
Abstract
Highlights
We found clinicians’ antibiotic prescription decisions were driven by gist representations of antibiotic risks for a given hypothetical patient scenario, and clinicians’ gist representations and verbatim risk estimates about antibiotic-related risks were distinct from each other.
We showed that the effect of patient scenarios on clinicians’ antibiotic prescription decisions was mediated by clinicians’ gist representations.
Less experienced clinicians tend to “hedge” in their antibiotic prescription decisions compared with more experienced clinicians.
The broader impact of our study is that antibiotic stewardship programs can benefit by communicating the appropriate gists to clinicians who prescribe antibiotics for pediatric patients, rather than solely focusing on closing potential knowledge deficits of the clinicians.
Keywords
Clinicians’ Gists Drive Their Prescription Decisions
Unnecessary antibiotic prescription is a serious concern in medical practice, which can have severe public health consequences. Antibiotics can cause harm to the individual patient, including common side effects such as diarrhea, yeast infections, and rash, as well as more rare but severe adverse effects such as Clostridium difficile infections and anaphylaxis. 1 Antibiotic overprescription is a threat not only because of potential side effects but also because of their impact on the evolution of multi-drug–resistant bacterial strains. 1 Providers are extensively trained to identify appropriate treatments for a given medical condition. In the past 20 y, provider education and training have included topics of antibiotic resistance and the adverse effects of unnecessary antibiotics. Nonetheless, overprescription is still prevalent.2–7 In the pediatric ambulatory setting, antibiotics are prescribed in 1 out of every 5 ambulatory visits, 8 and at least one-third of these are unnecessary. 9 Acute otitis media (AOM), or middle ear infections, is the most common indication for antibiotic prescriptions in young children. 10
Prior work drew upon fuzzy-trace theory 11 —a leading theory of medical decision making 12 —to explain the relationship between providers’ risk perceptions and their prescribing practices in an emergency room setting.6,13 Fuzzy-trace theory posits that people make decisions based on a continuum of mental representations, ranging from the most precise, “verbatim” representation to the least precise “gist” representation.11,13 Verbatim representations capture the superficial details of the stimulus. Gist representations, on the other hand, focus on the bottom line meaning of that stimulus. Fuzzy-trace theory posits that gist representations are often the main drivers of decisions. 14
Fuzzy-trace theory hypothesizes that reliance on gist representations increases with developmental progress. In particular, experts tend to primarily rely on gist representations, whereas novices, who are developmentally less advanced, tend to rely on precise verbatim mental representations.11,15,16 Gist is context dependent, capturing the essence of a decision in a manner that draws on extensive background knowledge and expertis.11,17 Thus, experts are expected to have a greater ability to extract the appropriate gists.
Prior work studying fuzzy-trace theory’s predictions for antibiotic prescribing found that both patients who expected antibiotics and physicians who prescribed antibiotics endorsed a categorical gist representation of the prescribing decision in which patients were sick, and so antibiotics were prescribed because it was “better to be safe than sorry”—a gist that prior work called “why not take a risk?”5,6 However, when not clinically indicated, the “better to be safe than sorry” gist can underestimate the risks of prescribing antibiotics and overvalue the potential benefit of antibiotics.
Problem Context: Antibiotic Treatment for AOM
AOM is one of the major reasons for antibiotic prescriptions in children.10,18 AOM is a middle ear infection most commonly seen in children 6 mo to 5 y of age and is one of the most common types of infections among young children. AOM is a clinically distinct entity from otitis media with effusion (OME); although these 2 entities may present with similar symptoms, they can be distinguished by examination of the middle ear. For OME, antibiotics are not indicated based on current consensus guidelines. 19 For AOM, antibiotics are indicated for young children less than 2 y of age but could be safely deferred or delayed for nonsevere cases in children older than 2 y, as most of these infections will improve without antibiotics. 19 Therefore, if not diagnosed properly, prescribed antibiotic treatment may be unnecessary and potentially contribute to antibiotic resistance. Misdiagnosis may lead to either a missed antibiotic treatment (in case the infection is severe AOM) or an unnecessary prescription (in the case of OME misdiagnosed as AOM). 20 In either case, mismanagement eventually harms patients at the individual and population levels. The American Academy of Pediatrics provides guidelines to prevent such misdiagnosis and mistreatment. 19 Here, we explore how these guidelines or similar information material influences clinicians’ risk perceptions, numerical judgments, and decisions.
