of the health decisions participants made over the previous year, and therefore, our data may have been subject to recall bias. Second, our sample may not be representative of all caregivers of older adults in Canada. For example, in Canada, more than half of caregivers are women, whereas 58.4% of our sample comprised men.8,86 The Leger panel is made up of 48% men and 52% women. Men are more likely to be Internet users (proficient users and advanced users) than women are, and male caregivers spend fewer hours per week providing care.1,87 Future recruitment strategies will create weighting that considers sociodemographic data such as sex and gender during sampling. In addition, 66% of participants were university educated, so people with limited literacy were underrepresented, and our sample frame did not include people from the 3 Canadian territories (more remote regions). Our results may therefore understate some of the decision-making difficulties specific to rural, female caregivers with less education. With online surveys, it is difficult to reach people with limited internet access, those with unfamiliarity with computers or mobile telephones (dexterity and literacy), and those who are living in remote areas.88–90 The Leger web panel uses demographic characteristics to set quotas for the sample. However, web panels use nonprobability sampling and therefore suffer from self-selection bias. Although propensity score adjustment is often used to try to remove this bias, we did not use it, as evidence of its effectiveness is mixed. 91 However, with face-to-face contact limited during the COVID-19 pandemic, an online panel was a practical if temporary solution. Future studies should include the Canadian territories, where there are large populations of Indigenous peoples, and adopt a culturally safe and relevant research lens. Fourth, it was challenging to interpret our decision regret scores because no clinical threshold for the DRS has yet been established in the literature.18,44 Thus, results on the frequency of decision regret identified as low, moderate, and high should be interpreted with caution. A consensus on the appropriate cutoff points for the DRS would better guide clinicians and researchers in using this important tool. Despite this drawback, a DRS version designed for caregivers, which better captures their subjective experiences, could be used for future studies. 92 Finally, this study began at the start of the COVID-19 lockdown in Canada, and the results may reflect the emotional state of caregivers of older adults in the context of a pandemic at its initial stage, rather than at all times before and after the pandemic.
Conclusion
We found that decision regret among caregivers of older adults receiving home care in Canada was high and that the difficult decisions made were most frequently about older adults’ housing and safety. In the decision-making process, the presence of family or friends to support caregivers, the life experience of the caregiver, and support tools created by organizations and health professionals can reduce decision regret. Our results may serve as a guideline for the creation of targeted strategies to provide effective decision support, such as the creation and dissemination of decision aids, interactive counseling, and self-help groups for caregivers of older adults receiving care at home. Ultimately, this will improve caregivers’ own health outcomes too and ensure Canada is at the forefront of ensuring caregivers’ well-being, a cornerstone of caring for a healthy aging population.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683221116304 – Supplemental material for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey
Supplemental material, sj-docx-1-mpp-10.1177_23814683221116304 for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey by Tania Lognon, Amédé Gogovor, Karine V. Plourde, Paul Holyoke, Claudia Lai, Emmanuelle Aubin, Kathy Kastner, Carolyn Canfield, Ron Beleno, Dawn Stacey, Louis-Paul Rivest and France Légaré in MDM Policy & Practice
Supplemental Material
sj-docx-2-mpp-10.1177_23814683221116304 – Supplemental material for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey
Supplemental material, sj-docx-2-mpp-10.1177_23814683221116304 for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey by Tania Lognon, Amédé Gogovor, Karine V. Plourde, Paul Holyoke, Claudia Lai, Emmanuelle Aubin, Kathy Kastner, Carolyn Canfield, Ron Beleno, Dawn Stacey, Louis-Paul Rivest and France Légaré in MDM Policy & Practice
Supplemental Material
sj-docx-3-mpp-10.1177_23814683221116304 – Supplemental material for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey
Supplemental material, sj-docx-3-mpp-10.1177_23814683221116304 for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey by Tania Lognon, Amédé Gogovor, Karine V. Plourde, Paul Holyoke, Claudia Lai, Emmanuelle Aubin, Kathy Kastner, Carolyn Canfield, Ron Beleno, Dawn Stacey, Louis-Paul Rivest and France Légaré in MDM Policy & Practice
Supplemental Material
sj-pdf-4-mpp-10.1177_23814683221116304 – Supplemental material for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey
Supplemental material, sj-pdf-4-mpp-10.1177_23814683221116304 for Predictors of Decision Regret among Caregivers of Older Canadians Receiving Home Care: A Cross-Sectional Online Survey by Tania Lognon, Amédé Gogovor, Karine V. Plourde, Paul Holyoke, Claudia Lai, Emmanuelle Aubin, Kathy Kastner, Carolyn Canfield, Ron Beleno, Dawn Stacey, Louis-Paul Rivest and France Légaré in MDM Policy & Practice
Footnotes
Acknowledgements
We thank our patient instructors Emmanuelle Aubin, Kathy Kastner, Carolyn Canfield, and Ron Beleno. We thank Louisa Blair for her editorial assistance. We also thank the Université Laval Statistics Consulting Services, Ghizlane Messaoudi, and Imane Benasseur for their help in the data analysis.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a Foundation Grant (No. FDN-159937) from the Canadian Institutes of Health Research (CIHR). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. FL holds a Tier 1 Canada Research Chair in Shared Decision Making and Knowledge Translation. LPR holds a Tier 1 Canada Research Chair in Statistical Sampling and Data Analysis. AG is funded by a CIHR Patient-Oriented Research fellowship. The funders are not involved in the project.
Authors’ Note
This study was undertaken at VITAM – Centre de recherche en santé durable, a Quebec research center associated with Université Laval. This work was presented in poster form at the Research Day of the Population Health and Optimal Health Practices of the CHU de Québec Research Center, June 4, 2021, and Research Days of Université Laval Faculty of Medicine and affiliated centers, May 25–27, 2021.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.