Hypotheses
Our hypotheses, derived from the predictions of fuzzy-trace theory about clinicians’ risk perceptions and judgments, are as follows.
Hypothesis 1: Clinical Scenario Predicts Gist
According to fuzzy-trace theory, expertise facilitates the extraction of appropriate gists in relevant contexts. 20 For example, a clinician may dismiss the potential harmful side effects of antibiotics and endorse the “why not take a risk?” gist in the context in which guidelines suggest that antibiotics may not be indicated. On the other hand, the same clinician may not endorse the same gist in a different context (i.e., if the harmful side effects are interpreted as nonnegligible). Therefore, we expect that participants’ gist endorsements about antibiotic-related risks will differ as the context of the hypothetical patient scenarios change.
Hypothesis 2: Gist Mediates the Relationship between Clinical Scenario and Antibiotic Prescription Decisions
It is natural to expect that providers’ behaviors would differ when they are given different scenarios. According to fuzzy-trace theory, this is because they encode different gist representations for these scenarios. We therefore hypothesize that the relationship between clinical scenario and providers’ antibiotic prescription decisions will be mediated by gist representations. In contrast, verbatim risk estimates should have relatively little impact on decision outcomes.
Hypothesis 3: Less Experienced Clinicians Tend to “Hedge” in Their Antibiotic Prescription Decisions, Compared with More Experienced Clinicians
Blalock and Reyna 21 argued that novices, who lack gist representations that are informed by expertise, are more likely to hedge, relying on middle-ground options. In contrast, experts tend to make “sharper all-or-none distinctions,” relying on categorical options because they are able to extract meaningful gists when applying their expertise. Similarly, Reyna and Lloyd 22 found that cardiologists with less experience were more likely to hedge when making decisions about intensive care unit admissions, consistent with experts’ being more likely to rely on categorical gist representations. We expect to see a similar pattern in our sample. Specifically, we hypothesize that more experienced clinicians will be more likely to choose to either immediately prescribe antibiotics or not prescribe antibiotics at all, whereas less experienced clinicians will be more likely to choose a hedging option (watchful waiting and follow-up with the patient).
Data Collection
We recruited providers who care for pediatric patients in the primary care and urgent care setting through the George Washington University Consumer Health Antibiotic Stewardship Working Group (CHASWG; see Appendix A). Participants were sent a survey—implemented using Qualtrics software—and received an optional $25 gift card upon survey completion. The study was approved by GWU's Institutional Review Board.
Methodology
Materials
We administered an online survey that included a set of items measuring clinicians’ risk perceptions and risky choices about antibiotic treatment. Participants were given the following tasks:
Patient Scenario Descriptions a

All of these scenarios differed only in terms of the symptoms, which include a sufficient level of details to indicate an antibiotic treatment or not. The scenarios were designed by 1 of the coauthors of the study (R.F.H.) based on the 2013 American Academy of Pediatrics Clinical Practice Guidelines. The “not indicated” scenario describes the ear exam of a child with otitis media with effusion, a condition for which antibiotics are not indicated. 19
Statistical Analysis Methodology
All analyses explained below were performed using R, version 3.6.2.
First, we encoded variables (see Appendix B for the variable-encoding process) and conducted an exploratory factor analysis (EFA). We used an oblimin rotation 25 to explain the variability in responses and thus identify common gists across survey items. We tested these hypotheses using these extracted factors, exploring the relationship between underlying gist themes and risky choices for each hypothetical patient scenario. To test hypothesis 1, we conducted multiple analyses of covariance for each of the 4 gist factors to investigate the extent to which gist endorsements differed across clinical scenarios (we controlled for multiple comparisons using the Holm-Bonferroni correction). Furthermore, we ran 4 regression analyses in which clinical scenarios are independent variables and gist endorsements are dependent variables. In addition, we examined whether providers’ numerical estimates of the probability that patients would improve without antibiotics differed across experimental condition.
To test hypothesis 2, we first used ordinal logistic regressions to examine the relationships between risky choices and expertise, gist endorsements, individual differences (i.e., numeracy and NFC), and relevant demographics. We encoded the variables for the ordinal logistic regression as follows: antibiotic prescription decisions were encoded as −1 for the “yes” option, 0 for the “maybe” option, and 1 for the “no” option. This enabled us to analyze the role of each of the gist factors as mediators between the prescription decision and the clinical scenario.
Finally, to analyze the hedging tendency across clinicians, we operationalized responses as “hedging” versus “nonhedging.” Specifically, we labeled the “maybe” option, which indicates watchful waiting as “hedging” and the “yes” and the “no” options as “not hedging.” We tested hypothesis 3 that expertise predicts hedging using logistic regression models. We also examined correlations between the number of years of experience and participants’ gist risk perceptions, risky choices, and verbatim risk estimates.
Results
Sample Characteristics
The sample included 260 (200 female; 77%) participants including attending and resident physicians, physician assistants, and nurse practitioners (Table 2). There were 84 participants randomly assigned to the “indicated” scenario, 87 to the “maybe indicated” scenario, and 89 to the “not indicated” scenario. Participants were experienced clinicians with an average of 12.19 y of experience (s = 9.61 y; Figure 1).

Histogram of clinicians’ number of years of experience. Years of experience are defined as time from medical or professional school graduation to time of participation in the study. Ten participants did not report their graduation years; thus, the following analyses were done on a sample size of 250 (10 participants did not report). We did not detect a difference in the years of experience among the experimental groups, F(2, 247) = 0.6, P = 0.54.
Sample Characteristics a

Average NFC score, scores ranging from 1 (strongly disagree) to 7 (strongly agree). Gender distributions did not differ across the experimental conditions, χ2(df = 2) = 0.65, P = 0.72.
Six participants did not report their gender.
Seven participants did not state whether they were Hispanic or non-Hispanic.
Nine participants did not report their professional titles.
The standard deviation of the average numeracy score was 0.16.
The standard deviation of the NFC was 0.35.
Exploratory Factor Analysis Results
We extracted 4 factors, minimizing the Bayesian information criterion (BIC = −3098.91; see Appendix C). Participants’ numerical risk estimates did not load on any of the extracted factors. Results were qualitatively consistent across factor rotation methods (see Appendix C and Appendix D.
Factor loadings are shown in Table 3 (also see Appendix E for the clinicians’ mean responses to each survey item). The first factor reflects the “why not take a risk?” gist. The second factor captures the “antibiotics might not help but can hurt” gist. The third factor captures the “antibiotics do NOT have harmful side effects” gist. Finally, the fourth factor captures the “antibiotics might have harmful side effects” gist. Although the first and fourth factor were anticorrelated (r = −0.35) in the factor analysis, they were statistically distinct, indicating that participants interpreted them differently. Verbatim risk estimates were not correlated with gist endorsements (Table 4).
Exploratory Factor Analysis Loadings (Oblimin Rotation) a
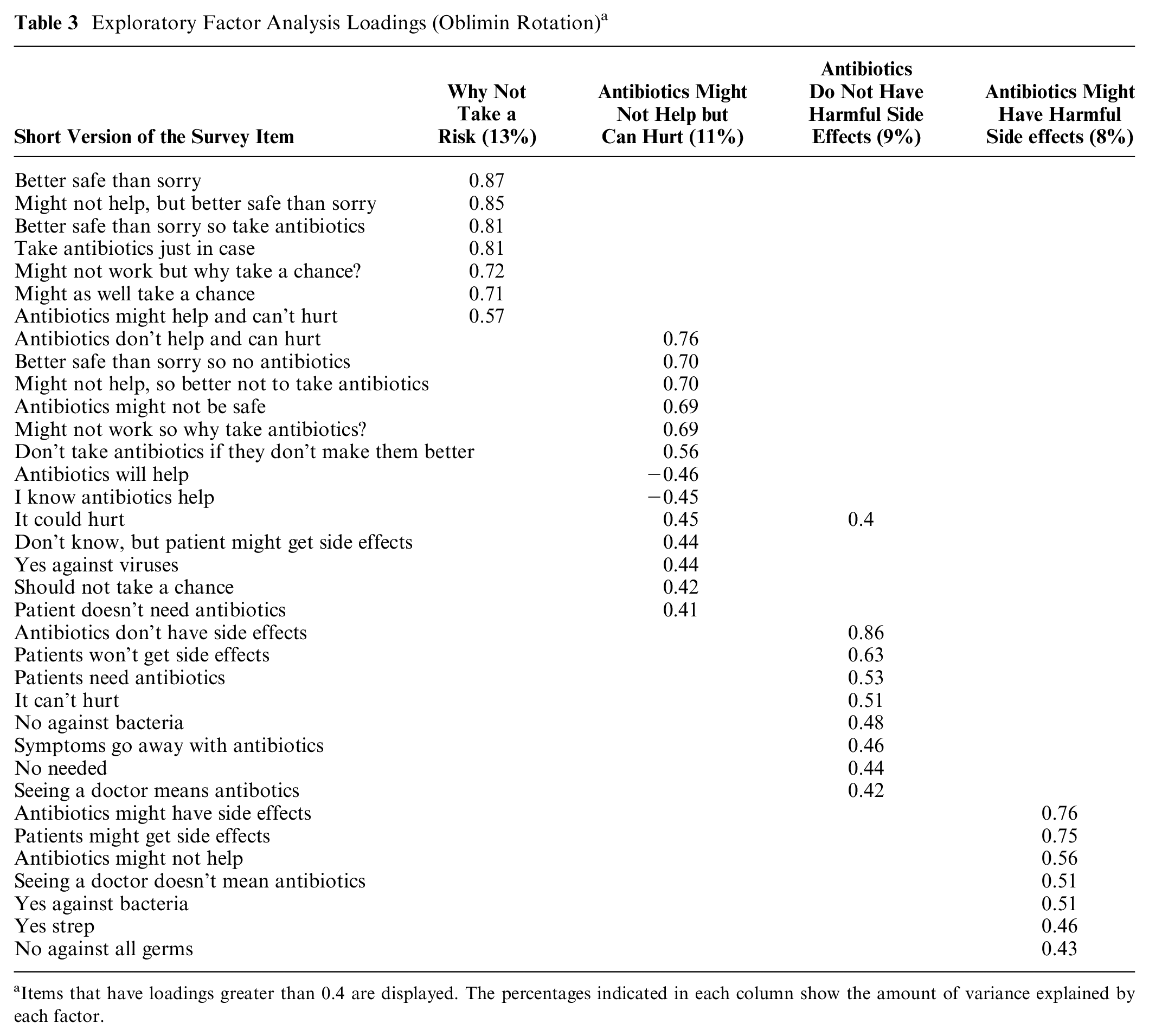
Items that have loadings greater than 0.4 are displayed. The percentages indicated in each column show the amount of variance explained by each factor.
Correlations among Gist Endorsements, Numeracy, NFC, Numerical Judgment, and Years of Experience

P < 0.001; **P< 0.01.
Hypotheses-Testing Results
Support for hypothesis 1: Clinical scenario predicts gist
Controlling for numeracy and NFC, endorsements of the “why not take a risk?” gist, F(2, 255) = 8.53, P < 0.001; the “antibiotics might not help but can hurt” gist, F(2, 255) = 5.14, P < 0.01; and the “antibiotics do NOT have harmful side effects” gist, F(2, 255) = 3.56, P < 0.05, but not the “antibiotics might have harmful side effects” gist, F(2, 255) = 1.56, P = 0.21), differed between decision scenarios. Regression analyses showed that, when comparing the “indicated” scenario to the “not indicated” scenario, the likelihood of endorsing the “why not take a risk” and “antibiotics do NOT have harmful side effects” gists decreased, and the likelihood of endorsing the “antibiotics might not help but can hurt” increased (Table 5). We did not observe any significant differences in gist endorsements between the “indicated” and “maybe indicated” scenarios for these gists (Figure 2). We also did not detect a statistically significant difference between providers’ estimates of the probability that patients would improve without antibiotics, F(2, 255) = 1.29, P = 0.27 (Figure 3), even when controlling for numeracy and NFC, F(2, 255) = 1.59, P = 0.20.
Regression Analysis Summary for Patient Scenarios Predicting Gist Factors a
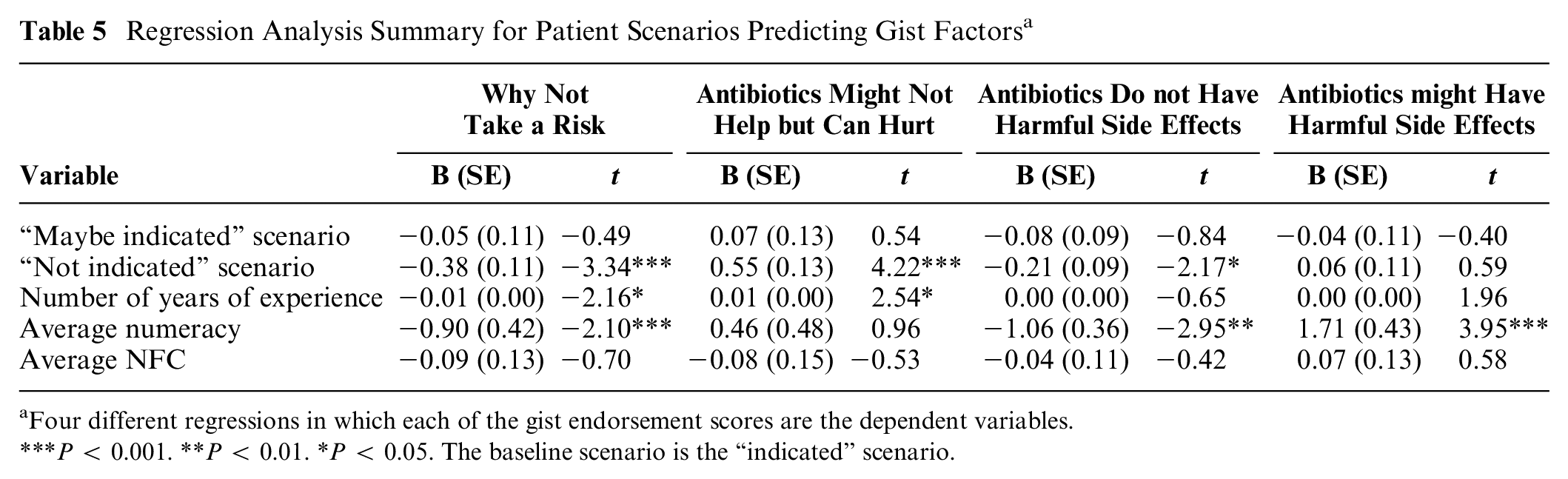
Four different regressions in which each of the gist endorsement scores are the dependent variables.
P < 0.001. **P < 0.01. *P < 0.05. The baseline scenario is the “indicated” scenario.
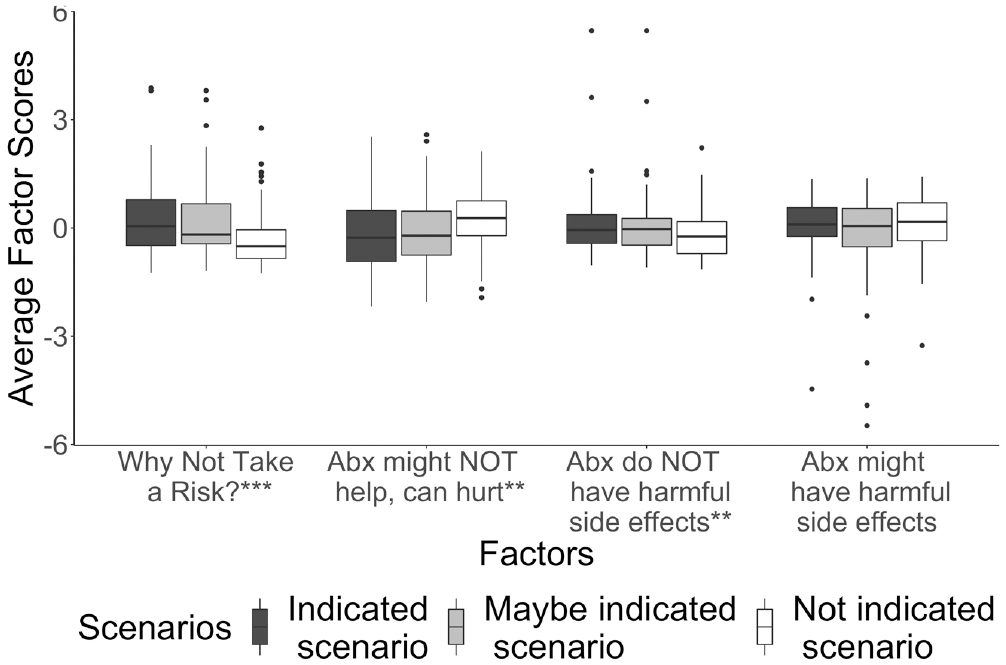
Average gist endorsements for each patient scenario. ***P < 0.001; **P < 0.01. The values of all variables are centered at zero and scaled. The zero exploratory factor analysis score represents the following: a disagreement with the average Likert score of 2.41 (i.e., disagree) for the “Why not take a risk” gist, neutrality with the average Likert score of 4.09 (i.e., neither agree nor disagree) for “the antibiotics might not help but can hurt” gist, agreement disagreement with the average Likert score of 6.17 (i.e., agree) for the antibiotics might have harmful side effects gist, and disagreement with the average Likert score of 2.01 (i.e., disagree) for “the antibiotics do not have harmful side effects” gist.

The vertical line shows the realization of the estimated probability of patient recovery without antibiotic treatment. Specifically, the probability of patients’ recovery under the “indicated scenario” is 40%, the probability of patients’ recovery under the “maybe indicated” scenario is 59%, and finally the probability of patients’ recovery under the “not indicated” scenario is 73%. Kolmogrov-Smirnov test results showed that the distributions are statistically indistinguishable from each other (D = 0.12, P = 0.47; D = 0.14, P = 0.31; D = 0.09, P = 0.81). Based on data from placebo-controlled randomized clinical trials,26,27 patients would improve without antibiotics (i.e., the proportion from the placebo group who improved) with 40% probability under the “indicated” scenario, 59% probability under the “maybe indicated” scenario, and 73% probability under the “not indicated” scenario.
Support for Hypothesis 2: Gist mediates the relationship between clinical scenario and antibiotic prescription decisions
Ordinal logistic regression results show that, controlling for the decision scenario, participants were significantly more likely to prescribe antibiotics if they endorsed the “why not take a risk?” and “antibiotics do not have harmful side effects” gist. On the other hand, they were more likely to choose not to prescribe antibiotics if they endorsed “antibiotics might not help but can hurt” and “antibiotics might have harmful side effects.” Moreover, we found that the relationship between the clinical scenario and prescription decision was mediated by endorsements of the “why not take a risk,” “antibiotics might not help but can hurt,” and “antibiotics do not have harmful side effects” gists (Figures 4–7). We did not detect a significant effect of verbatim risk estimate on prescription decisions (Appendix F).
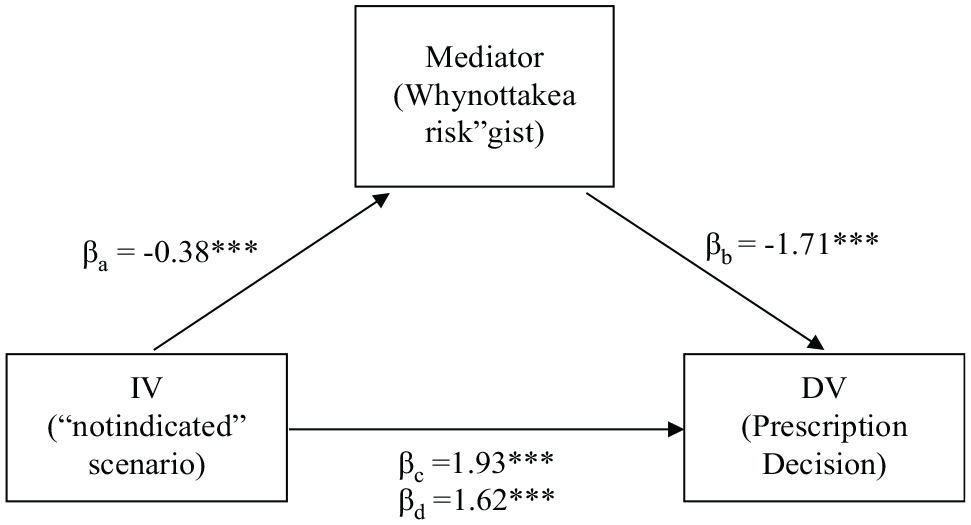
The mediation analysis for the “why not take a risk?” gist. * p < .05 **p < .01, ***p < .001. The independent variable IV, i.e., the “not indicated scenario” predicts the mediator gist in a linear regression (βa = -0.38, t=-3.34). The mediator predicts the dependent variable DV, i.e., prescription decision (βb =-1.71, t=-7.30) in an ordinal logistic regression. The “not indicated” scenario significantly predicts the decision (βc = 1.93, t= 5.46) and this effect is smaller when controlling for the mediating variable (βd =1.62, t=4.39).

The mediation analysis for the “Antibiotics might not help but can hurt” gist. * p < .05 **p < .01, ***p < .001. The independent variable IV, i.e., the “not indicated scenario” predicts the mediator gist in a linear regression (βa =0.55, t=4.22). The mediator predicts the dependent variable DV, i.e., prescription decision (βb =2.38, t=8.95). in an ordinal logistic regression. The “not indicated” scenario significantly predicts the decision (βc = 1.93, t= 5.46) and this effect is smaller controlling for the mediating variable (βd =1.54, t=3.88).

The mediation analysis for the “Antibiotics do not have harmful side effects” gist *p < .05 **p < .01, ***p < .001. The independent variable IV, i.e., the “not indicated scenario” predicts the mediator gist in a linear regression (βa =-0.21, t=-2.17). The mediator predicts the DV dependent variable, i.e., prescription decision (βb =-1.29, t=-5.23) in an ordinal logistic regression. The total effect of the “not indicated” scenario significantly predicts the decision (βc = 1.93, t= 5.46) and this effect is smaller when the mediating variable is included in the ordinal logistic regression (βd =1.78, t=4.97).

The mediation analysis for the “Antibiotics might have harmful side effects” gist. * p < .05 **p < .01, ***p < .001. The independent variable IV, i.e., the “not indicated scenario” is not a significant predictor of the mediator gist in the linear regression (βa =0.06, t=0.59, p=0.55). On the other hand, the mediator predicts the DV dependent variable, i.e., prescription decision (βb =0.76, t= 4.02) in an ordinal logistic regression. The total effect of the “not indicated” scenario significantly predicts the decision (βc =1.93, t= 5.46) and this effect remained the same when the mediator is included in the ordinal logistic regression (βd =1.93, t=5.43).
Support for hypothesis 3: less experienced clinicians tend to hedge in their antibiotic prescription decisions compared with more experienced clinicians.
According to fuzzy-trace theory, experts’ categorical thinking would lead them to avoid hedging and make decisions accordingly, whereas novices would tend to hedge more. 18 Logistic regression results show that participants are less likely to hedge as they become more experienced, controlling for scenario and gist endorsement, (B = −0.05, P = 0.001; Table 6). These results indicate that a clinician with 2.58 y of experience (1 standard deviation less than the mean of 12.19 y) is 2.61 times more likely to hedge than a clinician with 21.8 y of experience (possessing 1 standard deviation more experience than the mean of 12.19 y) regardless of clinical scenario. Furthermore, the average clinician was 5.41, 3.63, and 1.34 times more likely to hedge than not hedge, in the “indicated,” “maybe indicated,” and “not indicated” scenarios, respectively. Controlling for the number of years of experience, we did not detect any significant effect of professional title on the hedging tendency (Appendix G).
Logistic Regression Results Predicting Hedging Tendency

OR, odds ratio.
The outcome variable is a binary variable representing the hedging option, which is encoded as 1 if “maybe” option (watchful waiting) was chosen and 0 otherwise. The baseline experimental condition is the “indicated” scenario. In the sample where antibiotics are not indicated, hedging is associated with the number of years of experience (B = −0.04, P = 0.03).
P < 0.001. **P < 0.01.
Discussion
Fuzzy-trace theory predicts that clinicians will be more likely to prescribe when they endorse an individually rational, yet globally suboptimal, categorical gist that discounts potential harms from antibiotics yet acknowledges the possibility of benefit to the patient. In contrast, clinicians’ decisions should be relatively insensitive to verbatim representations of numerical probability estimates. Finally, these mental representations should be distinct. As predicted, risk estimates and gist factors were not significantly correlated.
Consistent with this prediction, subjects endorsing the “why not take a risk?” and “antibiotics do not have harmful side effects” gists were significantly more likely to prescribe antibiotics, controlling for decision scenarios. Subjects endorsing the “antibiotics might not help but can hurt” and “antibiotics might have harmful side effects” gists were less likely to prescribe. As in prior work, these contradictory gists were not correlated in the EFA, suggesting that subjects can endorse both at the same time.
Furthermore, we found significant differences across patient scenarios in endorsements of all 4 gists, highlighting the context-specific nature of gist representation. Patient scenarios influenced gist representations, which then influenced prescription decisions. However, verbatim risk estimates did not change with the decision scenario. This highlights that gist is context specific whereas verbatim representations are decontextualized.
One might argue that this may suggest a possible knowledge deficit when it comes to precise probability estimates, but these estimates were not associated with prescription decisions. This suggests that interventions that aim to fill a knowledge deficit may be insufficient, on their own, to change behaviors. Rather, behaviors were associated with endorsement of gist representations. Prior work showed that communicating gist to both patients and providers helps improve the decision-making processes in various domains and with respect to different expertise levels.28–31 In this case, our results pertain to communicating the gist to providers; however, future work could examine whether gist communications could also be designed to address parents’ concerns. Furthermore, gist endorsement and verbatim risk estimates were not significantly correlated, supporting the distinct contributions of these mental representations.
Finally, consistent with fuzzy-trace theory’s predictions, we found that more experienced clinicians were less likely to “hedge,” as predicted by Reyna and Lloyd. 22 Because most patients with AOM do eventually improve without antibiotics, “watchful waiting” is frequently an appropriate option, and it is endorsed by the American Academy of Pediatrics for most children with AOM. This option involves discussing with patients’ families the risks and benefits of antibiotics and opting to observe without antibiotics for 2 d but with establishment of a contingency plan that includes antibiotic prescriptions if the patient’s symptoms worsen or do not improve. According to fuzzy-trace theory, application of this modal option would be favored by novices, but not by experts, even when immediate antibiotics are clearly indicated or are obviously not indicated. 22 Notably, physicians must apply their expertise to individual cases to determine when “watchful waiting” is appropriate. Given that the specific gists studied in this work predict hedging, future work should explore the role of experience beyond these specific gists. According to fuzzy-trace theory, expertise facilitates gist extraction. 11 This finding suggests that more experienced clinicians better contextualized patient scenarios, deciding on when to rely on “why not take a risk?” As shown by prior research, expertise-based gist facilitates contextualizing relevant information.11,15,22 This suggests that expertise is more than knowing about the negative consequences of antibiotics; rather, it is knowing when to say “why not take a risk?” That is, experts are not simply those who “know,” rather they are the ones who know how to use what they know in an appropriate context.
Limitations
In practice, the “watchful waiting” approach may or may not be accompanied by a “delayed prescription,” in which the patient would be prescribed a postdated antibiotic with instructions to the patient and/or pharmacist for the prescription to be filled only if the patient does not improve in 2 d. The option for watchful waiting in the scenarios presented did not specify this option would include delayed prescribing; as watchful waiting is a recommended practice for AOM, it is debatable whether this option should be considered hedging for AOM. However, our “not indicated” scenario described the exam of a child with OME (not AOM), a condition for which antibiotics are never indicated according to consensus guidelines. Similarly, our “indicated” scenario described a condition for which consensus guidelines recommended immediate antibiotics; nevertheless, we observed increased hedging by novices in both of these scenarios (Table 6).
One might also argue that there could be a generational shift in attitudes toward prescribing and that this shift toward antibiotic stewardship among younger prescribers explains why these younger prescribers are less likely to prescribe. However, as above, this alternative explanation does not account for the fact that younger prescribers were more likely to hedge, even in circumstances in which antibiotics were not indicated (Table 6). Rather, our data are consistent with fuzzy-trace theory’s predictions, which replicate across settings as diverse as cardiac surgery 22 and even intelligence analysis. 32
Conclusions
It is crucial to understand clinicians’ judgments about antibiotic risk, a serious threat to public health. Some programs may operate on the assumption that overprescription is rooted in knowledge deficits; however, our research shows that mental representation drives judgments about prescriptions. Therefore, it is necessary to explore the underlying factors that drive clinicians’ mental representations. Antimicrobial stewardship programs could also benefit from addressing the evidence that showed that all participants underestimated the probability of recovery when the symptoms do not indicate antibiotic treatment
Our findings support fuzzy-trace theory’s predictions. Results also suggested that clinicians’ prescription decisions were indistinguishable in the scenario in which antibiotics are certainly indicated and that in which antibiotics simply may be indicated.
Limitations of our study include that our sample may not be representative of all providers. Future work could extend this study into other provider settings while testing the ways in which guidelines for clinicians can be designed more effectively by focusing on communicating categorical gists.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683221115416 – Supplemental material for Gist Representations and Decision-Making Processes Affecting Antibiotic Prescribing for Children with Acute Otitis Media
Supplemental material, sj-docx-1-mpp-10.1177_23814683221115416 for Gist Representations and Decision-Making Processes Affecting Antibiotic Prescribing for Children with Acute Otitis Media by Deniz Marti, Rana F. Hamdy and David A. Broniatowski in MDM Policy & Practice
Footnotes
Acknowledgements
The authors wish to acknowledge Thomas A. Mazzuchi and Roger Cooke for their useful feedback and support for the research design. The authors also gratefully acknowledge the assistance of Kelly Rickard, Melody Fung, Laura Rogers, and GWU’s Consumer Health Antibiotic Stewardship Working Group for their support in subject recruitment. Finally, the authors thank the leaders of SPUC, Pediatric Health Network, Pediatric Urgent Care Providers Network.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the GW School of Engineering and Applied Science.
Ethical Approval
The study was approved by the GWU Institutional Review Board (No. 191875).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.